Downloaded 33 times

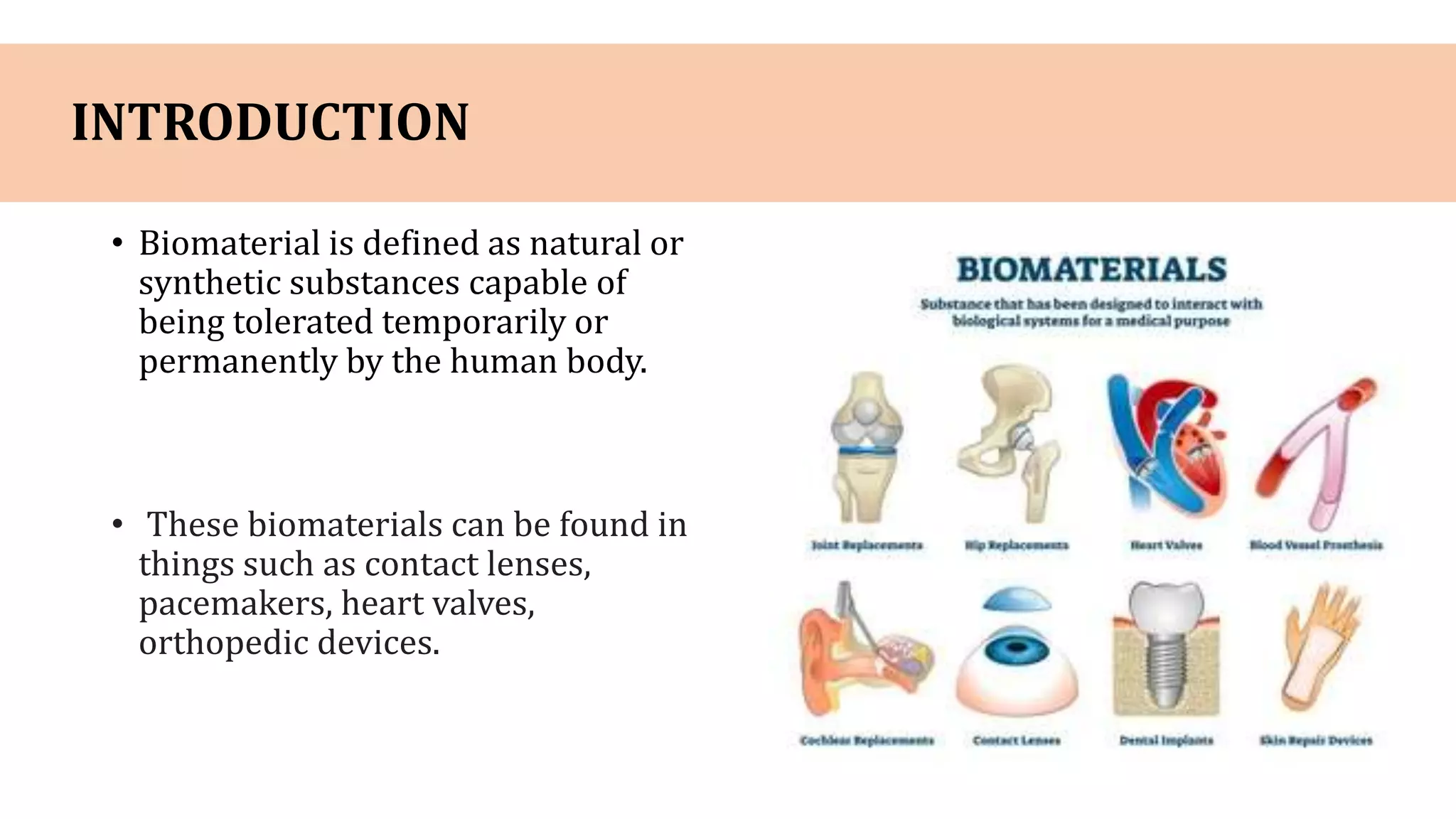




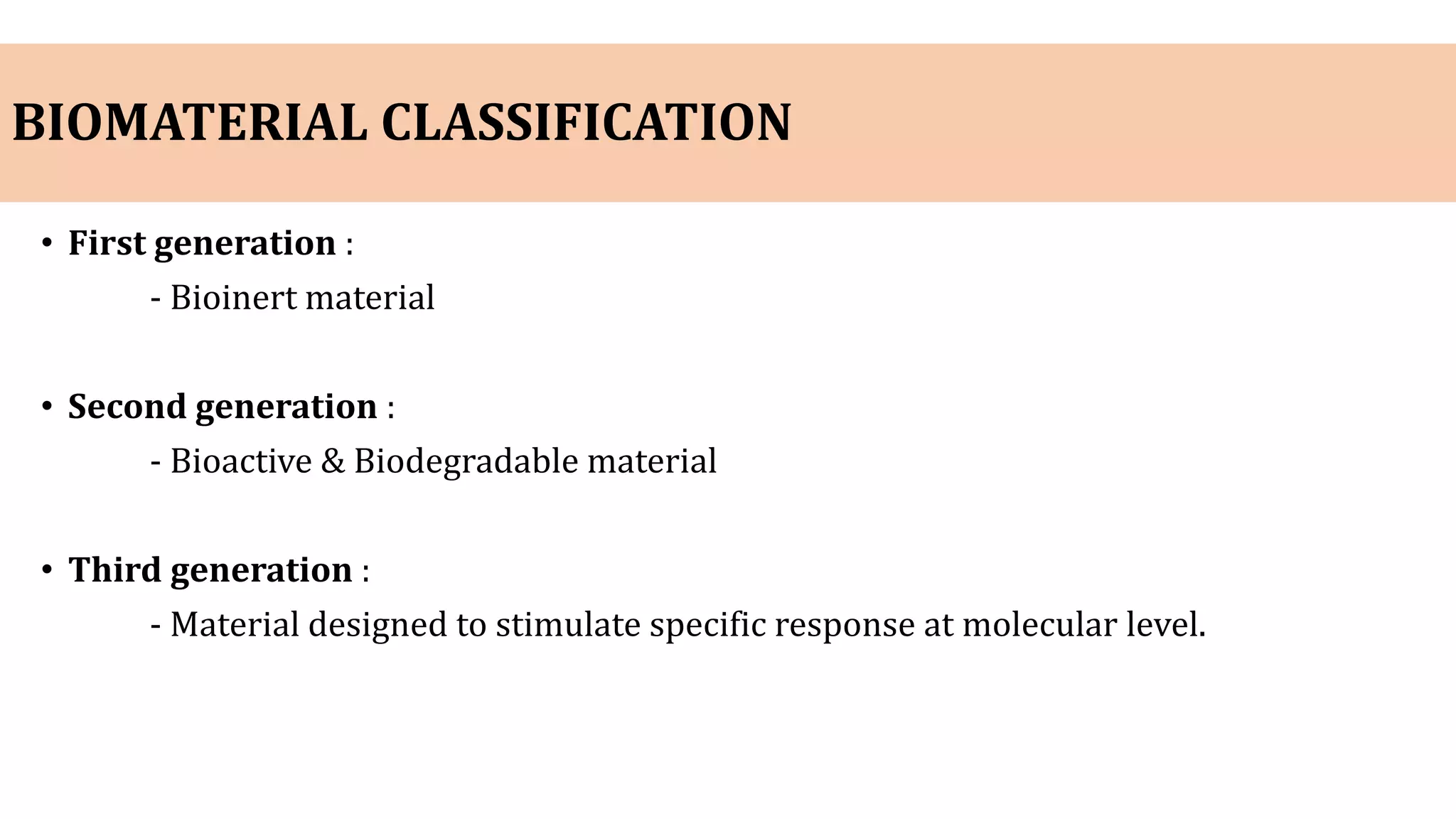

































Biomaterials are natural or synthetic substances that can be tolerated by the human body and are commonly used in orthopedic devices. There are three generations of biomaterials: first generation are bioinert materials, second generation are bioactive and biodegradable, and third generation stimulate specific cellular responses. Common biomaterial classes used in orthopedics include metals and alloys, ceramics, tissues adhesives, polymers, and carbon materials. Metals such as stainless steel, titanium, and cobalt chrome alloys are often used due to their strength and biocompatibility. Ceramics like alumina and zirconia are hard and brittle with high compressive strength. Complications can include infection, loosening





















































![SOFT TISSUE INJURY [Recovered].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/classificationofsofttissueinjuryrecovered-220424142623-thumbnail.jpg?width=640&height=640&fit=bounds)

























