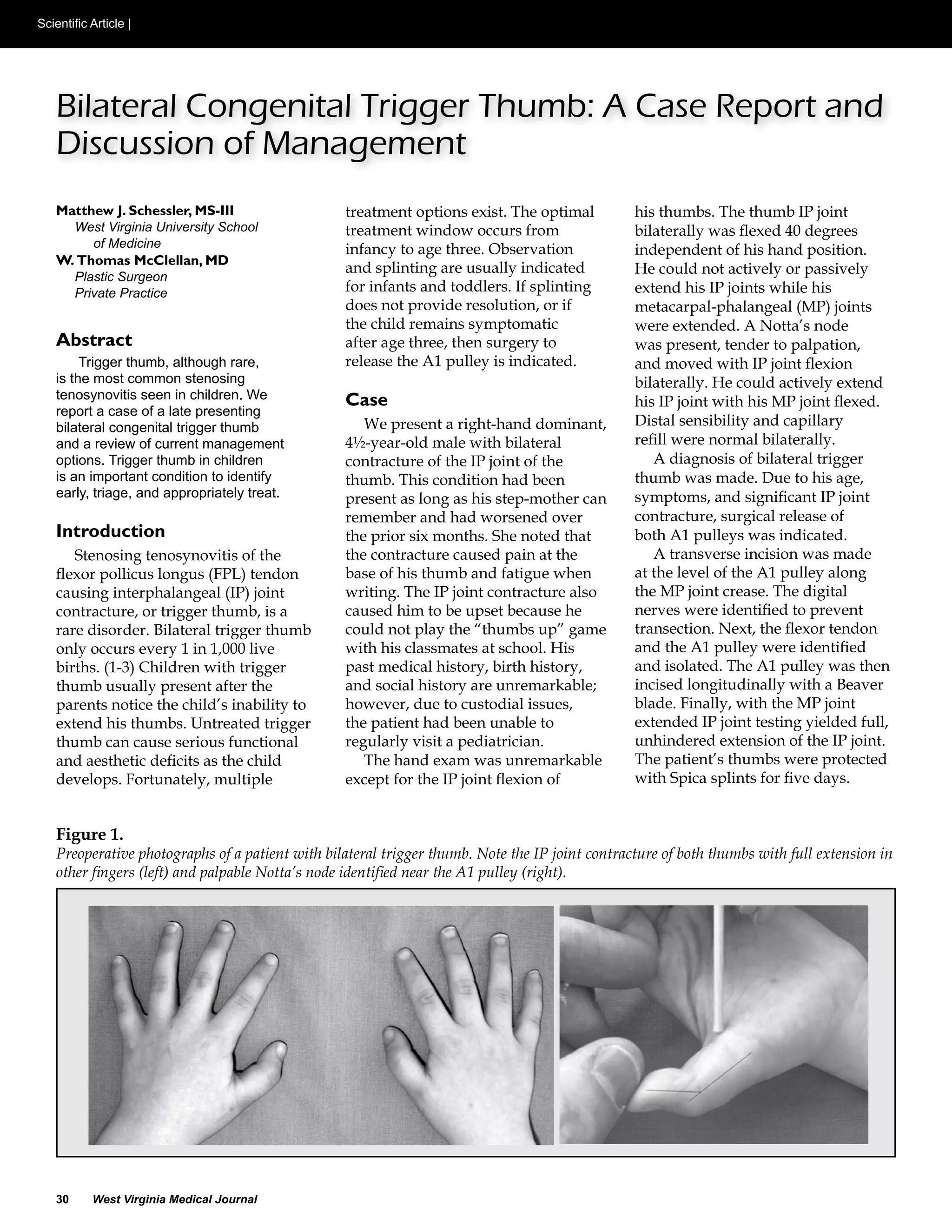
This case report describes a late presenting case of bilateral congenital trigger thumb in a 41⁄2-year old male. Trigger thumb is rare in children but most commonly affects the thumb. Early identification and treatment between ages 0-3 is important to allow for optimal development of hand function. While splinting is usually first-line for young children, the patient's persistent symptoms after 6 months of splinting indicated surgical release of the A1 pulley on both thumbs. At 3-month follow-up the patient had full extension of both thumbs with no complications. Surgical release is effective for refractory pediatric trigger thumb cases.













![Osteoarticular tuberculosis [bone and joint tb] dr mohamed ashraf,hod orthopa...](https://cdn.slidesharecdn.com/ss_thumbnails/osteoarticulartuberculosisboneandjointtbdrmohamedashrafhodorthopaedicsgovttdmedicalcollegealleppeyke-200910130018-thumbnail.jpg?width=640&height=640&fit=bounds)



















































































