Downloaded 16 times
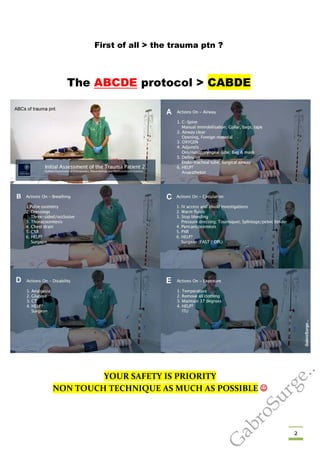
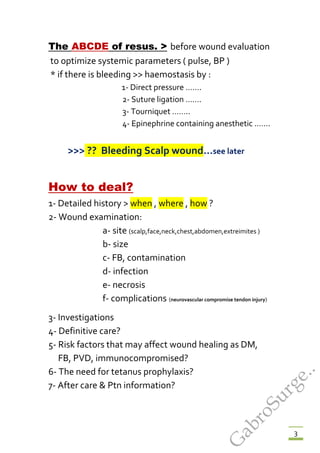

















The document provides guidance on basic wound management. It outlines the ABCDE protocol for initially assessing a trauma patient and controlling bleeding. It then describes in detail how to clean, debride, close and provide post-operative care for different types of wounds, including through suturing techniques. Specific wound locations like the face, eyes and joints are addressed. Proper wound closure and follow-up are emphasized to prevent complications and support proper healing.

































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











