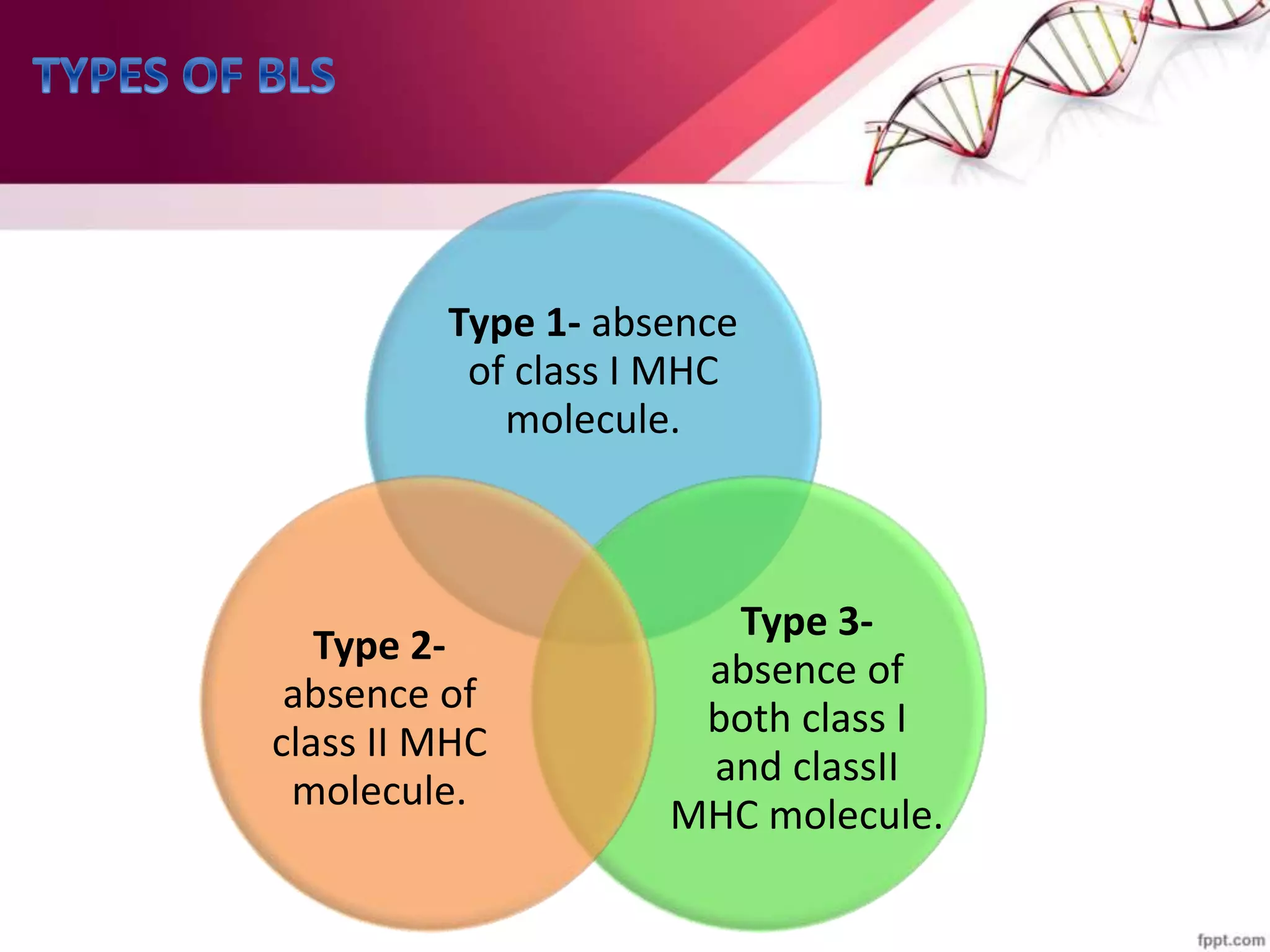
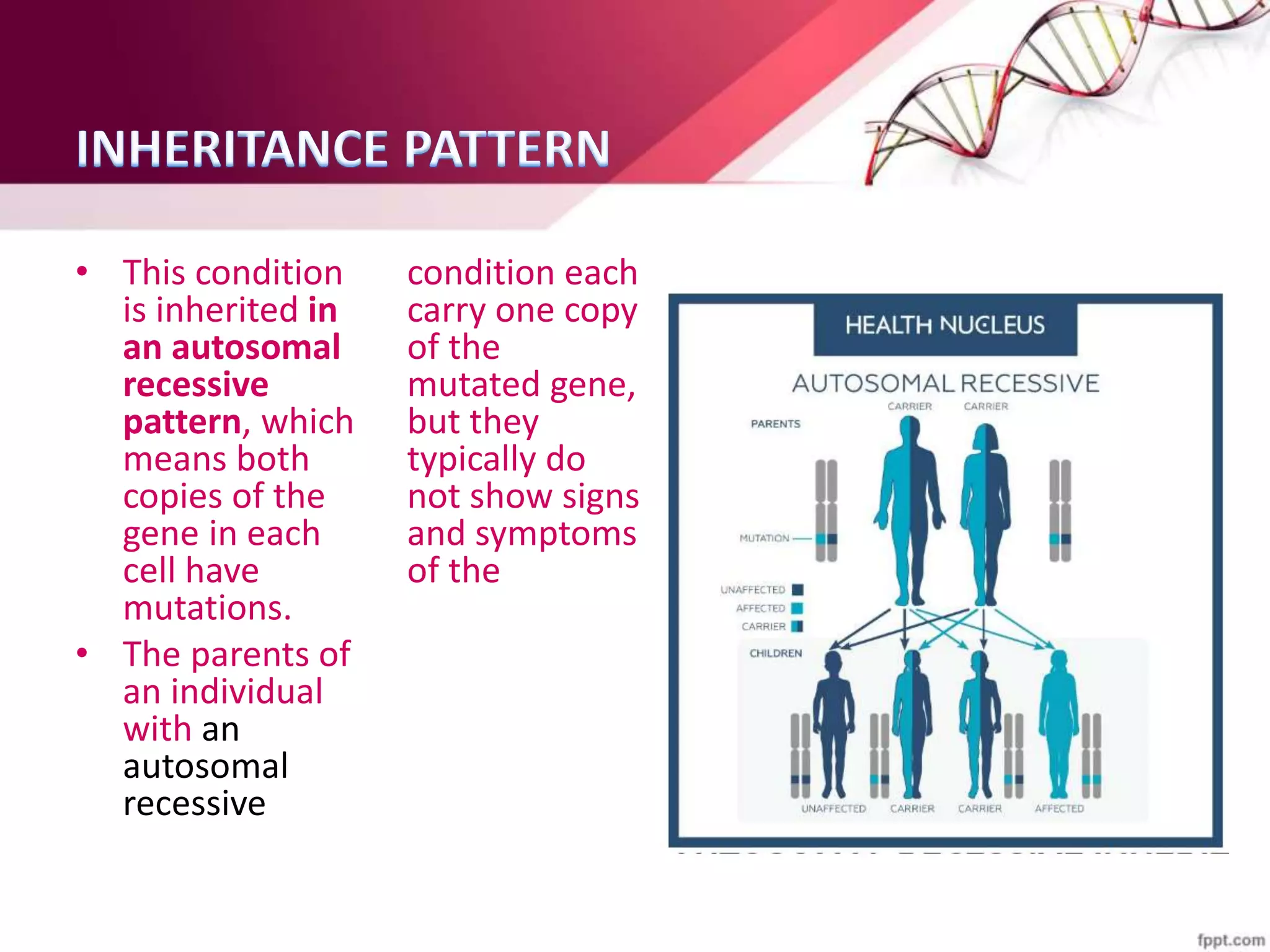
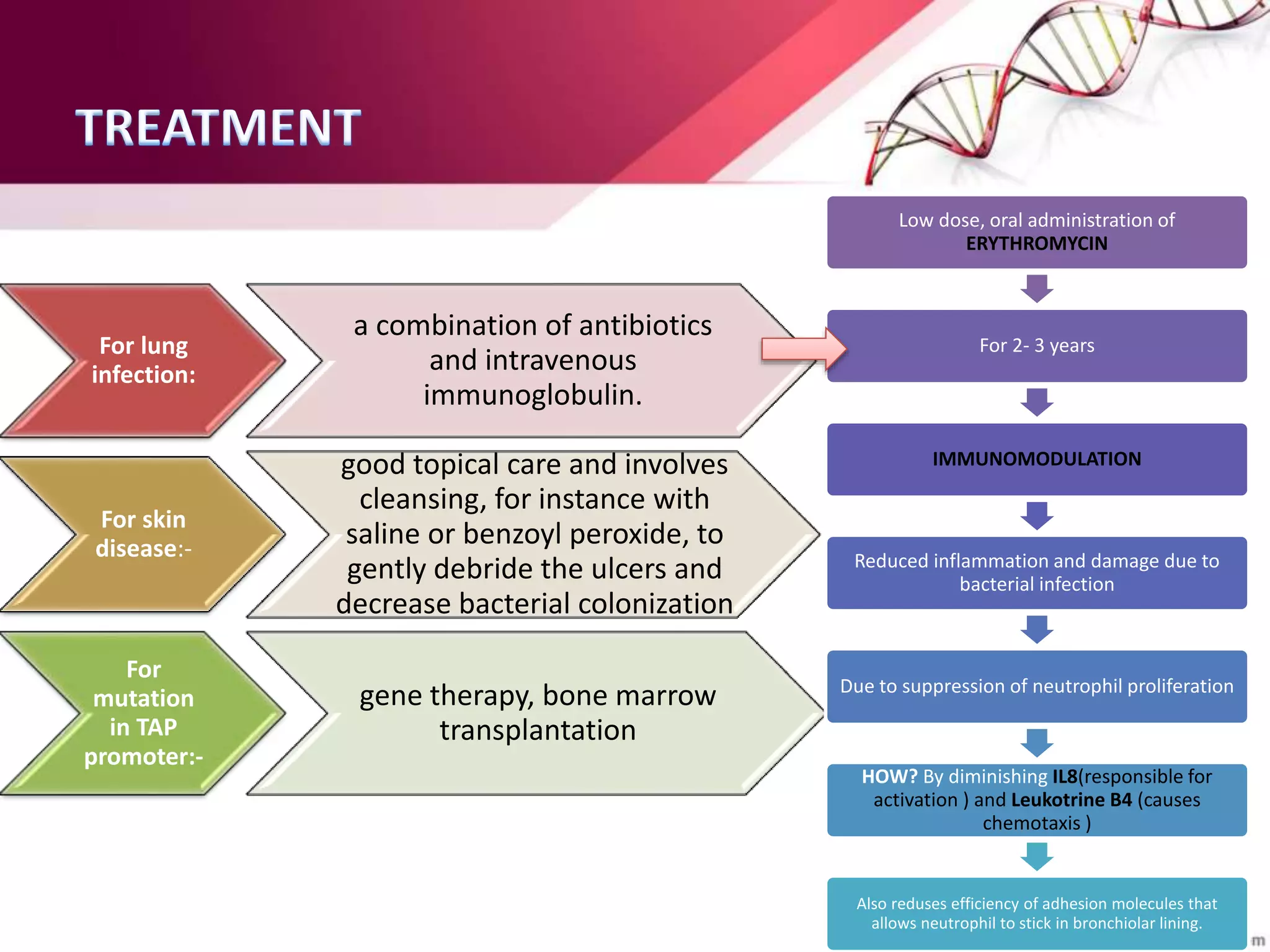
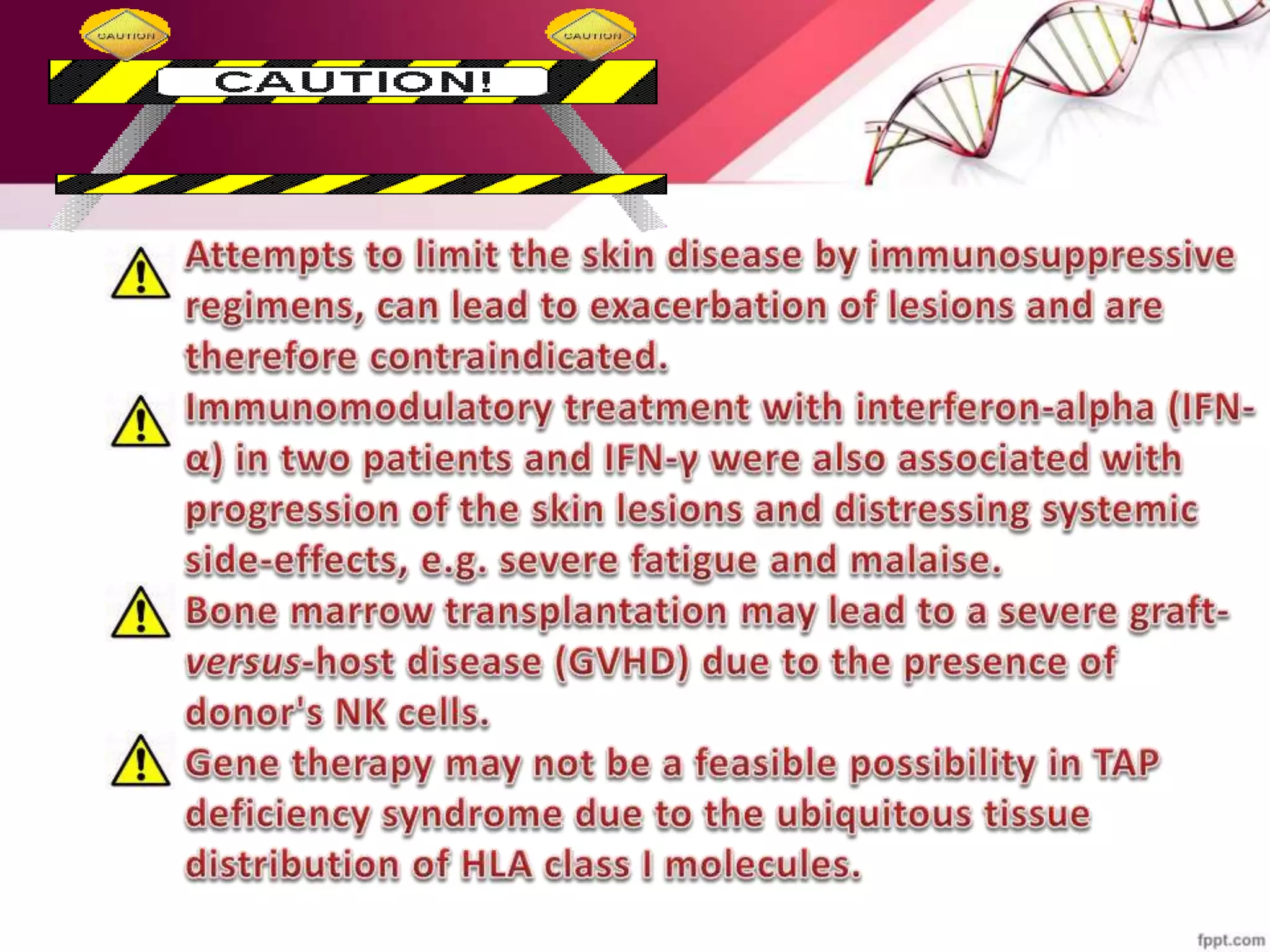
BLS (Bare Lymphocyte Syndrome) is a rare genetic immuno-deficiency disorder characterized by the absence of MHC or HLA on lymphocytes, leading to a fragile immune system similar to SCID. It is caused by mutations in genes related to MHC class I and II molecules, resulting in cellular abnormalities such as increased NK and γδ T cells while decreasing CD8+ αβ T cells. The condition is inherited in an autosomal recessive pattern and can lead to severe infections, requiring treatments like antibiotics, immunoglobulin, and potentially gene therapy or bone marrow transplantation.

































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)














