Downloaded 26 times
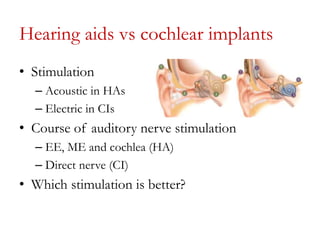
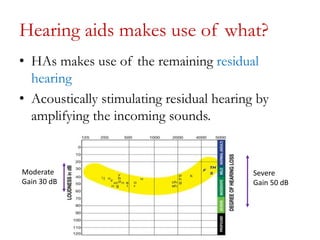
This document discusses cochlear implant candidacy criteria. It provides a brief history of cochlear implants and statistics on implants performed. It describes the differences between hearing aids and cochlear implants. Medical and audiological candidacy criteria for adults and children are outlined for different cochlear implant manufacturers based on FDA guidelines. Audiological tests used to assess candidacy and benefit from hearing aids are mentioned. The roles of various professionals on the cochlear implant team are highlighted.






























![Recent_Advances_Cochlear_Implant_Candidacy_Dr_Anand_Gupta[1]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/recentadvancescochlearimplantcandidacydranandgupta1-1-251128040227-e519dadb-thumbnail.jpg?width=640&height=640&fit=bounds)





![cochlear implant [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cochlearimplantautosaved-230807191245-e9fc2957-thumbnail.jpg?width=640&height=640&fit=bounds)






























