The document discusses the phases of partial denture service, including:
1) Educating the patient on proper use and maintenance to ensure success.
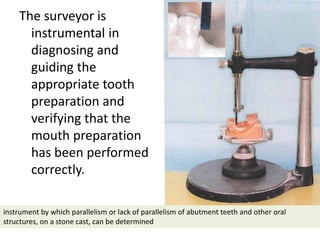
2) Diagnosing needs, treatment planning, designing the denture, and preparing the mouth.
3) Ensuring adequate support for distal extension denture bases by recording the ridge form under load.
4) Verifying occlusal relations and tooth arrangements after framework fitting.
5) Initial placement and ensuring occlusal harmony before giving the denture to the patient.
6) Periodic recall exams to monitor oral health and the need for maintenance.