Download to read offline

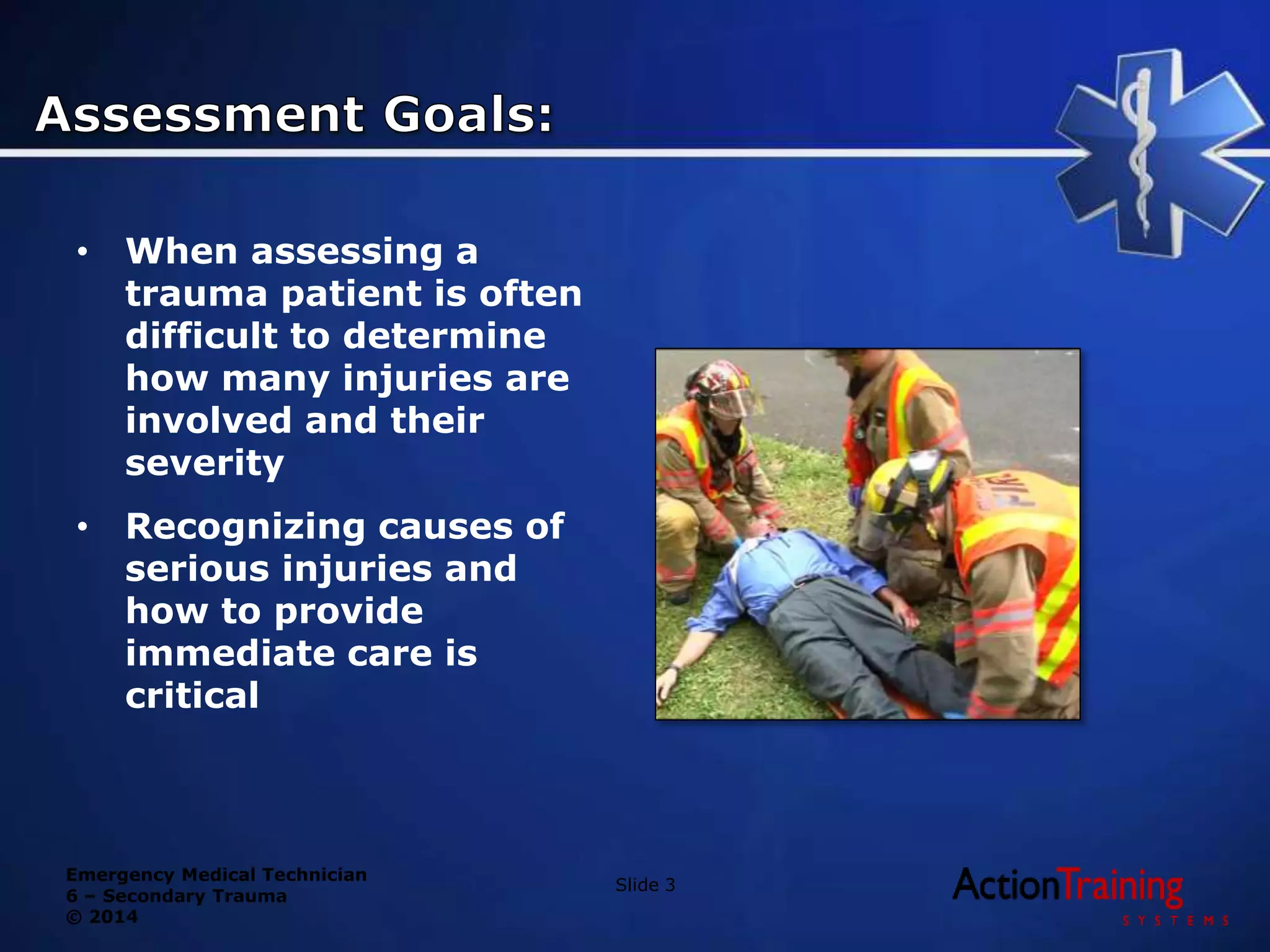


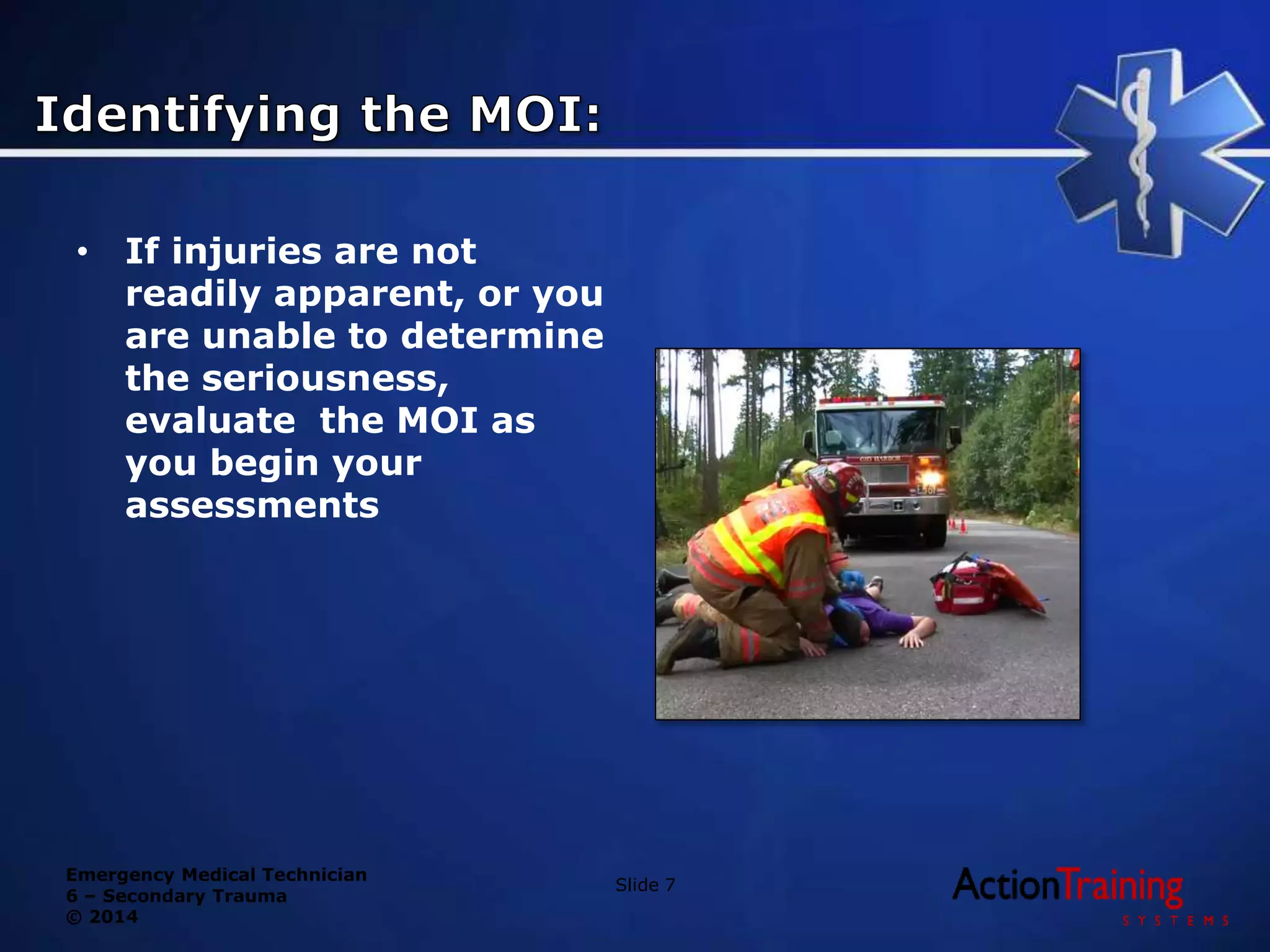











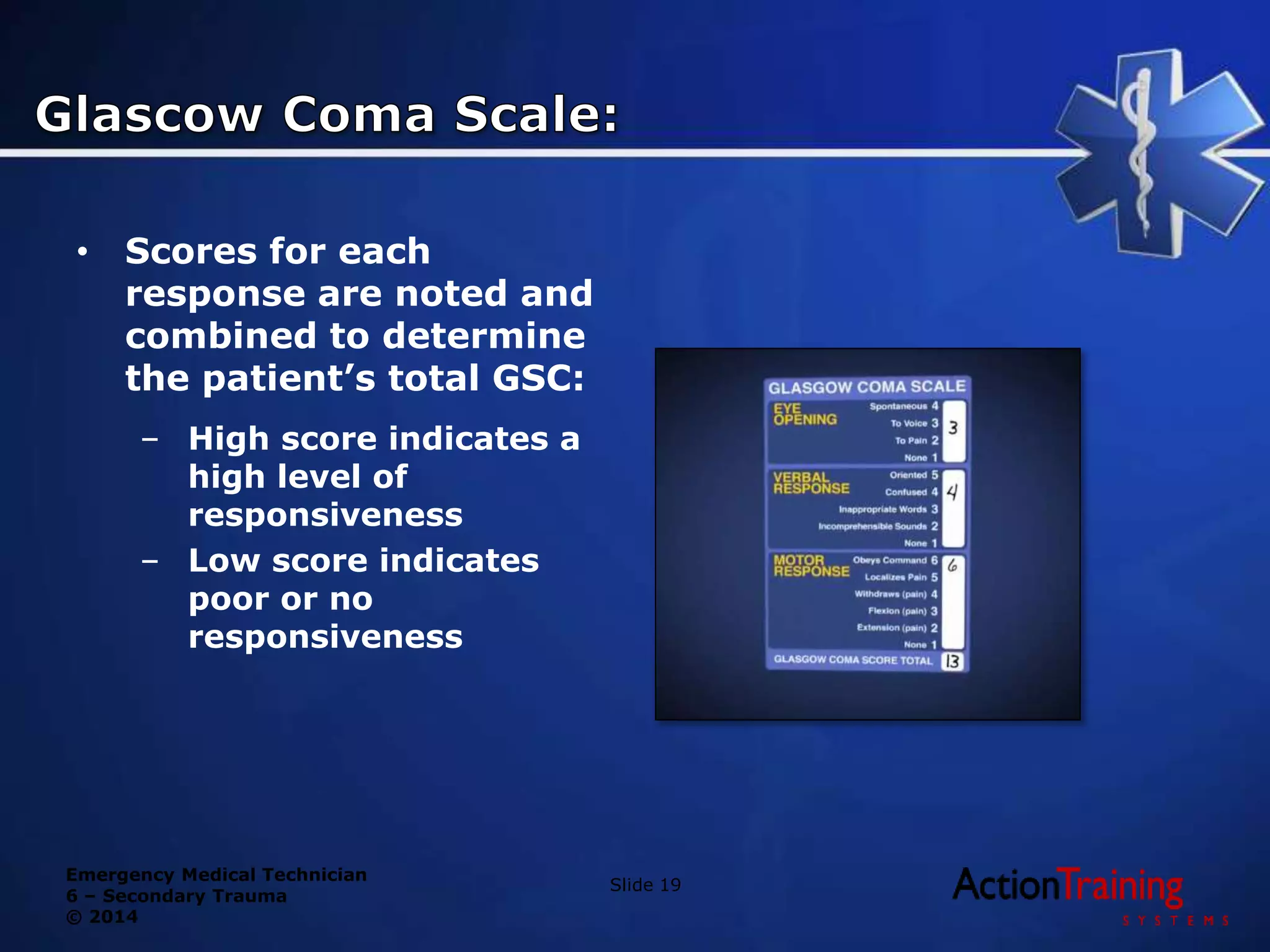

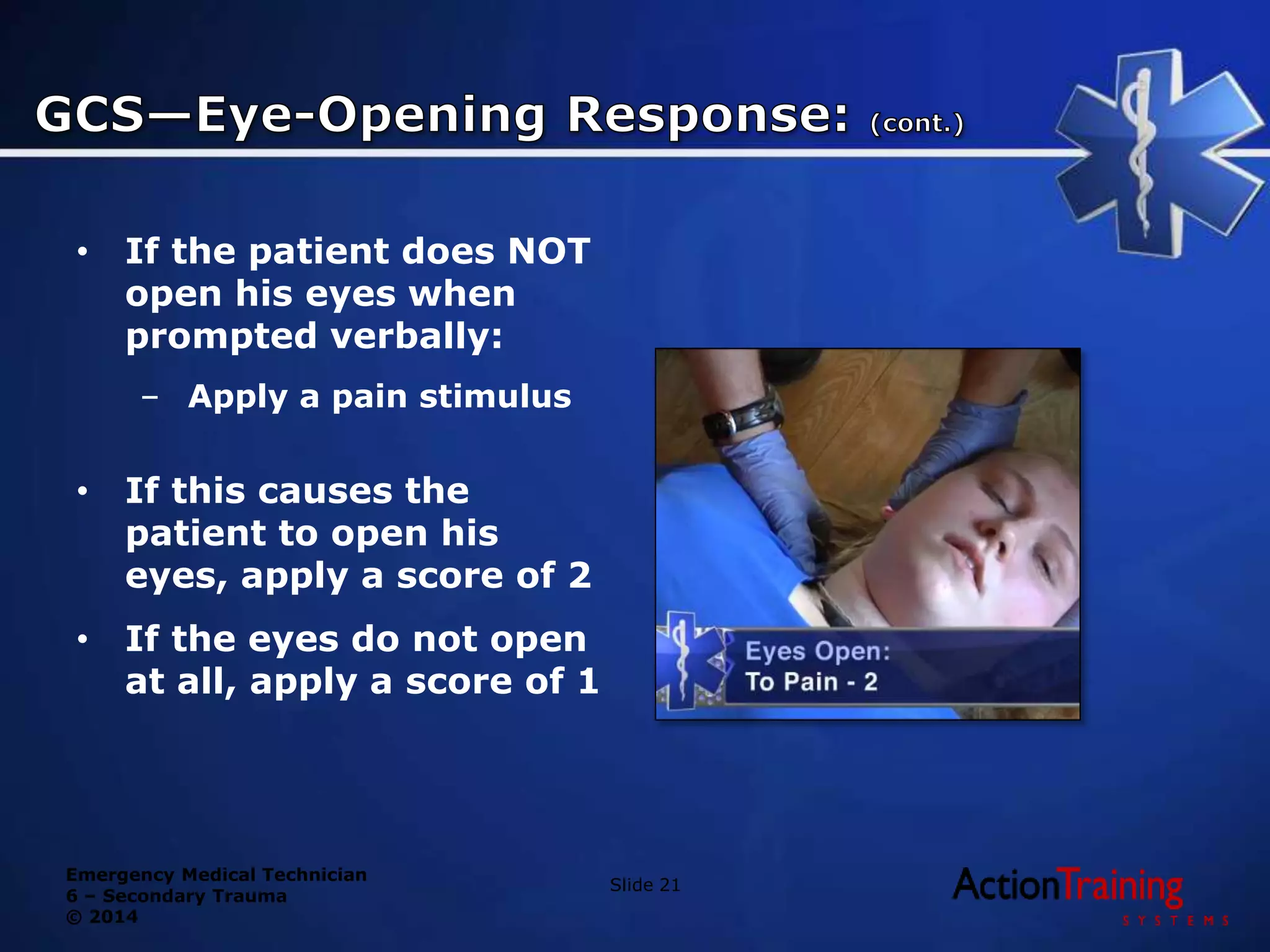
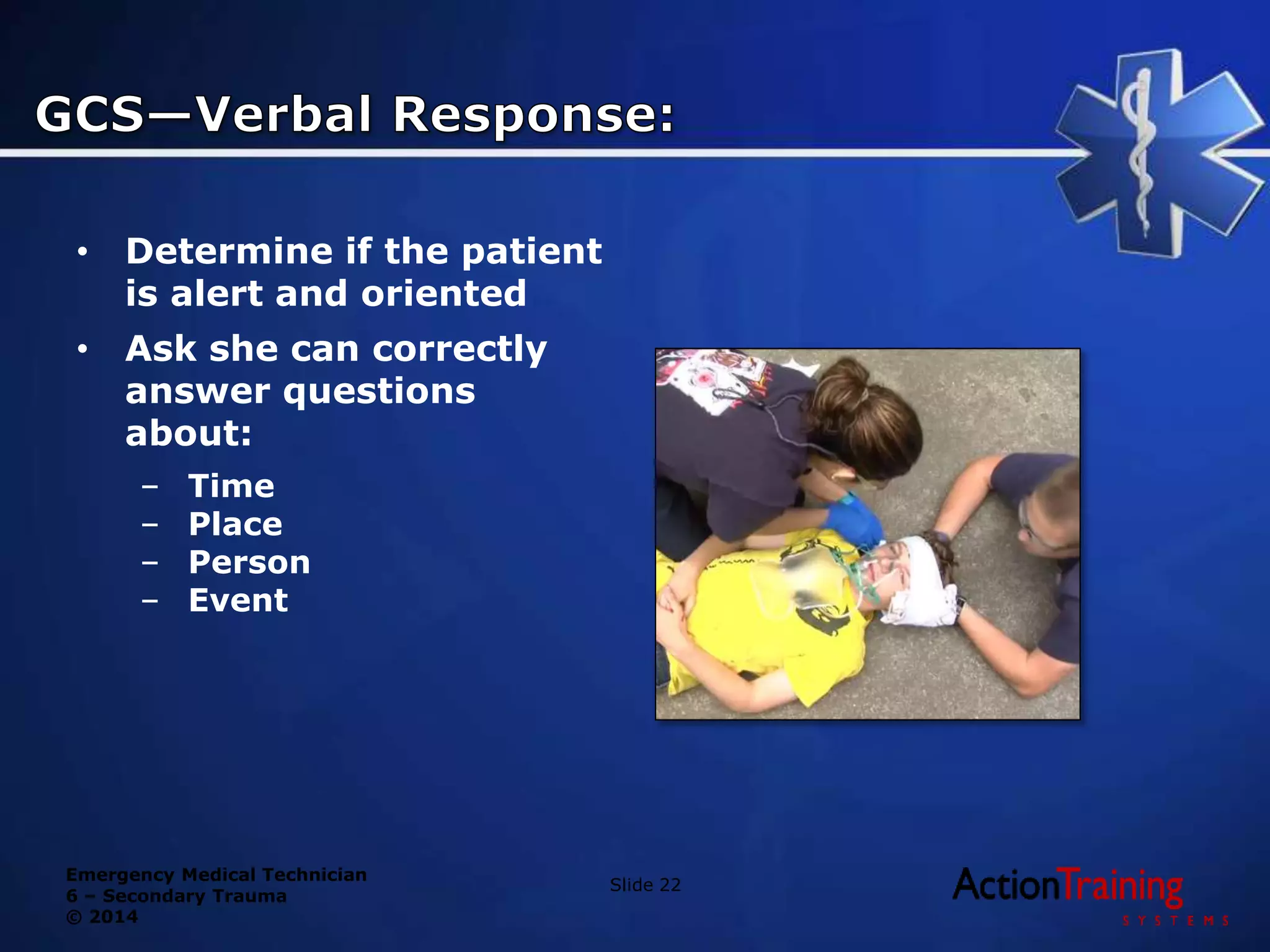



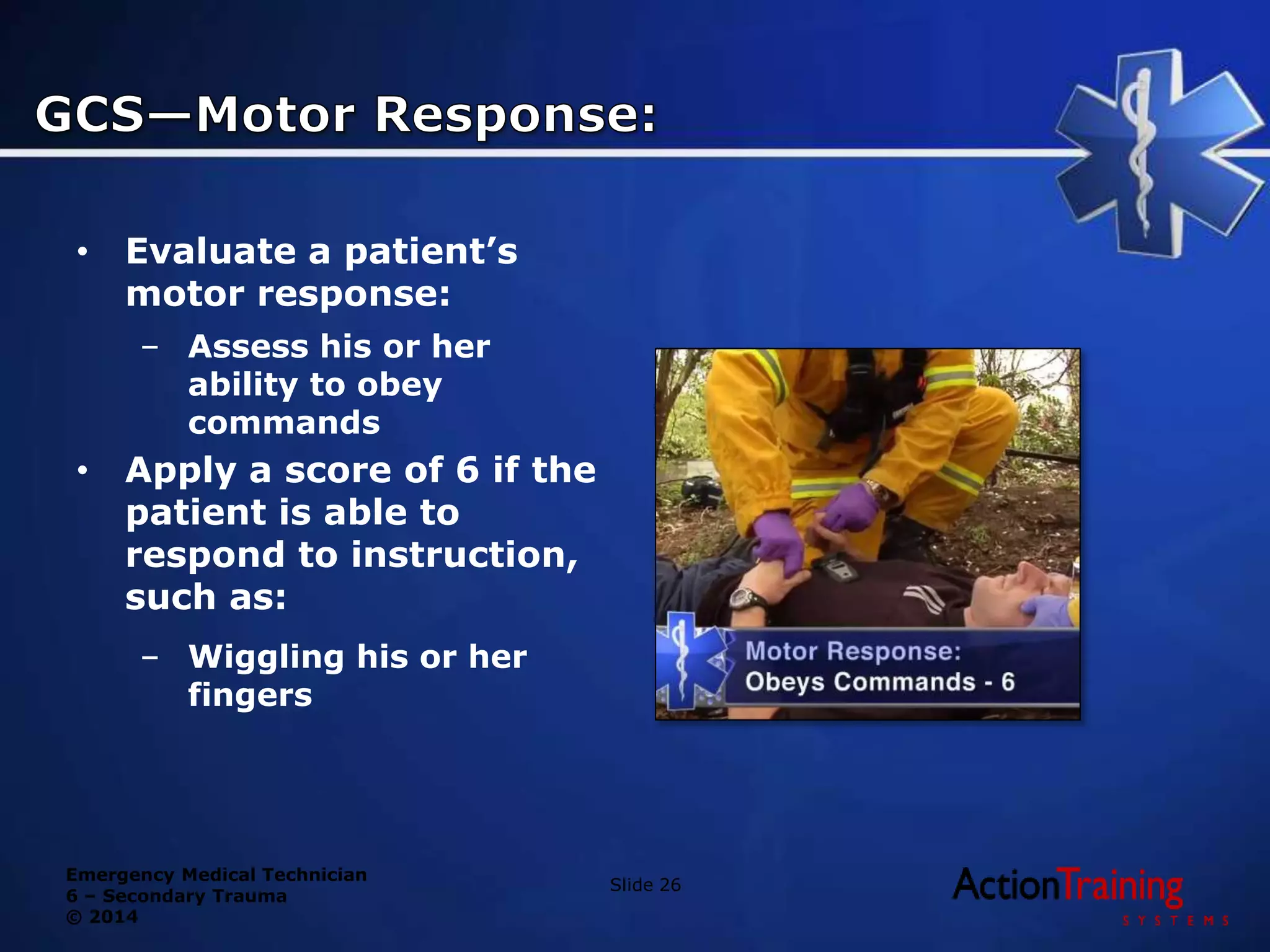

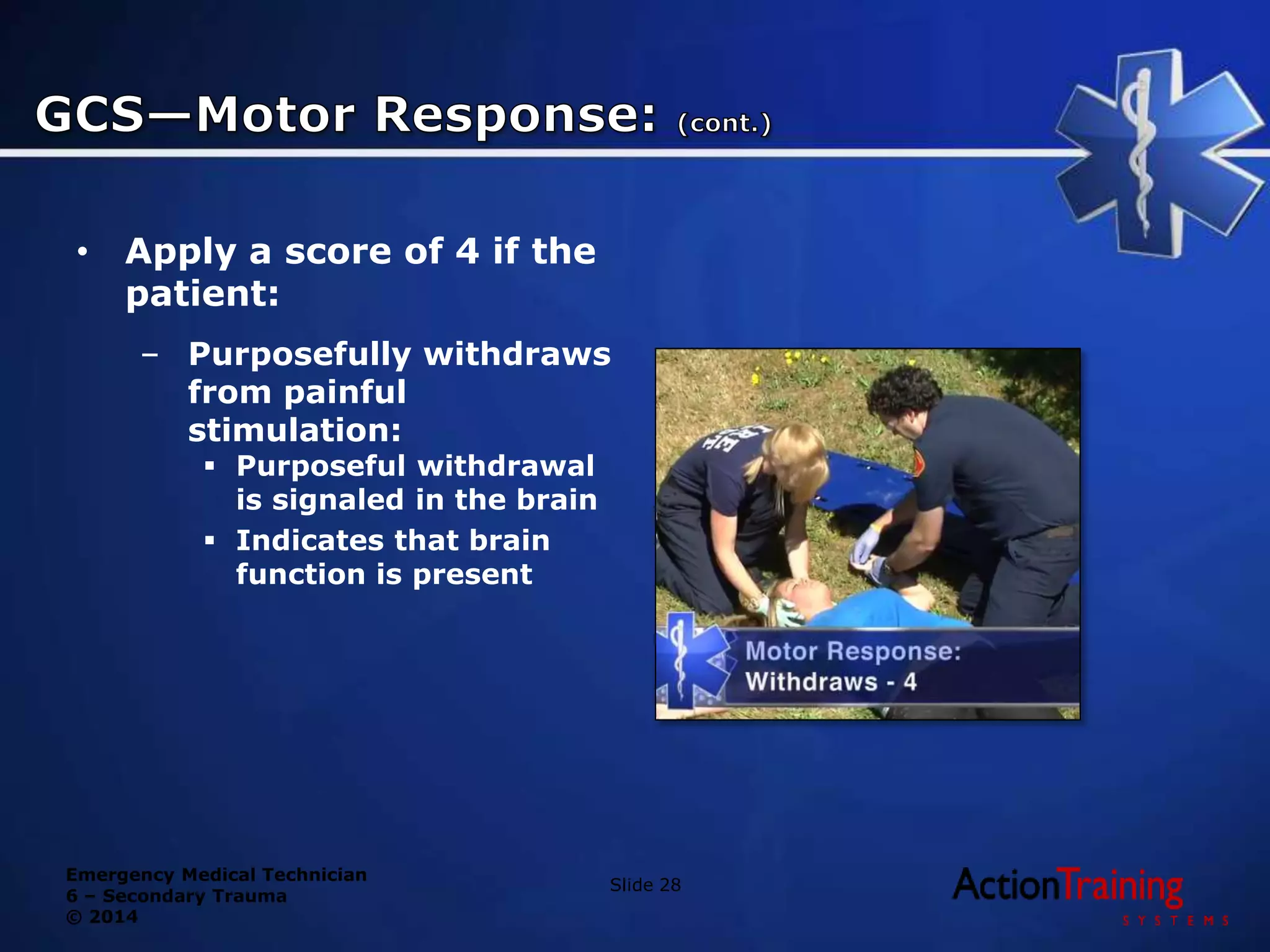


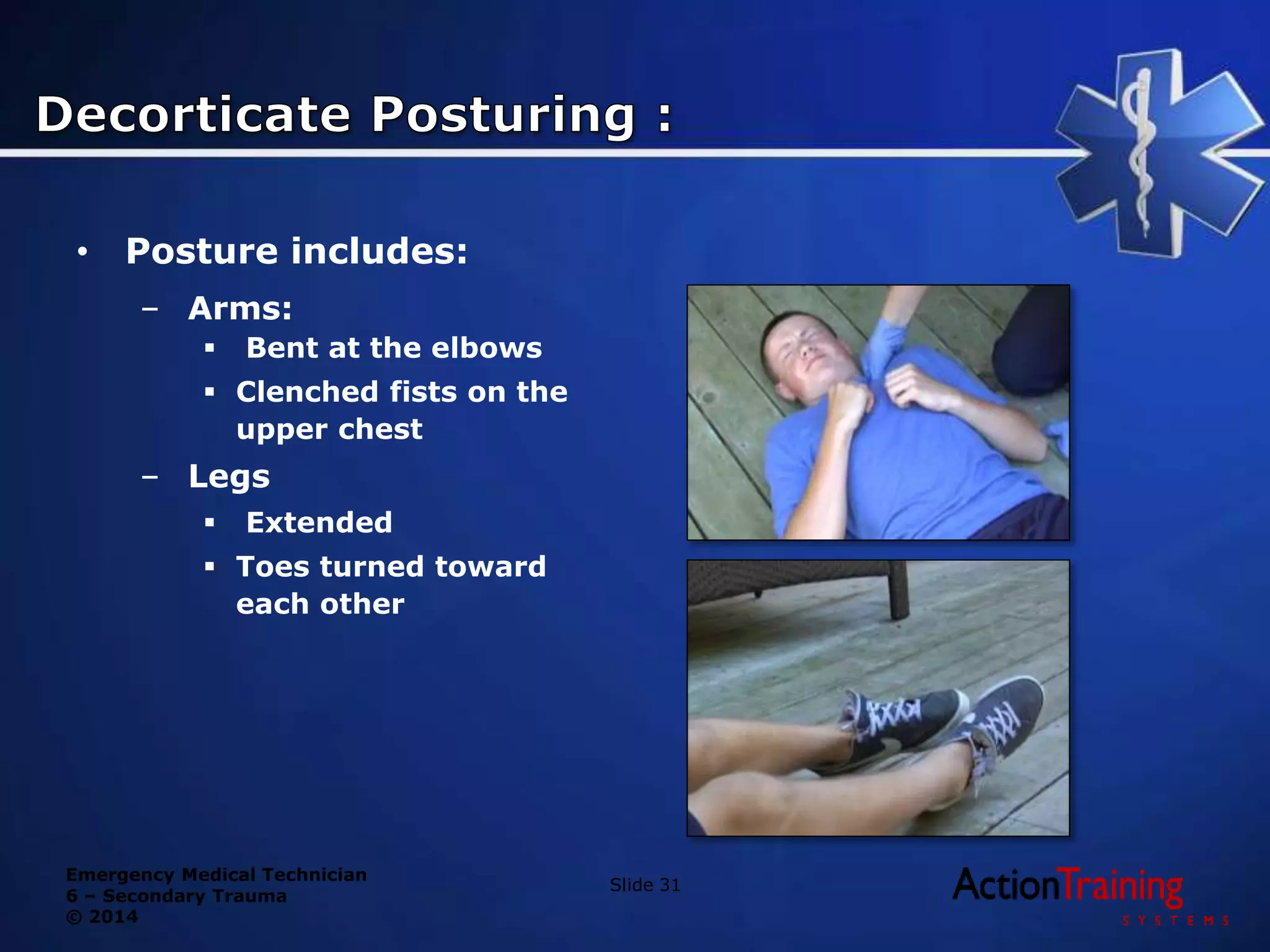
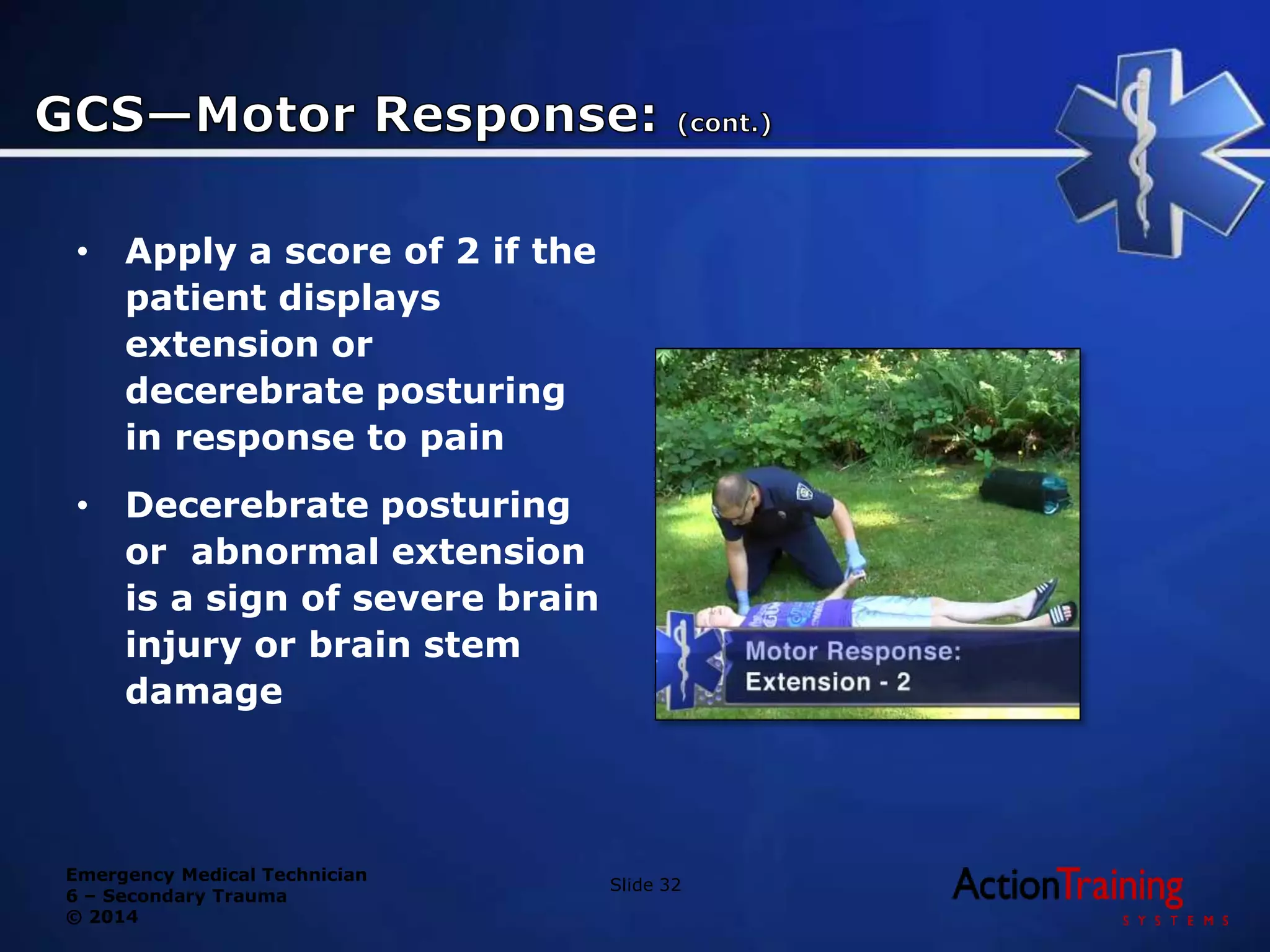

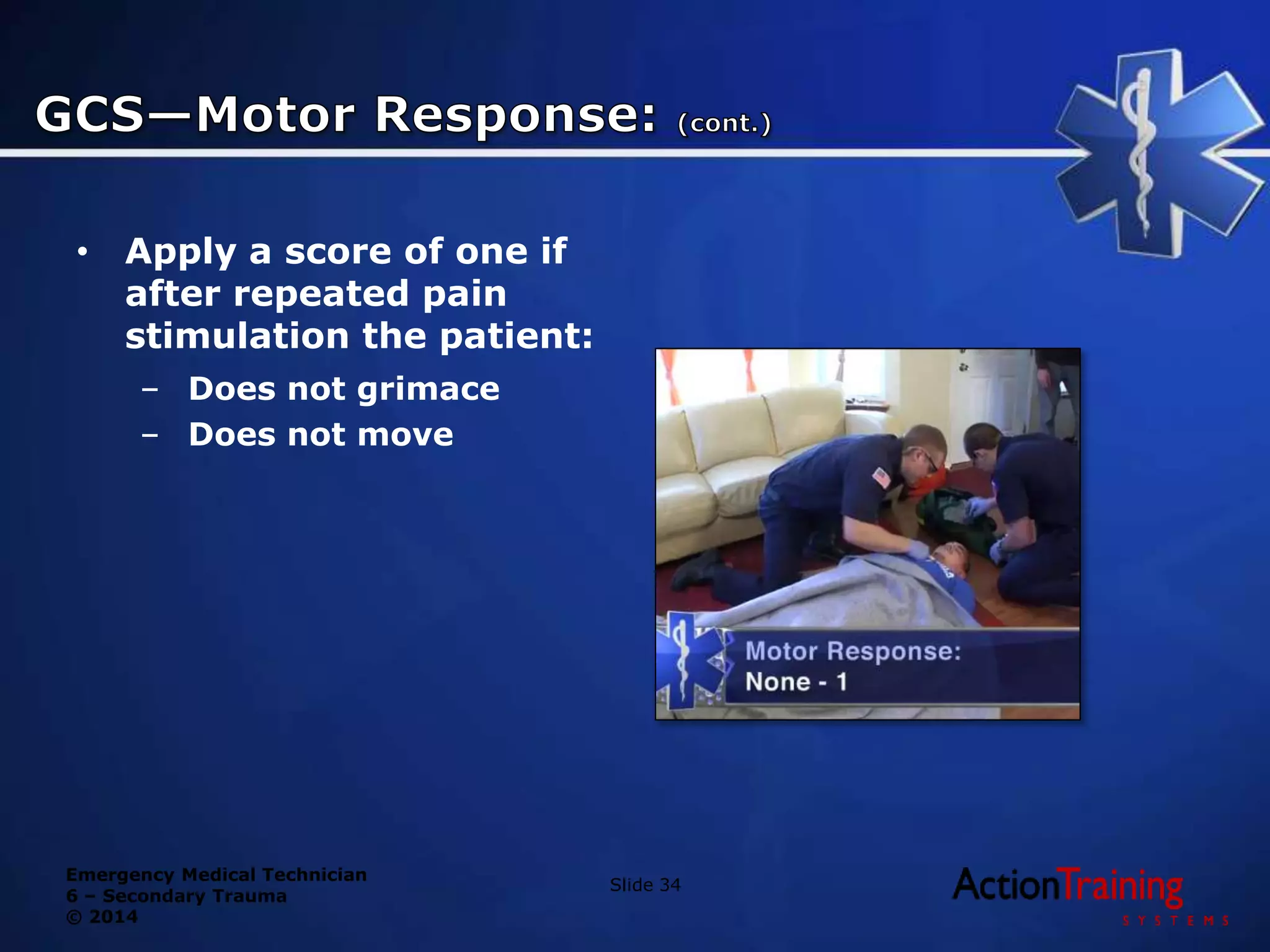



















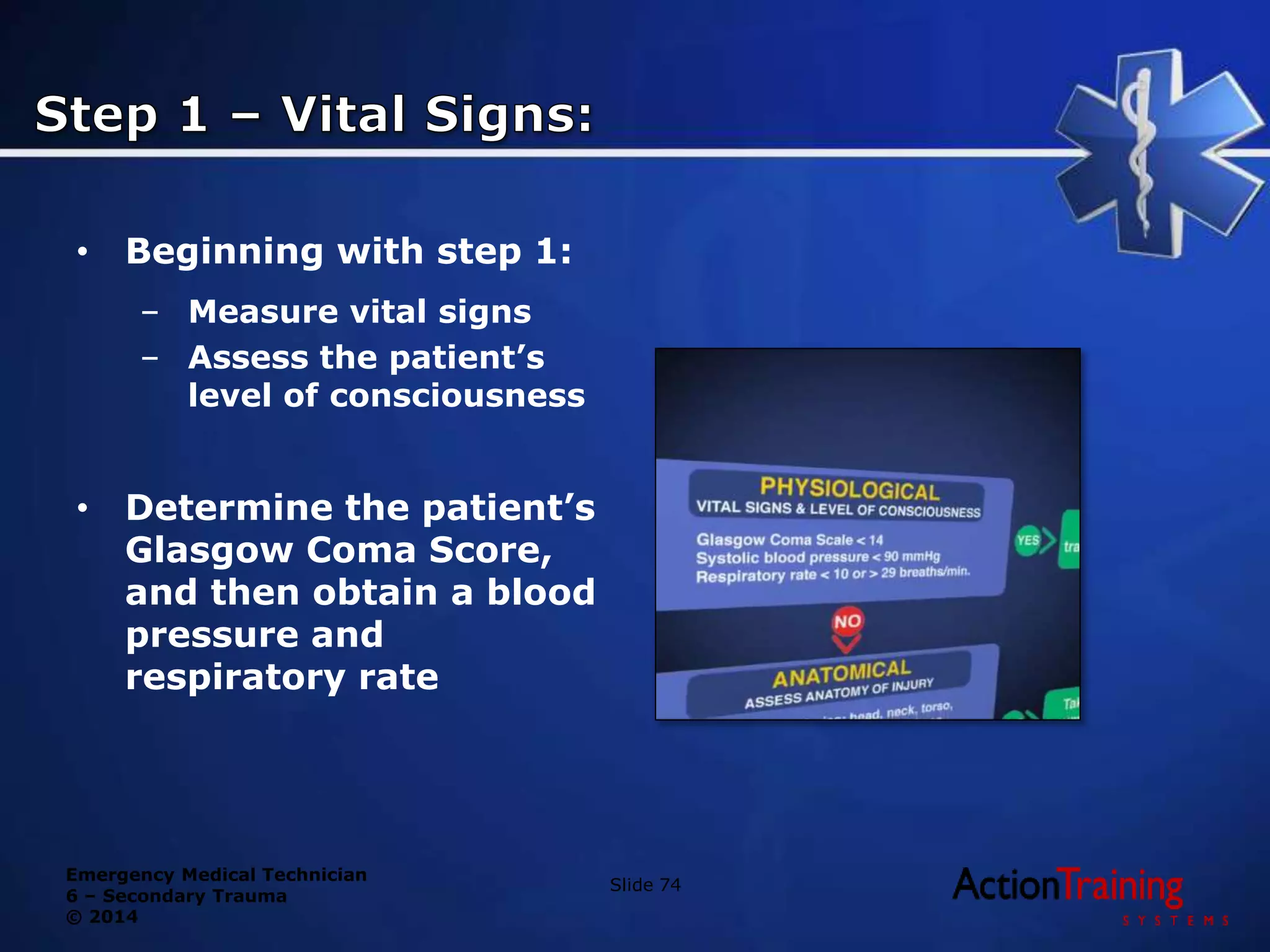



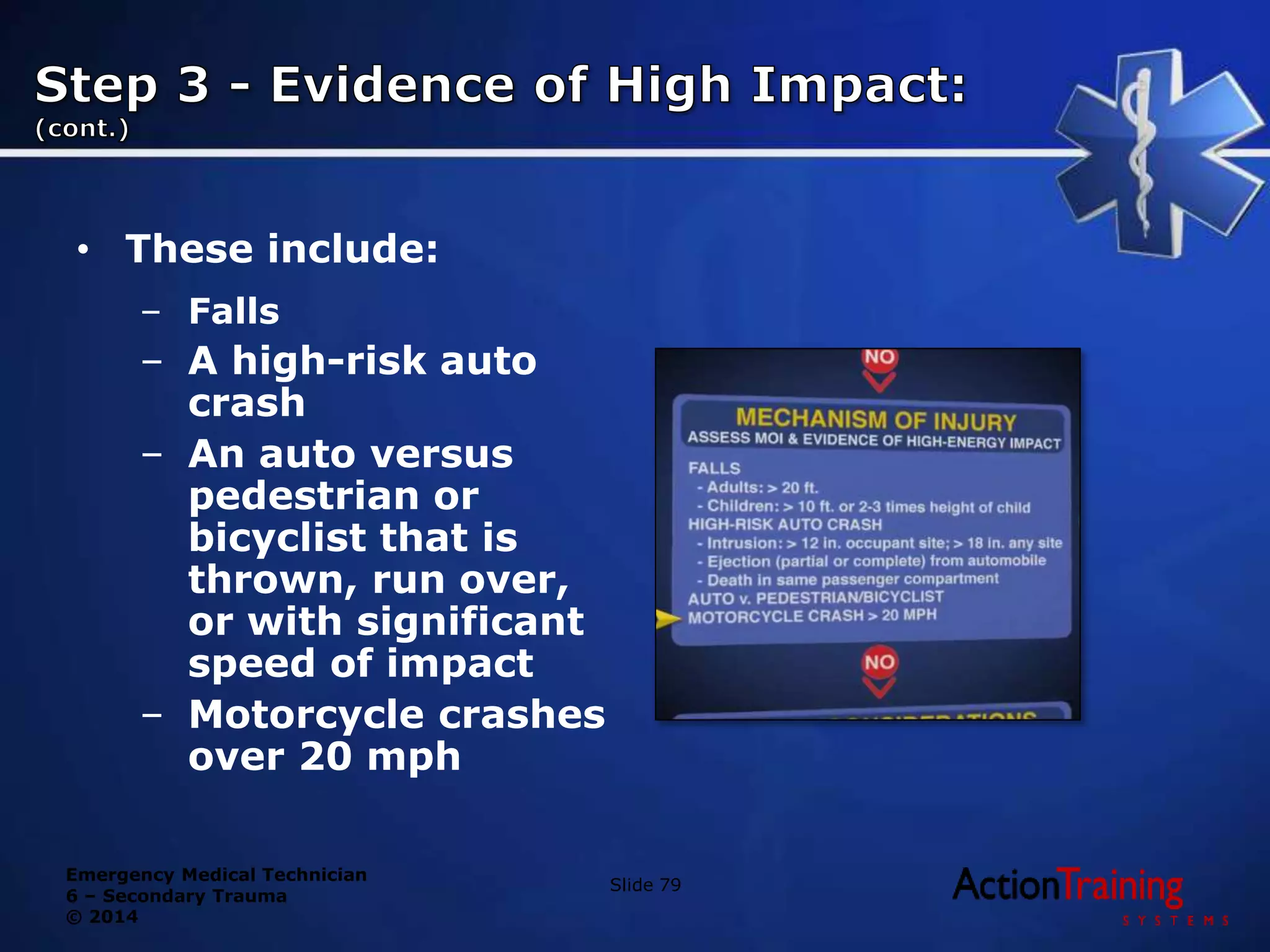

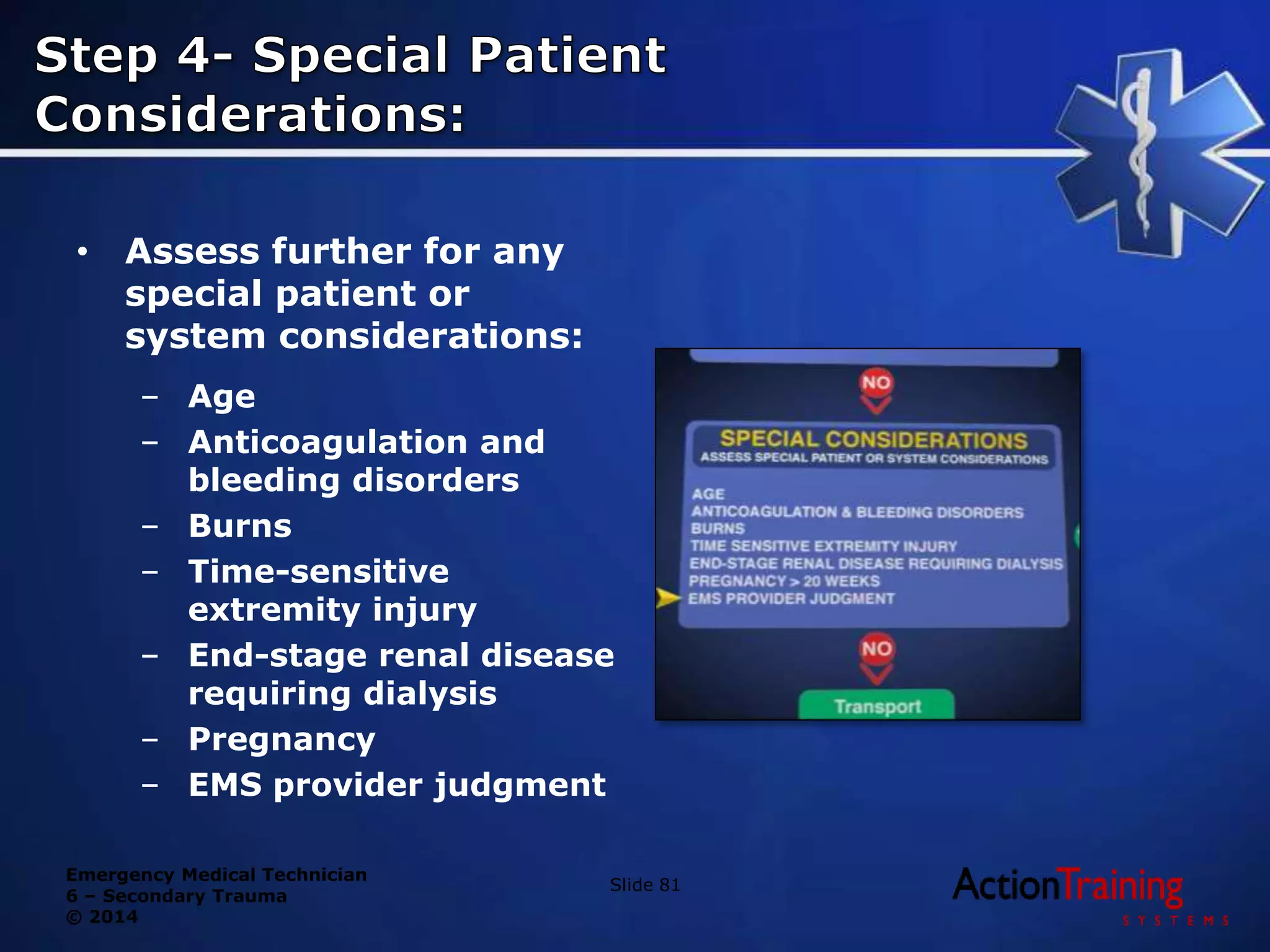




This document discusses the secondary assessment of trauma patients by emergency medical technicians. It describes assessing a patient's level of consciousness using the Glasgow Coma Scale and evaluating their motor, verbal, and eye responses to stimuli. Significant mechanisms of injury that could produce life-threatening trauma are outlined for both adults and children. The document provides guidance on performing a focused physical exam to identify injuries based on the mechanism of injury. The goal of the secondary assessment is to find potential life threats and determine if the patient requires transport to a trauma center.



















![Approach_to_the_trauma_patient[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/approachtothetraumapatient1-220906191256-c4d92395-thumbnail.jpg?width=640&height=640&fit=bounds)















































