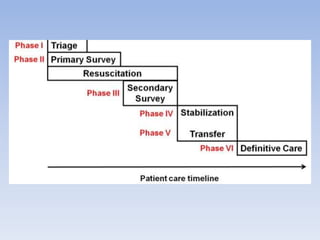
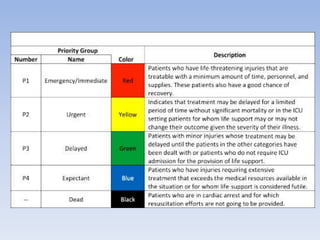
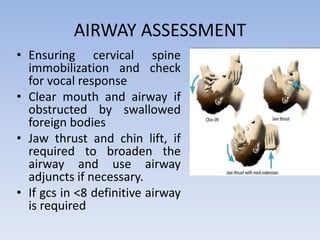
The document discusses the assessment and management of polytrauma, which involves multiple system injuries from various causes such as accidents and assaults. It outlines key procedures for primary and secondary surveys, triage, resuscitation techniques, and definitive care strategies to stabilize patients effectively. Emphasis is placed on urgent measures for airway, breathing, circulation, and identifying injuries to improve survival chances in critically injured individuals.























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













