Downloaded 145 times

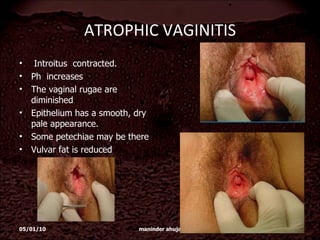
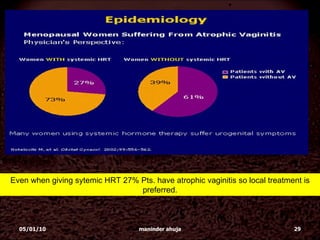
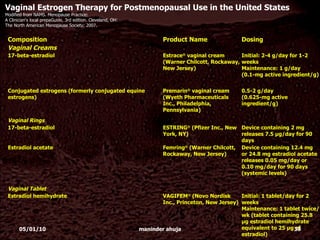
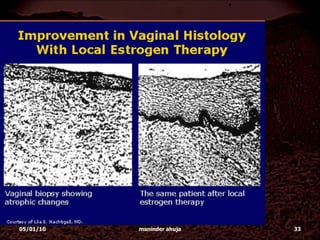


Atrophic vaginitis is underdiagnosed and undertreated in postmenopausal women. It affects around 80% of postmenopausal women, with around 20% experiencing symptoms. Local estrogen therapy is effective at treating atrophic vaginitis symptoms by improving vaginal health and reducing pH levels. Treatment options include low dose vaginal creams, rings, or tablets containing estradiol or other estrogens.



































































































