This document discusses chocolate cysts, also known as endometriomas. It provides definitions of endometriosis and discusses its prevalence, pathogenesis, classification systems, implications, clinical presentation, diagnosis and treatment approaches. Some key points include:
- Endometriosis is the presence of endometrial-like tissue outside the uterus, which induces inflammation. Estimated prevalence is 2-10% in the general female population and up to 50% in infertile women.
- The exact cause is unknown but theories include retrograde menstruation and coelomic metaplasia. It can cause painful symptoms and infertility.
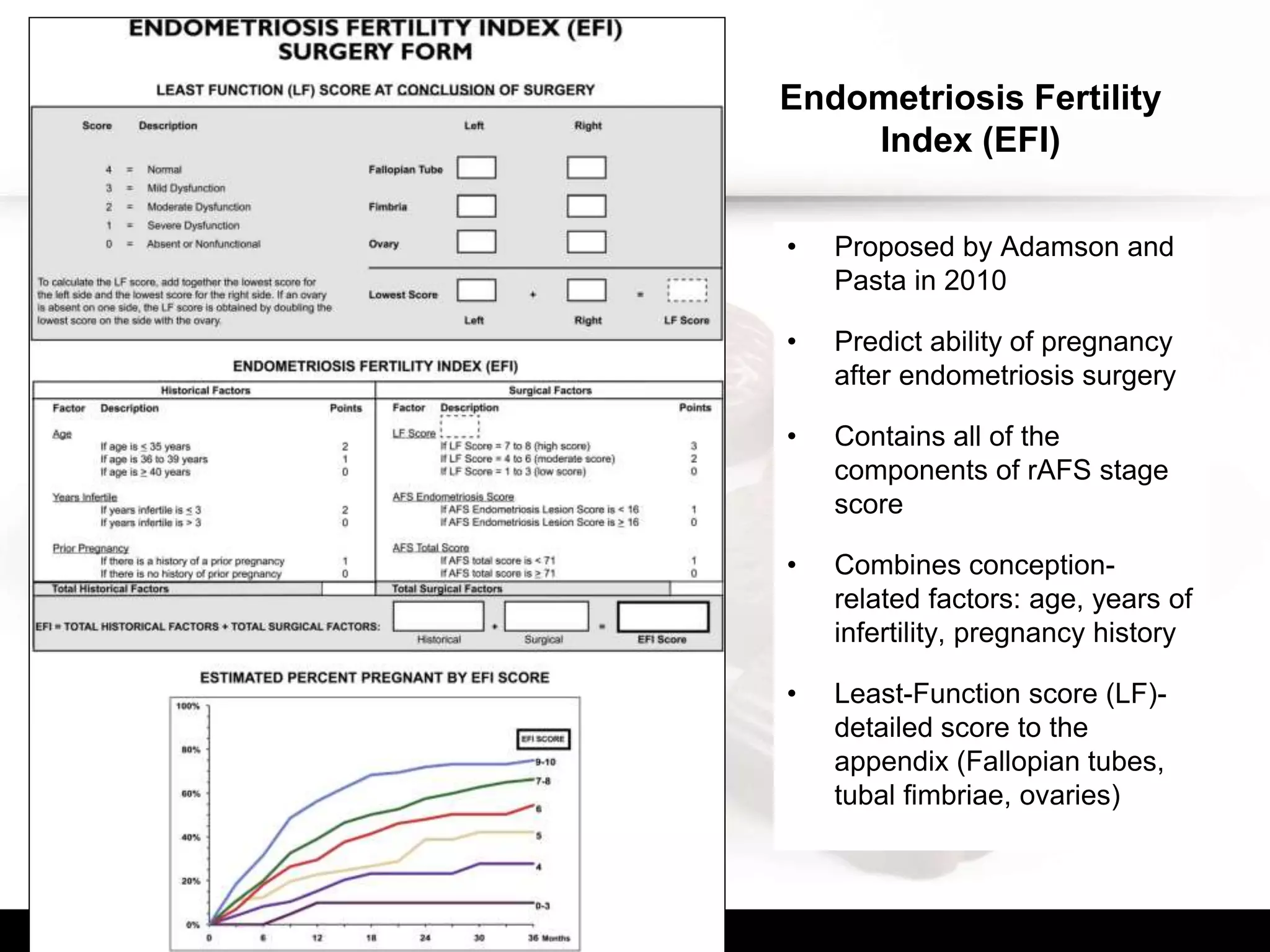
- Staging systems include rASRM and Endometriosis Fertility Index (



























![Hormonal therapies for treatment of
endometriosis-associated pain
• Endometriosis -> predominantly estrogen-dependent disease
• Hormonal suppression might be an attractive medical approach
• Recommended are: hormonal treatment [hormonal contraceptives
(level B), progestagens (level A), antiprogestagens (level A), or
GnRH agonists (level A)] as one of the options -> reduces
endometriosis-associated pain (Vercellini, et al., 1993, Brown, et al., 2012, Brown, et
al., 2010) - Recommendation A-B
• No overwhelming evidence to support particular treatment over
others
• Clinicians should take patient preferences, side effects, efficacy,
costs & availability into consideration when choosing hormonal
treatment for endometriosis-associated pain - GPP](https://image.slidesharecdn.com/chocolatecyst-atrickoratreat-150602065141-lva1-app6891/75/Chocolate-cyst-a-trick-or-a-treat-30-2048.jpg)


![• Progestagens & anti-progestagens
– Progestagens [medroxyprogesterone acetate (oral or depot), dienogest,
cyproterone acetate, norethisterone acetate, danazol] or anti-
progestagens (gestrinone) as one of the options, to reduce
endometriosis-associated pain (Brown, et al., 2012) – A
– Consider prescribing a levonorgestrel-releasing intrauterine system
as one of the options to reduce endometriosis-associated pain (Ferreira,
et al., 2010, Gomes, et al., 2007, Petta, et al., 2005) - B
– No evidence to suggest a benefit of progestagens over other treatments
– Take the different side-effect profiles of progestagens and anti-
progestagens into account when prescribing these drugs, especially
irreversible side effects (e.g. thrombosis, androgenic side effects)](https://image.slidesharecdn.com/chocolatecyst-atrickoratreat-150602065141-lva1-app6891/75/Chocolate-cyst-a-trick-or-a-treat-33-2048.jpg)











































































































