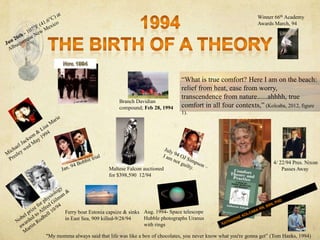
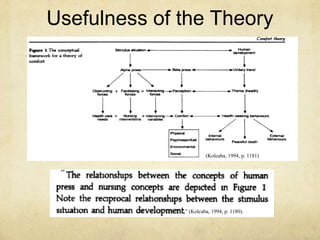
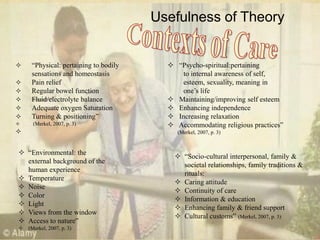
The document discusses the origin and development of Katherine Kolcaba's Theory of Comfort. Kolcaba developed the theory based on her experience with her brother's cancer and the comforting actions of nurses. She conducted a concept analysis that examined literature from several disciplines. The theory proposes three types of comfort - relief, ease, and transcendence - within four contexts of human experience. Major influences on the theory included the works of Orlando, Henderson, Paterson and Zderad. The theory provides a useful framework for assessing and meeting patient needs across physical, psycho-spiritual, sociocultural, and environmental domains.
![Meaning of Comfort
―A model of human press is the framework within which
comfort is related to interventions that enhance the state of
comfort desirable subsequent outcomes of nursing care‖
(Kolcaba, 1994, p.1178).
―The theory of holistic comfort is a
component of a normative and
descriptive theory for nursing care‖
(Kolcaba, 1994, p. 1180).
“First meaning:
Comfort — a cause of relief from
discomfort and/or of the state of comfort‖
(Kolcaba & Kolcaba, 1991, p. 1302).
“Fourth meaning:
Comfort — whatever makes life easy
or pleasurable‖ (Kolcaba & Kolcaba, 1991, p. 1302).
.
“Second Meaning:
Comfort — the state of ease and peaceful contentment‖
(Kolcaba & Kolcaba, 1991, p. 1302).
“Third meaning:
Comfort — relief from discomfort‖
(Kolcaba & Kolcaba, 1991, p. 1302).
[The construction of Kolcaba‘s theory
of comfort was the result of different
methods for theory development
applied during different stages of the
process of theory development. In
review, those methods were (1)
inductive explication of the
components of a specific practice, (2)
concept analysis and operationalization
of components that were yet
undefined, (3) deduction from a more
general organizing theory with
relocation of the main concepts, and
(4) retroduction to bring to the model a
concept for outcomes research] (Kolcaba,
2001).](https://image.slidesharecdn.com/astanehppt-131005102105-phpapp01/85/Astaneh-ppt-2-320.jpg)
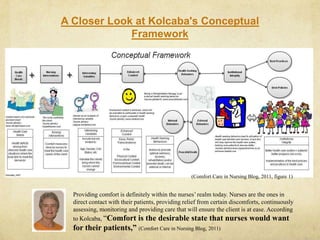
![[Theoretical Mode
Major Concepts and Definitions used in Conceptual Framework
Health Care Needs are those identified by the patient/family in a particular practice setting.
Comforting Interventions are nursing interventions that are designed to address specific comfort needs of
recipients. This includes physiological, social, financial, psychological, spiritual, environmental, and physical
interventions.
Intervening Variables are interacting forces that influence recipients' perceptions total comfort. This includes
factors such as past experiences, age, attitude, emotional state, support system, prognosis, and finances.
Enhanced Comfort
is an immediate desirable outcome of nursing care, according to Comfort
Theory. When comfort interventions are delivered consistently over time,
they are theoretically correlated a trend toward increased comfort levels over
time, and with desired health seeking behaviors (HSBs).
Health-Seeking Behaviors (HSBs):
The relationships between comfort and health seeking behaviors are entailed
in the second part of Kolcaba's comfort theory.
Internal: healing, immune function, number of T cells, etc.
External: health related activities, functional outcomes
Peaceful Death] (Nursing Theory, 2011, para. 3).](https://image.slidesharecdn.com/astanehppt-131005102105-phpapp01/85/Astaneh-ppt-3-320.jpg)
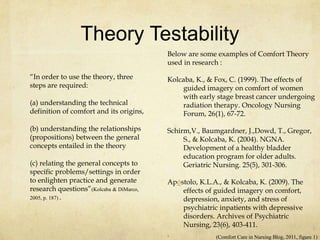
![Origin of the Theory
What was going on:
Katherine Kolcaba originally wrote the Theory
of Comfort with Alzheimer‘s and dementia
patients in mind. This is what was going on in
her world and she wanted to help out.
[I borrowed the ideas about Relief, Ease, and
Transcendence. Later, I "borrowed" the contexts
of experience from the literature review about
holism. I put these ideas together in a unique way.
Later, I borrowed the framework for the First and
Second parts of Comfort Theory from Henry
Murray. But I hung nursing concepts on his
abstract framework in a unique way. The idea of
institutional outcomes was unique and was added
through a process Tomey and Alligood call
retroduction] (Kolcaba, Durr, & Stoner, 2010, figure FAQ).
Motivation to write:
[My brother died of cancer when he was 41,
and during his illness I gained more
experience with comforting actions of nurses,
and how to articulate what they did. Because
of that experience and its timing, my
dissertation is about women with breast
cancer, not dementia or gerontology. And I
have done a lot of work with end of life
comfort] (Kolcaba, Durr, & Stoner, 2010, figure FAQ).
[My spirituality, which my mother fostered
and role-modeled for me, has also had a
strong influence] (Kolcaba, Durr, & Stoner, 2010,
figure FAQ).
[Also, my husband has always been a huge
supporter and brain stormer about Comfort
Theory] (Kolcaba, Durr, & Stoner, 2010, figure FAQ).
.
(Kolcaba, Durr, & Stoner, 2010, figure FAQ)](https://image.slidesharecdn.com/astanehppt-131005102105-phpapp01/85/Astaneh-ppt-8-320.jpg)
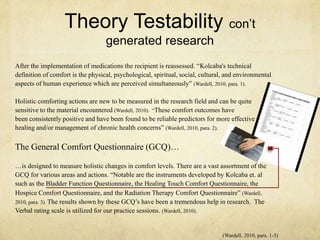
![Origin of the Theory con’t
Major influences in the development of
Comfort Theory:
[Relief: Ida Jean Orlando (1961 / 1990)
Nursing Process Theory
Ease: Virginia Avernal Henderson
(1978) Need Theory
Transcendence: Josephine Paterson
& Loretta Zderad (1976 / 1988) Humanistic
Nursing Theory
Framework for Comfort
Theory: Murray (1938) Henry Murray
designed a conceptual framework
diagrammed in three lines. Comfort theory
takes that framework to another level to
include a fourth line. This fourth line is the
framework for the comfort theory].(Kolcaba, Durr, & Stoner, 2010, figure FAQ).](https://image.slidesharecdn.com/astanehppt-131005102105-phpapp01/85/Astaneh-ppt-10-320.jpg)
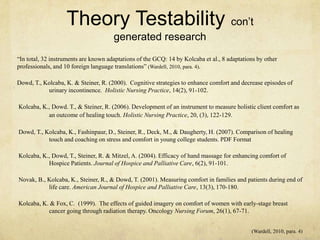
![Propositions in Kolcaba‘s middle-range
Theory of Comfort
[Propositions of Comfort Theory
1. Nurses identify comfort needs of patients and family members.
2. Nurses design interventions to meet identified needs.
3. Intervening variables are considered when designing interventions.
4. When interventions are delivered in a caring manner and are effective, and when enhanced
comfort is attained, interventions are called ―comfort measures‖.
5. Patients and nurse agree on desirable and realistic health- seeking behaviors.
6. If enhanced comfort is achieved, patients and family members are more likely to engage in
health-seeking behaviors these further enhance comfort.
7. When patients and family members are given comfort care and engage in health-seeking
behaviors, they are more satisfied with health care and have better health-related outcomes.
8. When patients, families, and nurses are satisfied with health care in an institution, public
acknowledgment about that institution‘s contributions to health care will help the institution
remain viable and flourish]
[These propositions provide a systematic approach to a solution by incorporating a
process that involves identifying a need, addressing that need, identifying
intervening variable, provide appropriate interventions, assessing if the goal is
achieved, and reaffirming the healthy behaviors learned by the client. Essentially,
Kolcaba has developed a nursing process that is specific to her Theory of Comfort]
(Weller, 1999, para. 8).
(Kolcaba, Durr, & Stoner, 2010, figure FAQ).](https://image.slidesharecdn.com/astanehppt-131005102105-phpapp01/85/Astaneh-ppt-20-320.jpg)
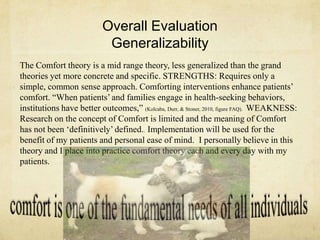
![Different Evolution of Experimental and Comparisons Psychiatric
Inpatients on Total Comfort
This quasi-experimental design was used to measure the differences in comfort, depression, anxiety,
and stress between a treatment group and a usual care group (comparison) of short-term psychiatric
inpatients diagnoses with depressive mood disorders.
Psychiatric Inpatients Comfort Scale (PICS), PICS evaluated reliability, construct validity, and
concurrent validity. The PICS is 5-point Likert type scale with 42 items for self-reporting ranging
from 1, “It doesn't correspond to anything that happens with me” to 5, “It totally corresponds to
what happens with me.”
―Depression, Anxiety, and Stress Scales (DASS-21). the authors assessed scale reliability, construct
validity, and concurrent validity. The DASS-21 contained a set of three 4-point Likerttype subscales
for self-reporting. Each subscale consisted of seven items, aimed at assessing depression, anxiety,
and stress] (Apostolo & Kolcaba, 2009).
[Imagery creates a bridge between mind and body, linking perception, emotion, and psychological, physiological, and
behavioral responses.
. Different Evolution of Experimental and Comparisons Psychiatric Inpatients on
Total Comfort
Example Case Study where
Comfort Theory Utilized-
(Apostolo & Kolcaba, 2009)-all cited so
not to loose meaning of test](https://image.slidesharecdn.com/astanehppt-131005102105-phpapp01/85/Astaneh-ppt-21-320.jpg)
![References
Apostolo, J. L., & Kolcaba, K. Y. (2009). The effects of guided imagery on comfort,
depression, anxiety, and stress of psychiatric in patients with depressive disorders. Archives
of Psychiatric Nursing, 23(6), 403-411. http://dx.doi.org/10.1016/j.apnu. 2008.12.003
Comfort Care in Nursing Blog. (2011, September 11). Kolcaba‘s activity [Blog comment].
Retrieved from http://comfortcareinnursing.blogspot.com/p/comfort-theory-major
Current Nursing. (2013). Retrieved March 25, 2010, from http://currentnursing.com/
nursing_theory/application_nursing_theories.html
Kolcaba, K. (1994). A theory of holistic comfort for nursing. Journal of Advanced Nursing, 19,
1178-1184. http://dx.doi.org/10.1111/j.1365-2648.1994.tb01202.x
Kolcaba, K. (2001). Evolution of the mid range theory for outcomes research. Nursing
Outlook, 49(2), 86-92. http://dx.doi.org/10.1067/mno.2001.110268
Kolcaba, K., & DiMarco, M. A. (2005). Comfort theory and its application to Pediatric
nursing. Pediatric Nursing, 32(3), 187-194. Retrieved from http://
www.medscape.com/viewarticle/507387_2
Kolcaba, K., Durr, K., & Stoner, M. [Comfort Line]. (2010, June). FAQ [Blog comment].
Retrieved from http://www.thecomfortline.com](https://image.slidesharecdn.com/astanehppt-131005102105-phpapp01/85/Astaneh-ppt-24-320.jpg)
![Kolcaba, K., & Kolcaba, R. (1991). An analysis of the concept of comfort. Journal of Advanced Nursing,
16(11), 1301-1310. http://dx.doi.org/10.1111/j.1365-2648.1991.tb01558.x
Kolcaba, K. Y. (2012, July 12). True Comfort [Blog comment]. Retrieved from http://
www.thecomfortline.com
McEwen, M., & Willis, E.M. (2011). Theoretical Basis of Nursing, (3rd ed.). Philadelphia: Lippincott.
Merkel, S. (2007). Comfort Theory: A Framework for pain management nursing practice. [PowerPoint
slides]. Retrieved from http://www.aspmn.org/conference/documents/sandramerkelfull.pdf
Nursing Theory. (2011). Retrieved July 14, 2013, from http://nursing-theory.org/theories- and-models/
Kolcaba-theory-of-
Tomey, A. M., & Alligood, M. R. (2010). Nursing theorists and their work. (7th ed.). Maryland Heights,
MO: Mosby Elsevier
Wardell, D. W. (2010). Measurement tools: Comfort touch. American Holistic Nurses Association, 2(2).
Retrieved from http://www.ahna.org/portals/4/docs/Research/eNews/Connections_R-eNews_1-10.htm
Weller, K. [KWeller Nursing Blog]. (1999, Summer). Scholarly [Blog comment]. Retrieved from http://
kweller99.wordpress.com/scholarly-work/
References Cont‘d](https://image.slidesharecdn.com/astanehppt-131005102105-phpapp01/85/Astaneh-ppt-25-320.jpg)

































































![Nursing theory presentation[1] AMJAD.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/nursingtheorypresentation1amjad-240725182944-f7b0345a-thumbnail.jpg?width=640&height=640&fit=bounds)





















