Downloaded 24 times














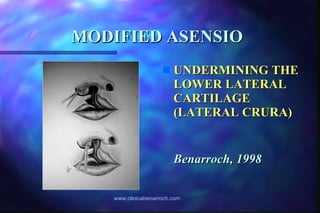








The document discusses the nasal deformities associated with unilateral cleft lip and the Asensio technique for repairing the lip and nose simultaneously. It describes the nasal deformities such as a shorter columella and displaced lower lateral cartilage on the cleft side. The modified Asensio technique aims to correct these deformities by repositioning tissues and cartilage during lip repair. Studies found no nasal growth disturbances with this simultaneous approach.













































































