Downloaded 615 times

















![Arrhythmias, related with violationArrhythmias, related with violation
ofof automatismautomatism of heartof heart
Distinguish two groups of arrhythmiasDistinguish two groups of arrhythmias, related with, related with violationviolation
of automatism of heart.of automatism of heart.
1)1) Nomotopic arrhythmiasNomotopic arrhythmias -- the generation of impulsesthe generation of impulses, as well, as well
as in a norm,as in a norm, takes place bytakes place by pacemaker cells (P-cells) inpacemaker cells (P-cells) in
sinoatrial [sinus] node, [nodus sinuatrialis]sinoatrial [sinus] node, [nodus sinuatrialis]. To them belong:. To them belong:
a)a) sinus tachycardiasinus tachycardia is multiplying frequency of cardiacis multiplying frequency of cardiac
reductions;reductions;
b)b) sinus bradycardiasinus bradycardia is diminishing of frequency of cardiacis diminishing of frequency of cardiac
reductions;reductions;
c)c) sinus (respiratory) arrhythmiasinus (respiratory) arrhythmia is a change of frequency ofis a change of frequency of
heartbeat in the different phases of respiratory cycleheartbeat in the different phases of respiratory cycle
(become more frequent at inhalation [breath] and(become more frequent at inhalation [breath] and
diminishing is at exhalation [outward breath]).diminishing is at exhalation [outward breath]).](https://image.slidesharecdn.com/arrhytmias2013med-130202062202-phpapp02/85/Arrhytmias-20-320.jpg)



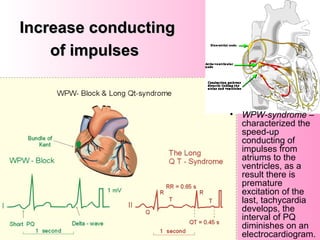
![Reason and mechanisms of development ofReason and mechanisms of development of
sinus tachy- and bradycardiasinus tachy- and bradycardia
Increase generating of impulsesIncrease generating of impulses .. Reasons:Reasons:
a) at diminishing of level of maximal diastolic potential of cells of sinus nodea) at diminishing of level of maximal diastolic potential of cells of sinus node
b) at approaching to it of maximum critical potential,b) at approaching to it of maximum critical potential,
c) at multiplying speed of slow diastolic depolarization.c) at multiplying speed of slow diastolic depolarization.
Such phenomenon is observed:Such phenomenon is observed:
a) under act of the promoted temperature of bodya) under act of the promoted temperature of body
b) stretching areas of sinus node,b) stretching areas of sinus node,
c) under act of mediators of sympathetic system.c) under act of mediators of sympathetic system.
Opposite,Opposite,
a) diminishing of speed of slow diastolic depolarization,a) diminishing of speed of slow diastolic depolarization,
b) hyperpolarization in a diastole andb) hyperpolarization in a diastole and
c) the decreasing of critical maximum potential, as it is observed at annoying ac) the decreasing of critical maximum potential, as it is observed at annoying a
vagus nerve, are accompanied deceleration of generation of impulses, andvagus nerve, are accompanied deceleration of generation of impulses, and
consequently -consequently -
The instability [fluctuation, variation] of tone of vagus nerve during the act ofThe instability [fluctuation, variation] of tone of vagus nerve during the act of
breathing predetermine respiratory arrhythmia (become more frequentbreathing predetermine respiratory arrhythmia (become more frequent
palpitation at inhalation, deceleration - at exhalation).palpitation at inhalation, deceleration - at exhalation).
Children have respiratory arrhythmia in a normChildren have respiratory arrhythmia in a norm , sometimes it also, sometimes it also
observed for adults.observed for adults.
Tachycardia developsTachycardia develops
Bradycardia developsBradycardia develops](https://image.slidesharecdn.com/arrhytmias2013med-130202062202-phpapp02/85/Arrhytmias-24-320.jpg)
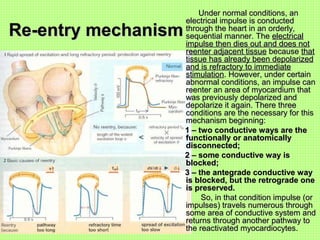
![Arrhythmias, related to violations of excitabilityArrhythmias, related to violations of excitability
The main reason is appearance so-called ectopic hotbed of
excitations which generate premature impulsespremature impulses.
The most widespread arrhythmias of this group are:
a) extrasystole [beat]a) extrasystole [beat] andand
b) paroxysmal [recurrent, reentrant] tachycardia.b) paroxysmal [recurrent, reentrant] tachycardia.
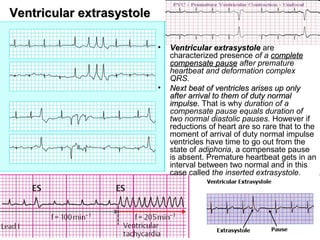
Extrasystole is a type of arrhythmias, which are stipulated
violations of function of excitability which shows up the origin
of premature contraction of heart or only ventricles.
In dependence on localization of hotbed which an premature
impulse goes out from, distinguish the followings types of
extrasystole:
a)a) sinussinus (or nomotopic),(or nomotopic),
b)b) atrialatrial,,
c)c) atrio-ventricularatrio-ventricular andand
d)d) ventricular [ventricular premature beats].ventricular [ventricular premature beats].
As a wave of excitation, which arose up in an unusual place,
spreads in the changed direction, it is reflected on the
structure of the electric field of heart and finds a reflection on
an electrocardiogram.](https://image.slidesharecdn.com/arrhytmias2013med-130202062202-phpapp02/85/Arrhytmias-25-320.jpg)




















The document outlines a lecture plan on the circulatory system, covering topics like the cardiac cycle, the heart's conductive system, arrhythmias, and ischemic heart disease. It details the causes, classifications, and mechanisms of arrhythmias, highlighting their relationship with various diseases and physiological influences. Additionally, it explains the heart's structure, functionality, and the impact of various factors on heart rhythm and circulation.