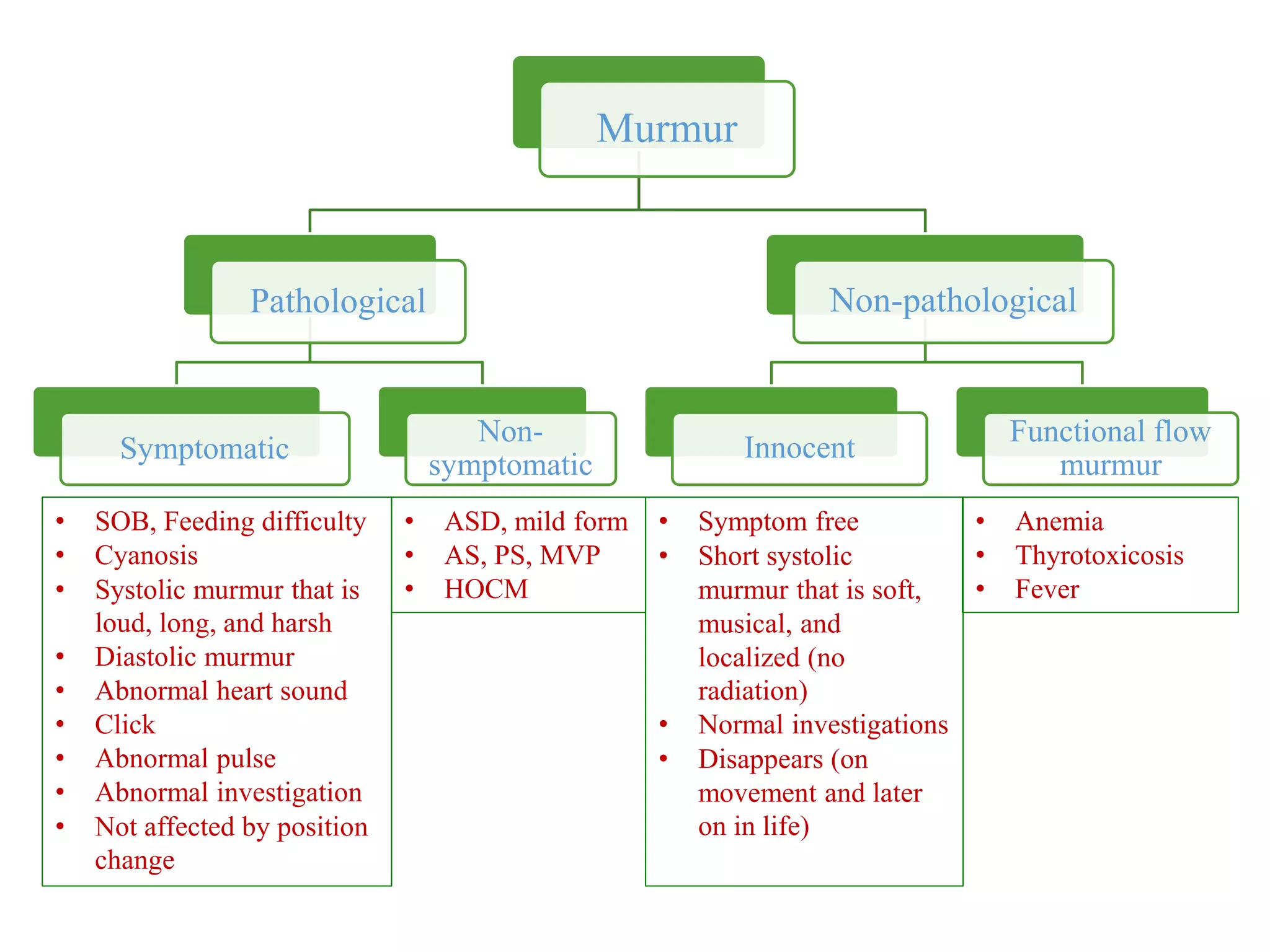
This document discusses the approach to murmurs in pediatrics. It defines a murmur as a heart sound produced by turbulent blood flow across a heart valve or defect. Murmurs can be innocent, pathological, or symptomatic. Innocent murmurs are harmless and common in children. Pathological murmurs indicate an underlying structural issue. Symptomatic murmurs cause issues like shortness of breath. The document outlines characteristics of different types of murmurs and provides guidance on evaluating a child presenting with a murmur through history, physical exam, and potential further workup.
















![1. History:
• Feeding history, exercise intolerance. [HF. In <1-year exercise level
is obtained during feeding (an infant with HF can only take small
volumes of milk, develops SOB on sucking, and often perspires)]
• Heavy sweating with minimal or no exertion.
• Poor appetite and failure to grow normally (in infants). [indicates
heart failure (HF)]
• Chronic cough. [indicates lung congestion]
• Swelling or sudden weight gain. [Edema]
• Cyanosis or cyanotic spells ± squatting posture (indicates cyanotic
CHD, classically seen in tetralogy of Fallot).
• Chest pain, prolonged fever. [Endocarditis]
• Dizziness, fainting episodes.](https://image.slidesharecdn.com/approachtomurmurinpaediatrics-221125165919-6ee8014d/75/Approach-to-murmur-in-Paediatrics-pptx-34-2048.jpg)


![• Birth History.
• Was the baby term or preterm (structural abnormalities)?
• Was there asphyxia? (caused by a type of C.M., low O2 to the
heart),
• ask for prolonged labor, history of convulsion, and SGA
• Maternal complications:
• DM leads to HOCM.
• HTN leads to TGA.
• SLE lead to COMPLETE HEART BLOCK.
• TORCH: rubella leads to PDA.
• Drug history:
• Isotretinoin is teratogenic.
• Anti-convulsants.
• Aspirin.
• Is there a family history of congenital heart disease? [There
is a higher risk of heart defects in siblings of children with
congenital heart disease.]](https://image.slidesharecdn.com/approachtomurmurinpaediatrics-221125165919-6ee8014d/75/Approach-to-murmur-in-Paediatrics-pptx-37-2048.jpg)














































![[Int. med] heart murmurs from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/b29t6cwrtzwunmrfazue-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171700-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)