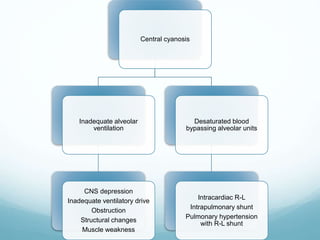
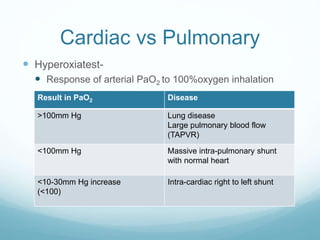
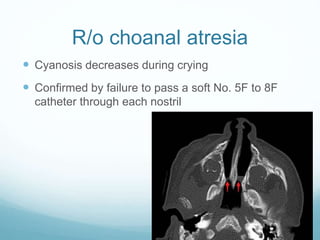
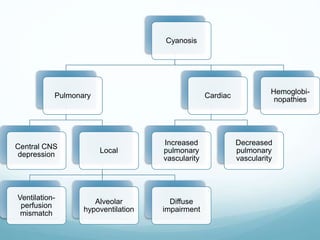
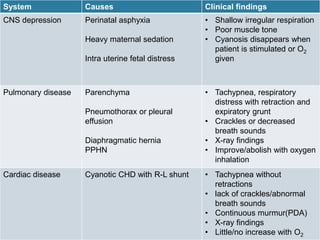
Cyanosis is a bluish discoloration of the skin and mucous membranes caused by low oxygen levels. It can be due to pulmonary or cardiac issues. Pulmonary causes include problems leading to ventilation-perfusion mismatching or low oxygen exchange in the lungs. Cardiac causes are congenital heart defects causing right-to-left shunts, reducing oxygenated blood to the body. Diagnosis involves physical exam, blood tests, chest x-ray, and oxygen responsiveness testing to distinguish between cardiac and pulmonary etiologies. Initial management focuses on stabilization, monitoring, supportive care like oxygen, and treating any underlying issues like sepsis.









![Approach to Cyanosis [Paediatrics presentation for medical (MBBS) students]](https://cdn.slidesharecdn.com/ss_thumbnails/approachtocyanosis71to77final-210927113642-thumbnail.jpg?width=640&height=640&fit=bounds)



















































































