Download to read offline

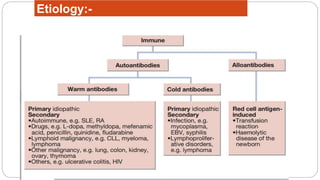
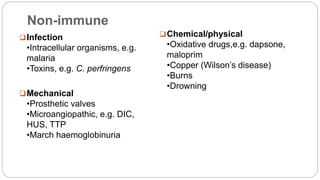
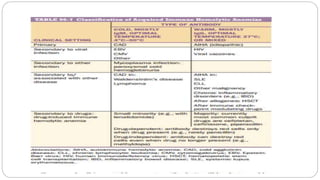


This document discusses approaches to extracorpuscular hemolytic anemia. It begins by defining extracorpuscular anemias as defects in which red blood cells are normal but destroyed due to mechanical, immunologic, infectious, or metabolic/oxidant damage. It then covers the etiology of non-immune and immune hemolytic anemias, including infections, mechanical factors like prosthetic valves, chemicals/drugs, and autoimmune disorders. Warm and cold agglutinin diseases are described as types of autoimmune hemolytic anemia. The document concludes by covering non-immune causes such as mechanical heart valves, burns, and microangiopathic anemias.








































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)