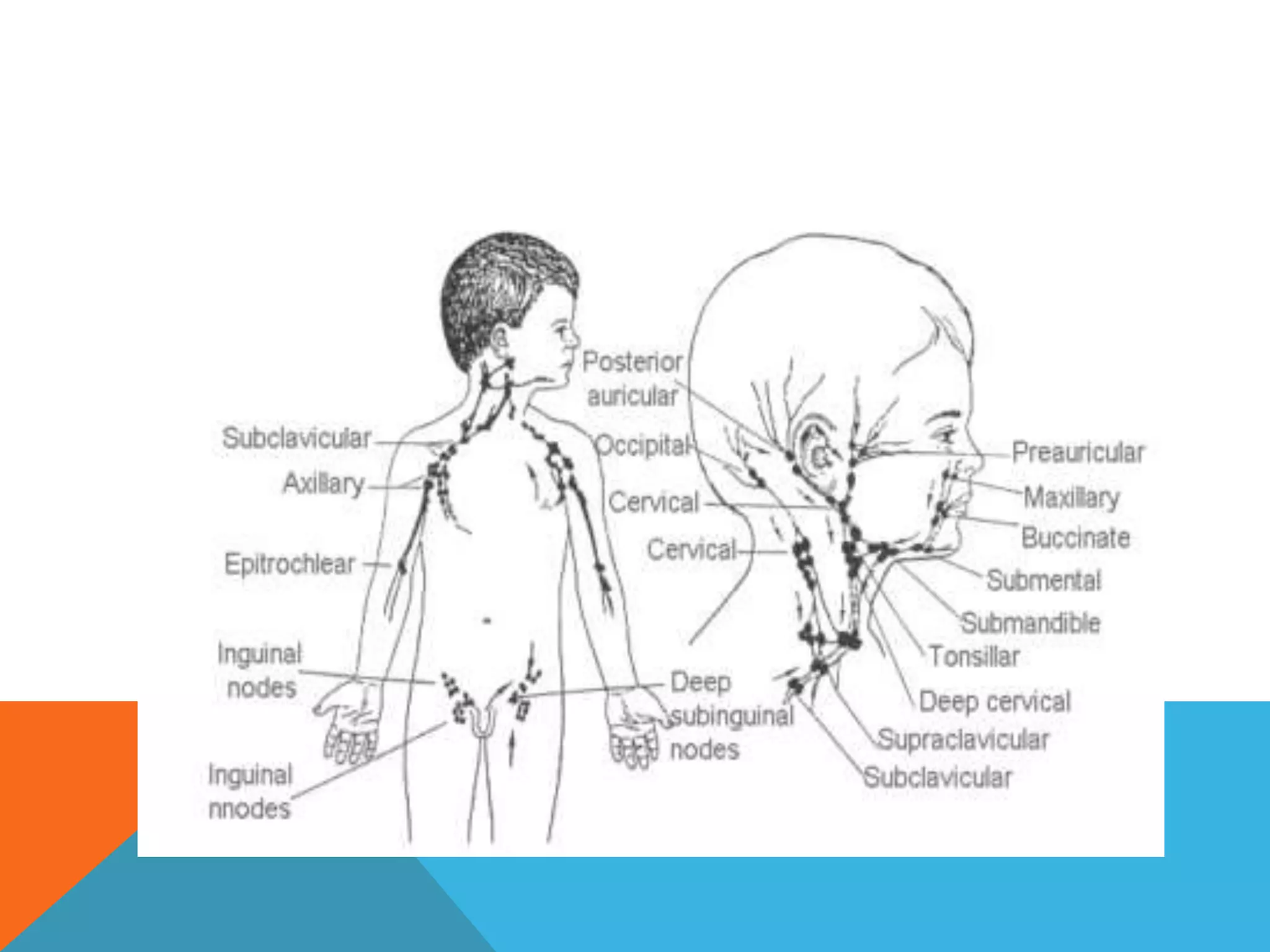
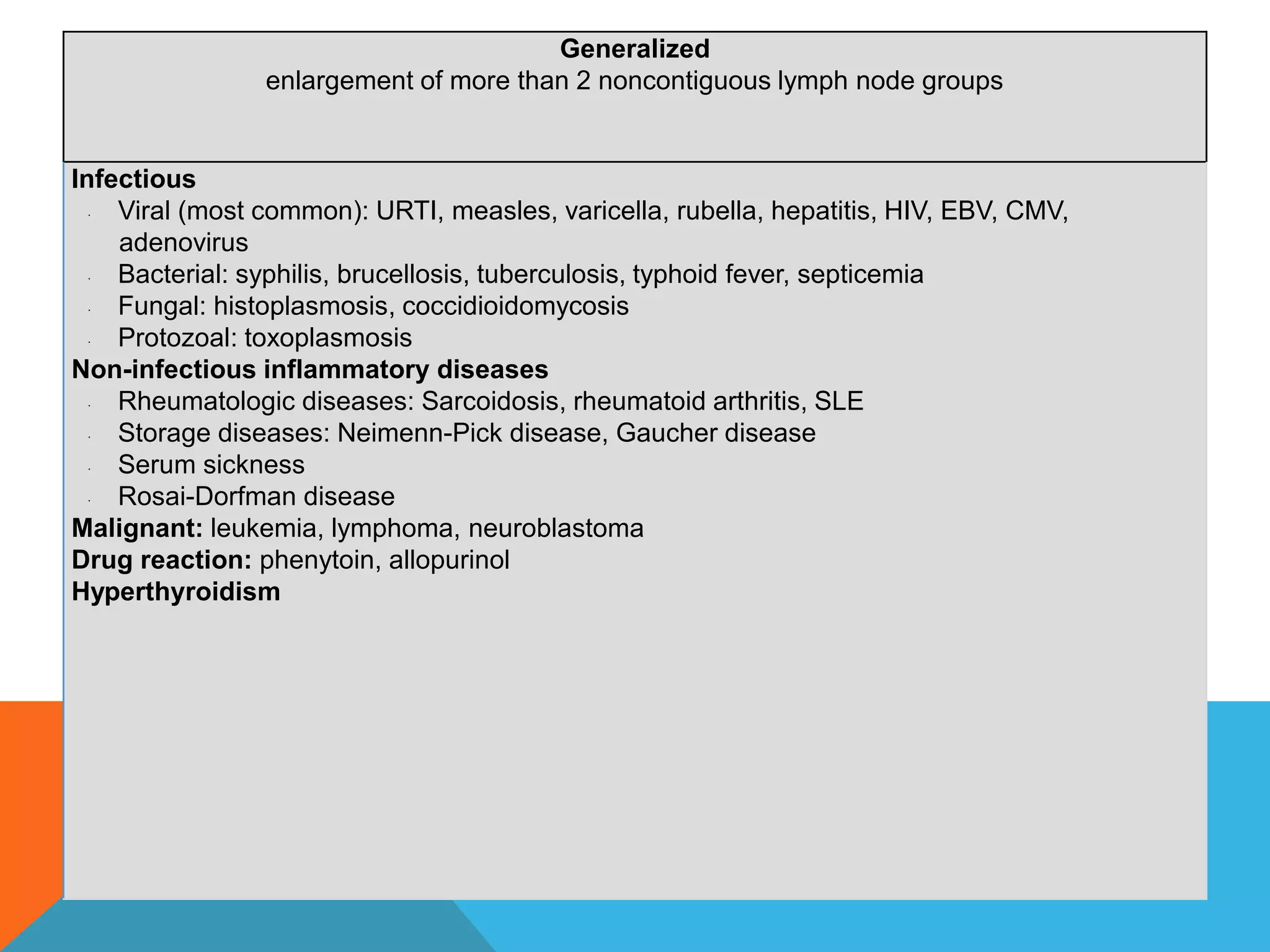
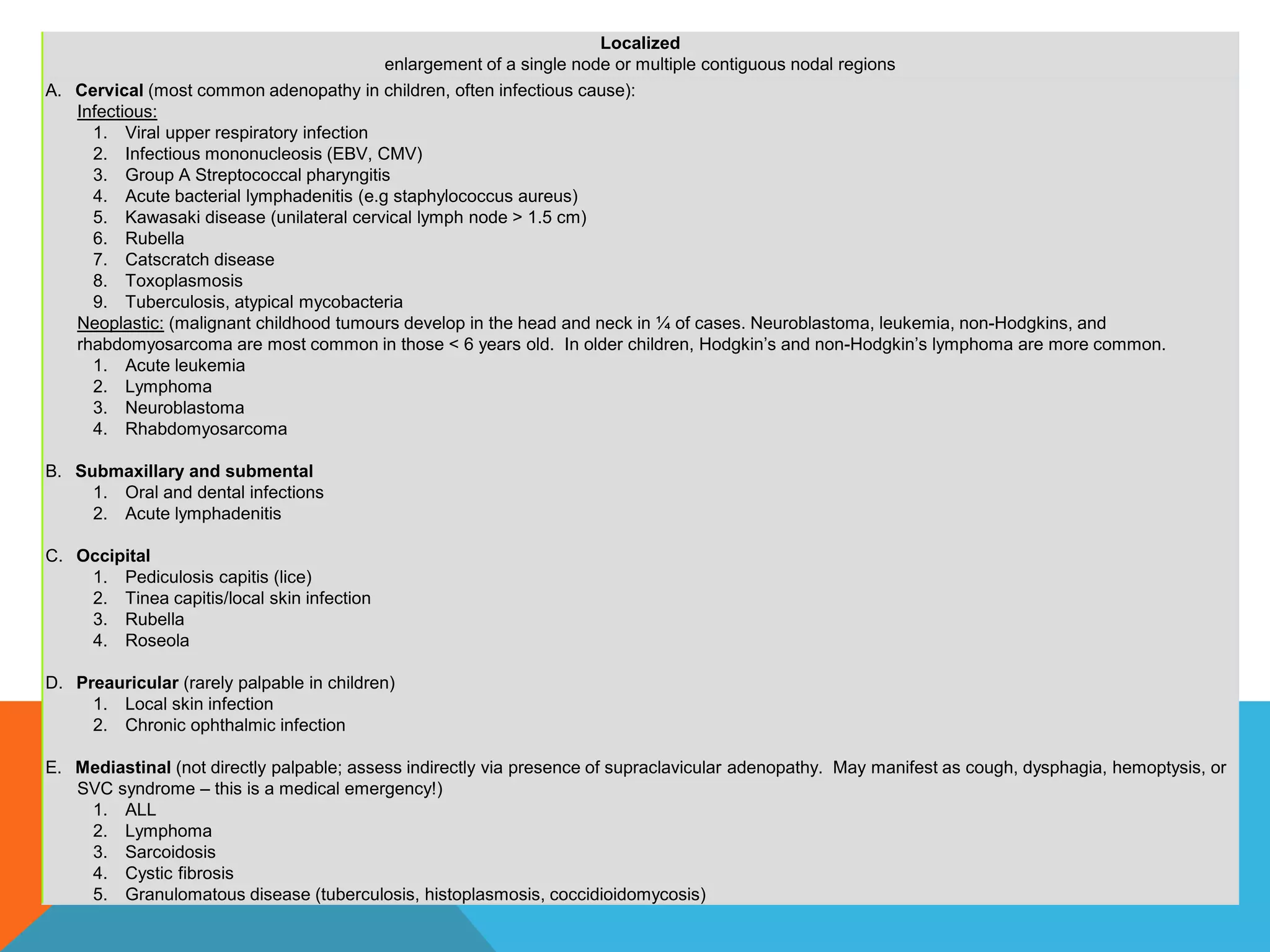
Lymphadenopathy refers to enlarged lymph nodes, which can occur due to viral or bacterial infections leading to immune responses in the lymph nodes. A physical examination should closely examine the head, neck, skin, abdomen and lymph nodes themselves, noting characteristics like size, location, tenderness and consistency. Investigations may include blood tests and biopsies, while management depends on whether an infectious or malignant cause is suspected, with infectious causes treated with antibiotics and possible biopsies for unchanged nodes or malignancy.