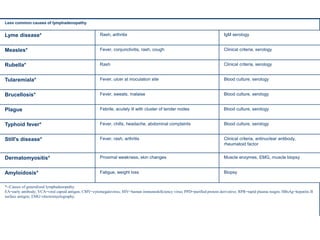
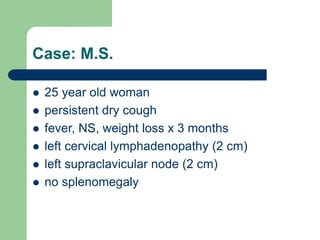
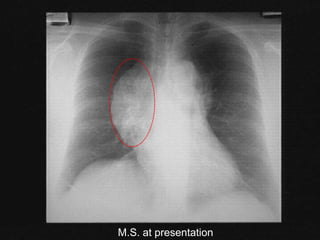
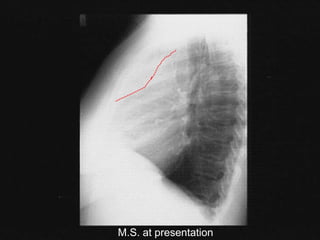
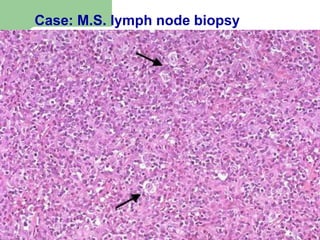
This document discusses lymphadenopathy and provides information about evaluating and diagnosing causes of lymphadenopathy. It begins by defining lymphadenopathy and describing classifications such as localized versus generalized. For patients presenting with unexplained lymphadenopathy, approximately 3/4 will have localized lymphadenopathy while 1/4 will have generalized. The document then discusses evaluating the history, performing a physical exam, potential causes of lymphadenopathy, and guidelines for biopsy of localized versus generalized lymphadenopathy. It also provides a case study of a patient, M.S., who presented with lymphadenopathy and was ultimately diagnosed with Stage IIB nodular sclerosis Hodgkin's lymphoma.