Download to read offline


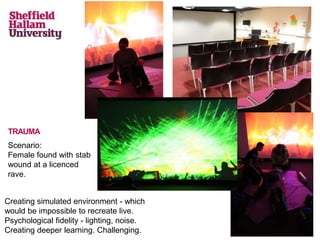
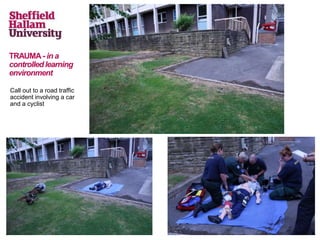
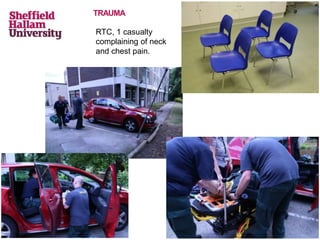

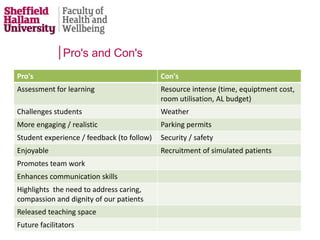

The document discusses using simulation training to prepare paramedic students for real-life scenarios. It describes using various locations around campus to simulate different emergency situations like traffic accidents, stabbings, and falls. Students responded positively to the realistic scenarios, saying it improved their learning compared to traditional classroom simulations. The effort put into the realistic simulations was appreciated and students felt it better prepared them for practice, built their confidence, and allowed them to adapt guidelines to new situations.