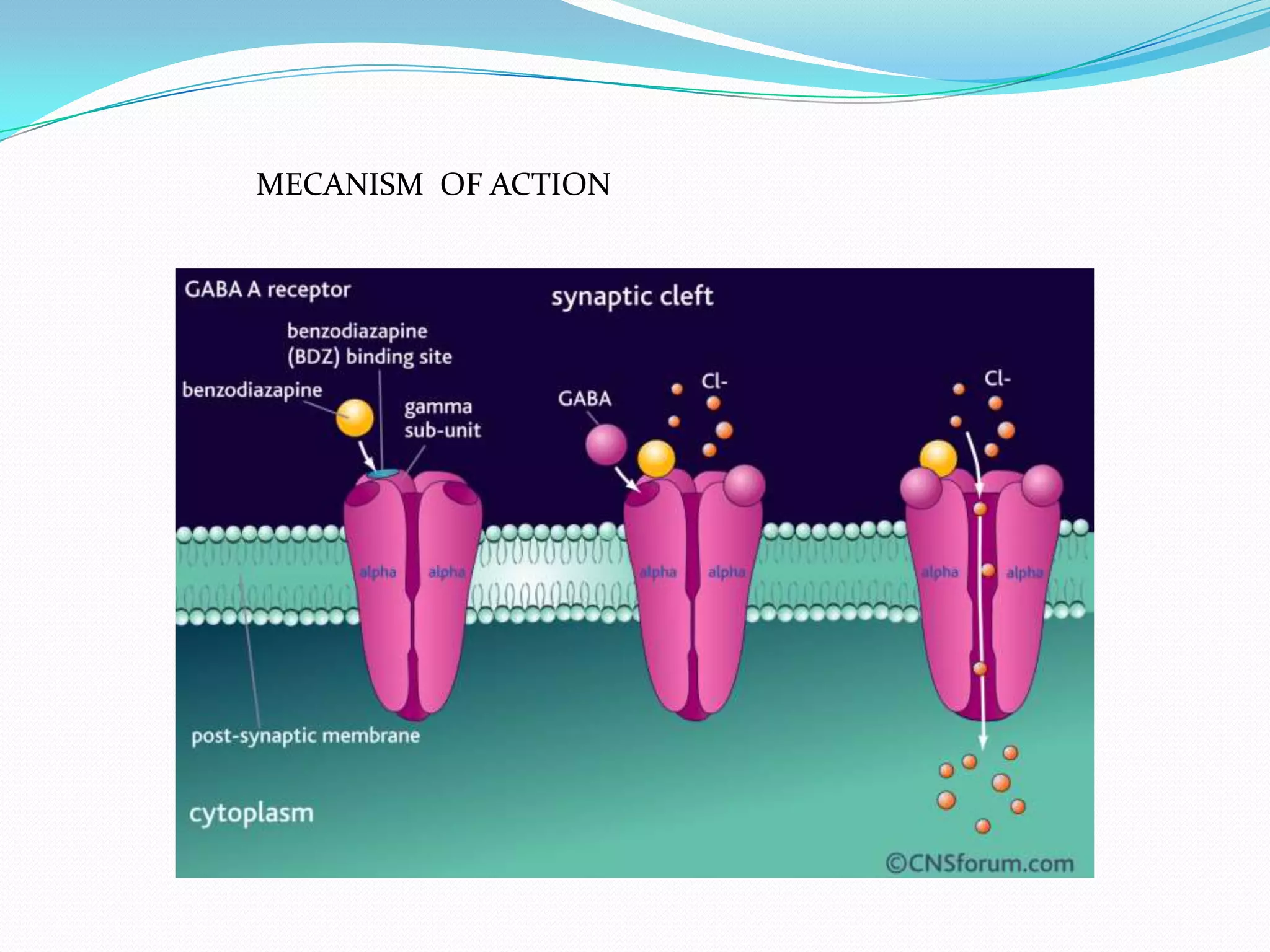
Anxiety disorders are characterized by excessive anxiety and associated symptoms that impair functioning. There are several types, including generalized anxiety disorder, social anxiety disorder, and post-traumatic stress disorder. Physiologically, anxiety disorders are linked to abnormalities in neurotransmitter systems like norepinephrine, GABA, and serotonin. Symptoms vary by disorder but can include excessive worry, poor concentration, restlessness, sleep issues, sweating, and fast heartbeat. Diagnosis involves medical exams and ruling out other potential causes. Treatment includes counseling, stress management, exercise, benzodiazepines, antidepressants, and beta blockers, though these carry side effects like sedation and nausea.