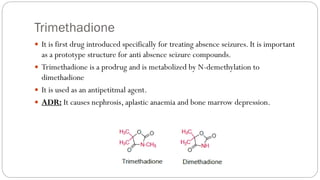
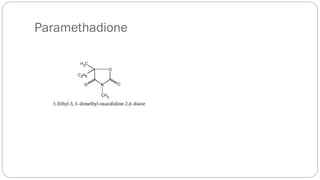
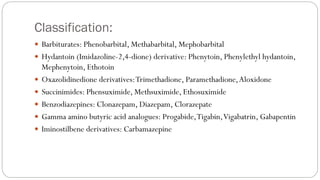
This document provides information on various classes of anticonvulsant drugs, including their mechanisms of action and uses. It discusses barbiturates like phenobarbital, hydantoins like phenytoin, oxazolidinediones like trimethadione, succinimides like ethosuximide, carbamazepine, clonazepam, and gabapentin. It also covers the classification, mechanisms, structure-activity relationships, metabolism, and adverse reactions of these anticonvulsants used to treat epilepsy disorders like absence seizures, partial seizures, and tonic-clonic seizures.


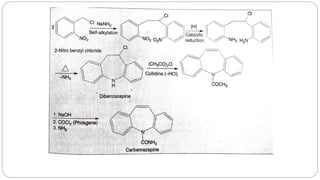
![Iminostilbene derivatives: Carbamazepine (CBZ)
CBZ, 5H dibenz[b,f]lazepine 5 carboxamide is an iminostilbene derivative of tricyclic
antidepressants
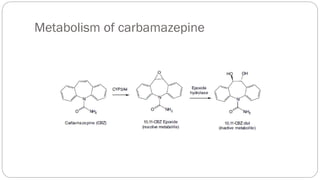
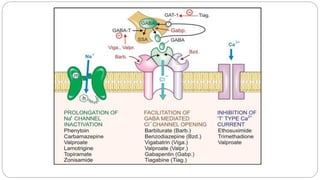
MOA: Inhibits voltage dependent-sodium channels (same as phenytoin)
USE: One of the safest and most effective older anti-epileptic drugs
1. Indicated as initial or adjunct therapy for complex partial, tonic-clonic and mixed type
seizures.
2. Used in the treatment of trigeminal neuralgia
ADR: Common toxicities include blurred vision, dizziness, drowsiness and ataxia.
Tremor, depression, hyponatremia, and cardiac disturbances are seen at high serum
concentrations.
Severe idiosyncratic reactions including aplastic anemia, agranulocytosis, thrombocytopenia
and jaundice](https://image.slidesharecdn.com/anticonvulsants11-230617153609-3a13564f/85/ANTICONVULSANTS-1-1-pdf-22-320.jpg)