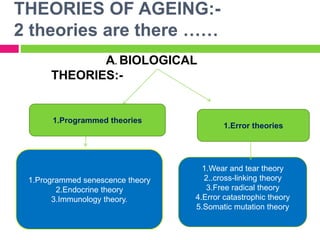
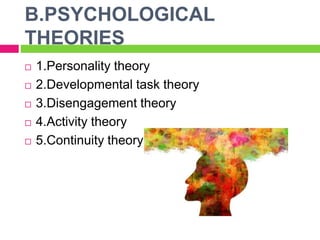
This presentation summarizes key topics related to geriatric nursing. It introduces the speaker and defines geriatrics as the branch of medicine focusing on healthcare for elderly individuals. The document then outlines several theories of aging, including programmed, error, biological, and psychological theories. It also discusses common physiological changes in cardiovascular, pulmonary, and other body systems associated with aging. The presentation provides an overview of important concepts and trends in geriatric nursing.