Downloaded 1,010 times




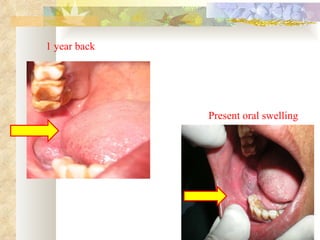
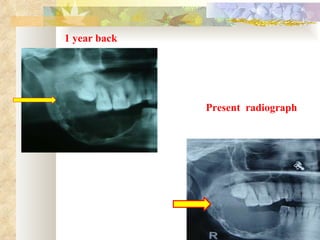
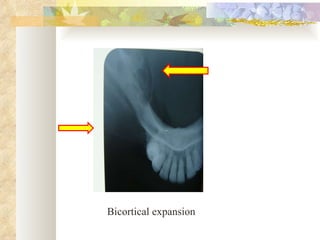
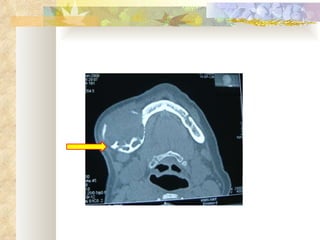

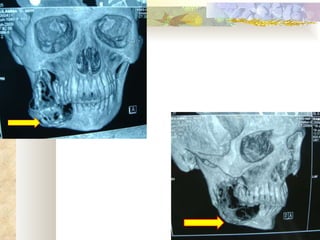

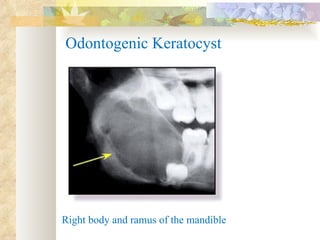




The document reports a case of ameloblastoma in a 60-year old female patient. She presented with a swelling on her right cheek that had been growing over the past 2 years. Radiological investigations including OPG and CT scans showed a bicortical expanding lesion in the right body and ramus of the mandible. An incisional biopsy was performed and the provisional diagnosis of ameloblastoma was made.



































































