Download as PDF, PPTX


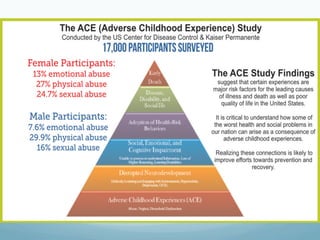

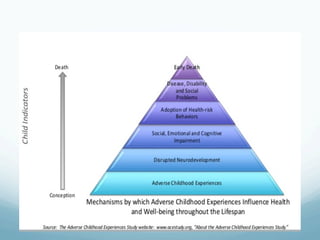
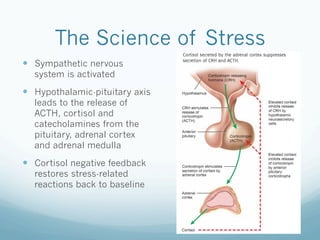






The UC San Diego Antiviral Research Center conducts weekly presentations to share the latest research on infectious diseases like HIV, emphasizing education for clinicians and researchers. The document includes case studies on patients such as Maria and Marcus, detailing their struggles with adherence and the effects of trauma on health outcomes. It explores the psychological impact of stress and trauma, particularly in the context of childhood abuse and its correlation with poor health and HIV-related challenges.




































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















