Downloaded 13 times


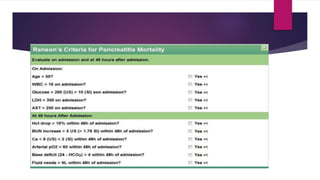
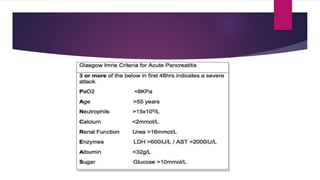
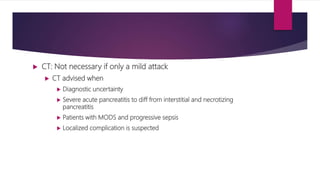
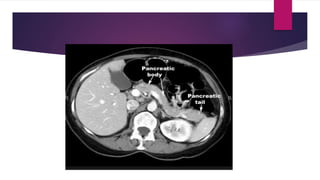
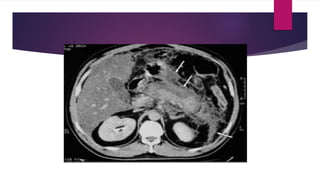


This document provides an overview of pancreatitis, including: - It describes acute and chronic pancreatitis, with acute pancreatitis presenting with abdominal pain and elevated enzymes. - The mechanism involves premature enzyme activation leading to autodigestion and inflammation of the pancreas. - Signs, symptoms, and imaging findings are discussed for assessing severity and managing acute pancreatitis. Complications like fluid collections, necrosis, and abscesses are also covered. - Treatment involves conservative management for mild cases and intensive care, monitoring, antibiotics and drainage procedures for more severe cases.























































































