Download to read offline

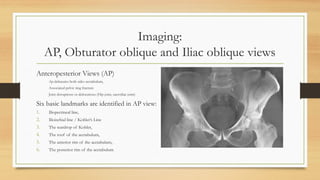
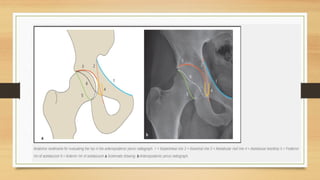
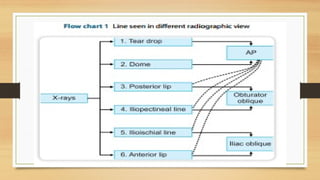




The document discusses acetabular fractures, detailing their definitions, mechanisms of injury, classification, and management strategies. It highlights the importance of imaging techniques, particularly CT scans, for assessing fractures and planning treatments, including both non-operative and operative approaches. The document also explores surgical techniques, postoperative care, and potential complications associated with acetabular fractures.



































































