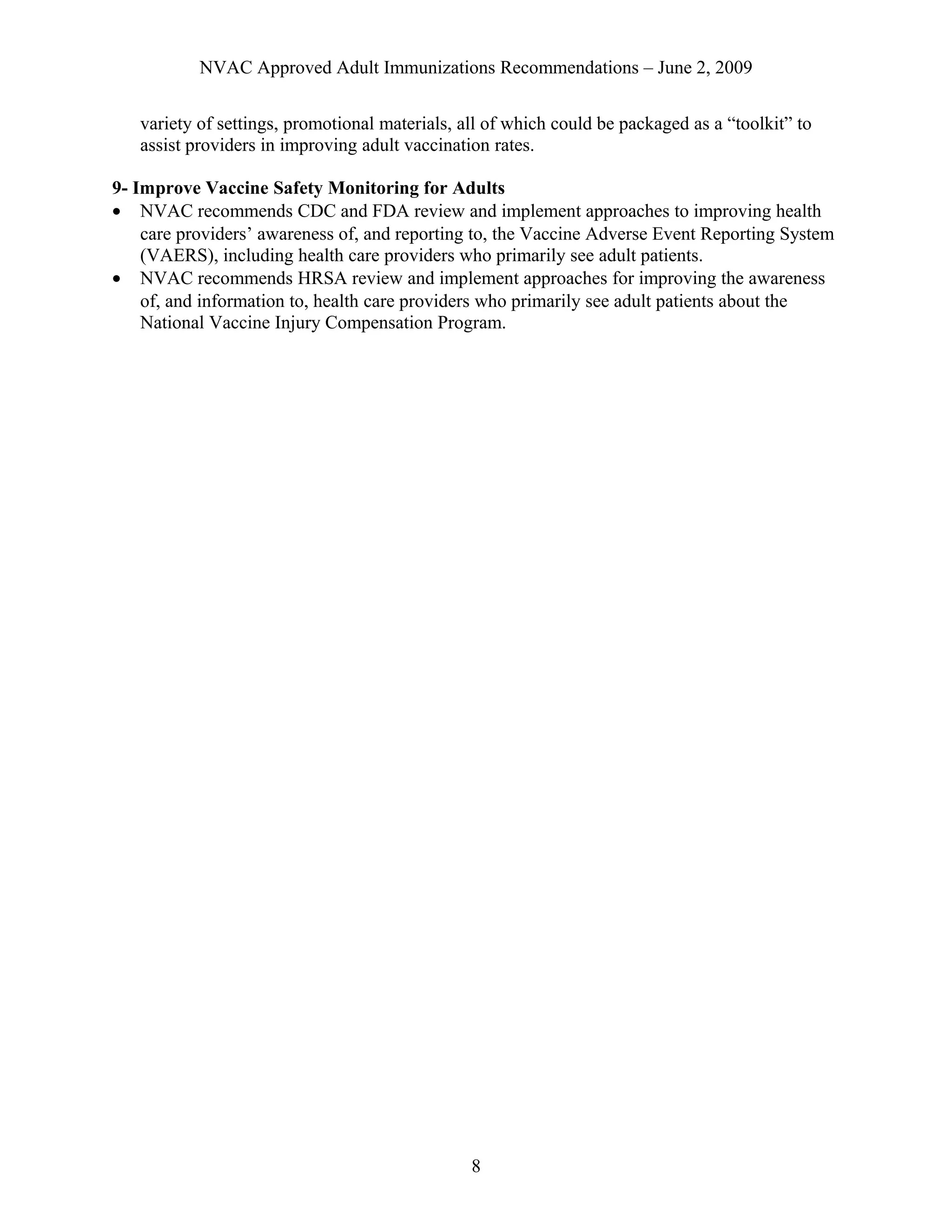
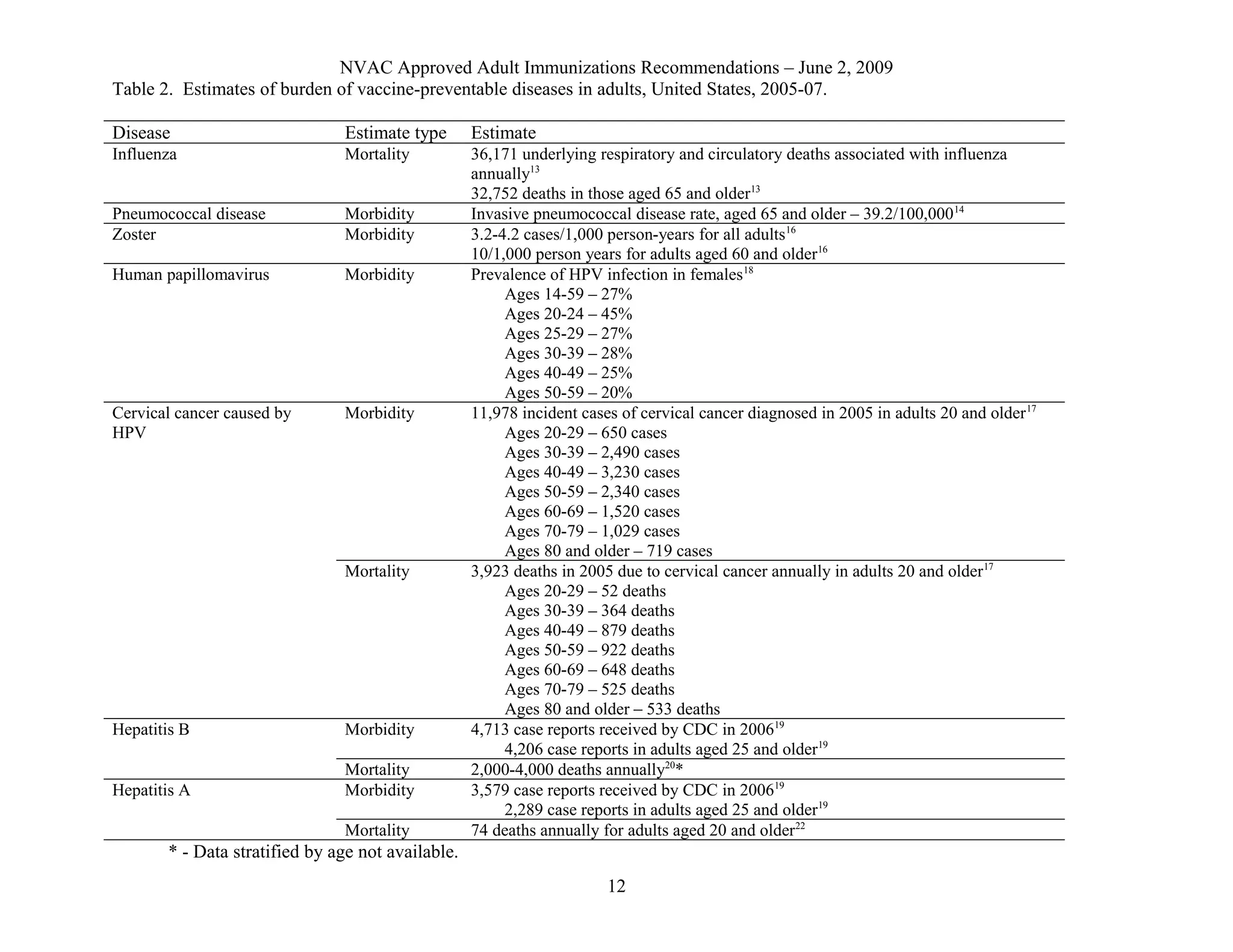
The document discusses recommendations from the National Vaccine Advisory Committee regarding adult immunization programs. It provides an overview of adult immunization levels and targets, noting that rates for influenza and pneumococcal vaccines have increased but remain below Healthy People 2010 goals. Burden of vaccine-preventable diseases in adults is significant, with estimates of tens of thousands of influenza-associated deaths annually in the US. Recommendations focus on improving coordination, evaluation, and collaboration across federal agencies to increase adult vaccination uptake.

![NVAC Approved Adult Immunizations Recommendations – June 2, 2009
References
1. National Vaccine Advisory Committee. Report of the Subcommittee on Adult
Immunization. 1990 [cited 8 Apr 2009]. Available from
http://www.hhs.gov/nvpo/nvac/Adult%20Immunization%202-90.pdf.
2. National Vaccine Advisory Committee. Adult Immunization: A report by the National
Vaccine Advisory Committee. 1994 [cited 8 Apr 2009]. Available from
http://www.hhs.gov/nvpo/nvac/AdultImmunization194.pdf.
3. Centers for Disease Control and Prevention. Adult immunization programs in
nontraditional settings: quality standards and guidance for program evaluation – a report
of the National Vaccine Advisory Committee and Use of standing orders programs to
increase adult vaccination rates: recommendations of the Advisory Committee on
Immunization Practices. MMWR 2000;49(RR-1):1-13.
4. Advisory Committee on Immunization Practices. Recommended adult immunization
schedule: United States, 2009. Ann Intern Med. 2009;150:40-4.
5. Department of Health and Human Services. Healthy People 2010: 14: Immunization and
Infectious Diseases. 2000 [cited 8 Apr 2009]. Available from
http://healthypeople.gov/document/pdf/Volume1/14Immunization.pdf.
6. Centers for Disease Control and Prevention. Self-reported influenza vaccination
coverage trends 1989-2007 among adults by age group, risk group, race/ethnicity, health-
care worker status, and pregnancy status, United States, National Health Interview
Survey (NHIS). 2008 [cited 8 Apr 2009]. Available from
http://www.cdc.gov/flu/professionals/vaccination/pdf/NHIS89_07fluvaxtrendtab.pdf.
7. Centers for Disease Control and Prevention. Vaccination coverage among US adults –
National Immunization Survey-Adult, 2007. 2008 [cited 8 Apr 2009]. Available from
http://www.cdc.gov/vaccines/stats-surv/nis/downloads/nis-adult-summer-2007.pdf.
8. Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System
Prevalence and Trends Data – Adults aged 65+ who have had a flu shot within the past
year. 2008 [cited 8 Apr 2009]. Available from
http://apps.nccd.cdc.gov/brfss/display.asp?cat=IM&yr=2007&qkey=4407&state=US.
9. Centers for Disease Control and Prevention. Self-reported pneumococcal vaccination
coverage trends 1989-2007 among adults by age group, risk group, race/ethnicity, health-
care worker status, and pregnancy status, United States, National Health Interview
Survey (NHIS). 2008 [cited 8 Apr 2009]. Available from
http://www.cdc.gov/flu/professionals/vaccination/pdf/NHIS89_07ppvvaxtrendtab.pdf.
10. Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System
Prevalence and Trends Data – Adults aged 65+ who have ever had a pneumonia
vaccination. 2008 [cited 8 Apr 2009]. Available from
http://apps.nccd.cdc.gov/brfss/display.asp?cat=IM&yr=2007&qkey=4408&state=US.
11. Centers for Disease Control and Prevention. Vaccination coverage among adolescents
aged 13-17 years – United States, 2007. MMWR 2008;57(40):1100-3.
12. Thompson WW, Shay DK, Weintraub E, et al. Mortality associated with influenza and
respiratory syncytial virus in the United States. JAMA 2004;289(2):179-86.
9](https://image.slidesharecdn.com/88881295-program-150908151620-lva1-app6891/75/88881295-program-9-2048.jpg)
![NVAC Approved Adult Immunizations Recommendations – June 2, 2009
13. Thompson WW, Weintraub E, Dhankhar P, et al. Estimates of US influenza-associated
deaths made using four different methods. Influenza Other Respir Viruses. 2009;3:37-
49.
14. Centers for Disease Control and Prevention. Active Bacterial Core Surveillance (ABCs)
Report, Emerging Infections Network, Streptococcus pneumoniae 2007. available at
http://www.cdc.gov/ncidod/dbmd/abcs/survreports/spneu07.pdf, accessed April 12, 2007
15. Lexau CA, Lynfield R, Danila R, Pilishvili T, Facklam R, Farley MM, Harrison LH, Schaffner
W, Reingold A, Bennett NM, Hadler J, Cieslak PR, Whitney CG, for the ABCs Team. Changing
epidemiology of invasive pneumococcal disease among older adults in the era of pediatric
pneumococcal conjugate vaccine. JAMA 2005;294(16):2043-2051.
16. Centers for Disease Control and Prevention. Prevention of Herpes Zoster:
recommendations from the Advisory Committee on Immunization Practices (ACIP).
MMWR Recomm Rep 2008;57(RR-5):1-30.
17. U.S. Cancer Statistics Working Group. United States Cancer Statistics: 1999-2005
Incidence and Mortality Web-Based Report. Atlanta: U.S. Department of Health and
Human Services, Centers for Disease Control and Prevention and National Cancer
Institute. 2009 [cited 23 Apr 2009]. Available from http://www.cdc.gov/uscs.
18. Dunne EF, Unger ER, Sternberg M, et al. Prevalence of HPV infection among females in
the United States. JAMA 2007;297(8):813-9.
19. Centers for Disease Control and Prevention. Summary of Notifiable Diseases – United
State, 2006. MMWR 2008;55(53):1-100.
20. Centers for Disease Control and Prevention. Disease burden from Hepatitis A, B, and C
in the United States. 2008 [cited 8 Apr 2009]. Available from
http://www.cdc.gov/hepatitis/Statistics.htm#section3.
21. Centers for Disease Control and Prevention. Surveillance for acute viral hepatitis –
United States, 2006. Surveillance Summaries, March 21, 2008. MMWR 2008;57(No.
SS-2):
22. Vogt TM, Wise ME, Bell BP, et al. Declining hepatitis A mortality in the United States
during the era of hepatitis A vaccination. J Infect Dis 2008;197(9):1282-8.
10](https://image.slidesharecdn.com/88881295-program-150908151620-lva1-app6891/75/88881295-program-10-2048.jpg)

























































![Immunization concerns revised 3-2-2011 - final [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/immunizationconcerns-revised3-2-2011-finalcompatibilitymode-110304113251-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

![Immunization concerns revised 3-2-2011 - final [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/immunizationconcerns-revised3-2-2011-finalcompatibilitymode-110304113610-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)







































