Download to read offline
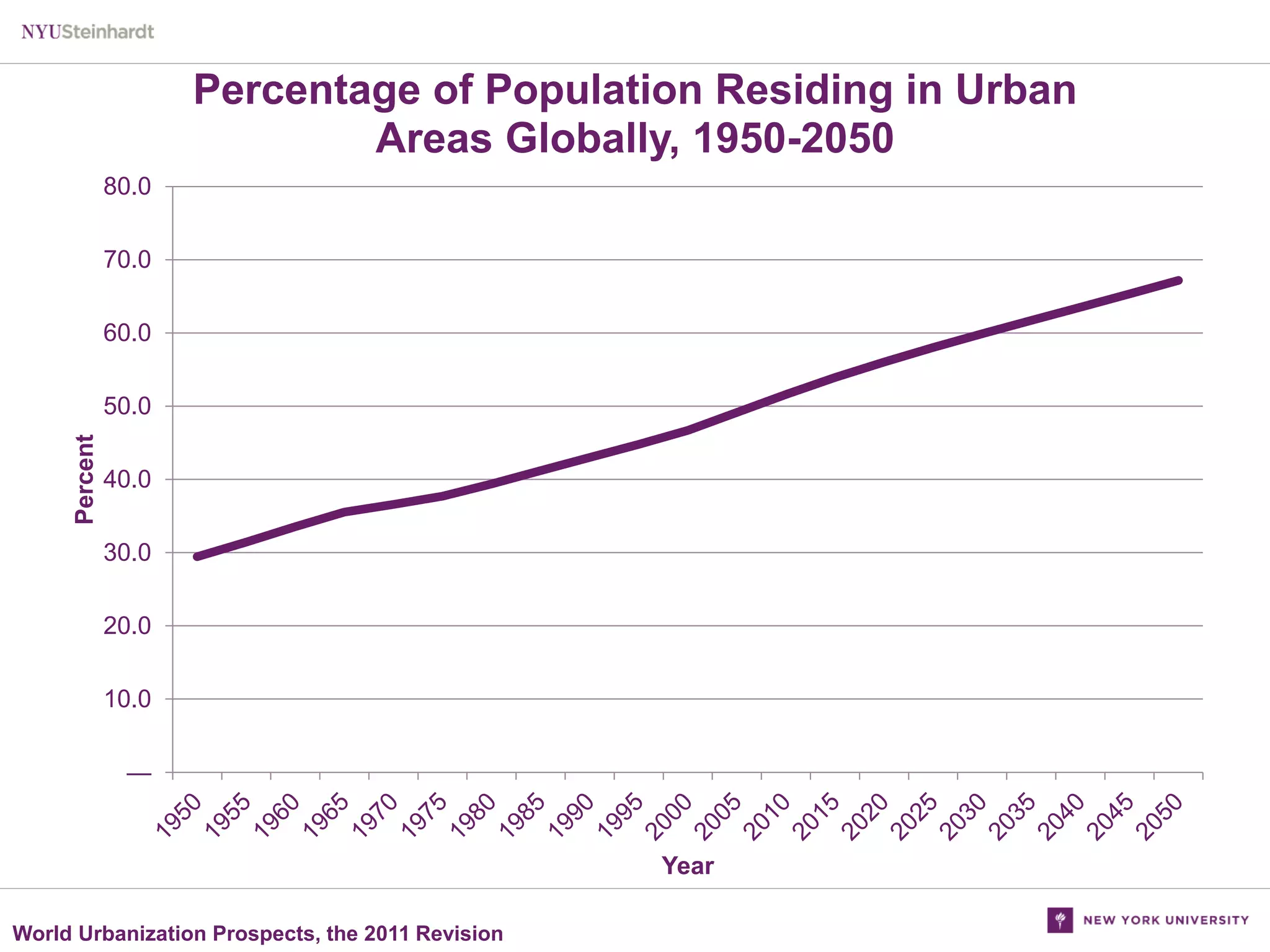
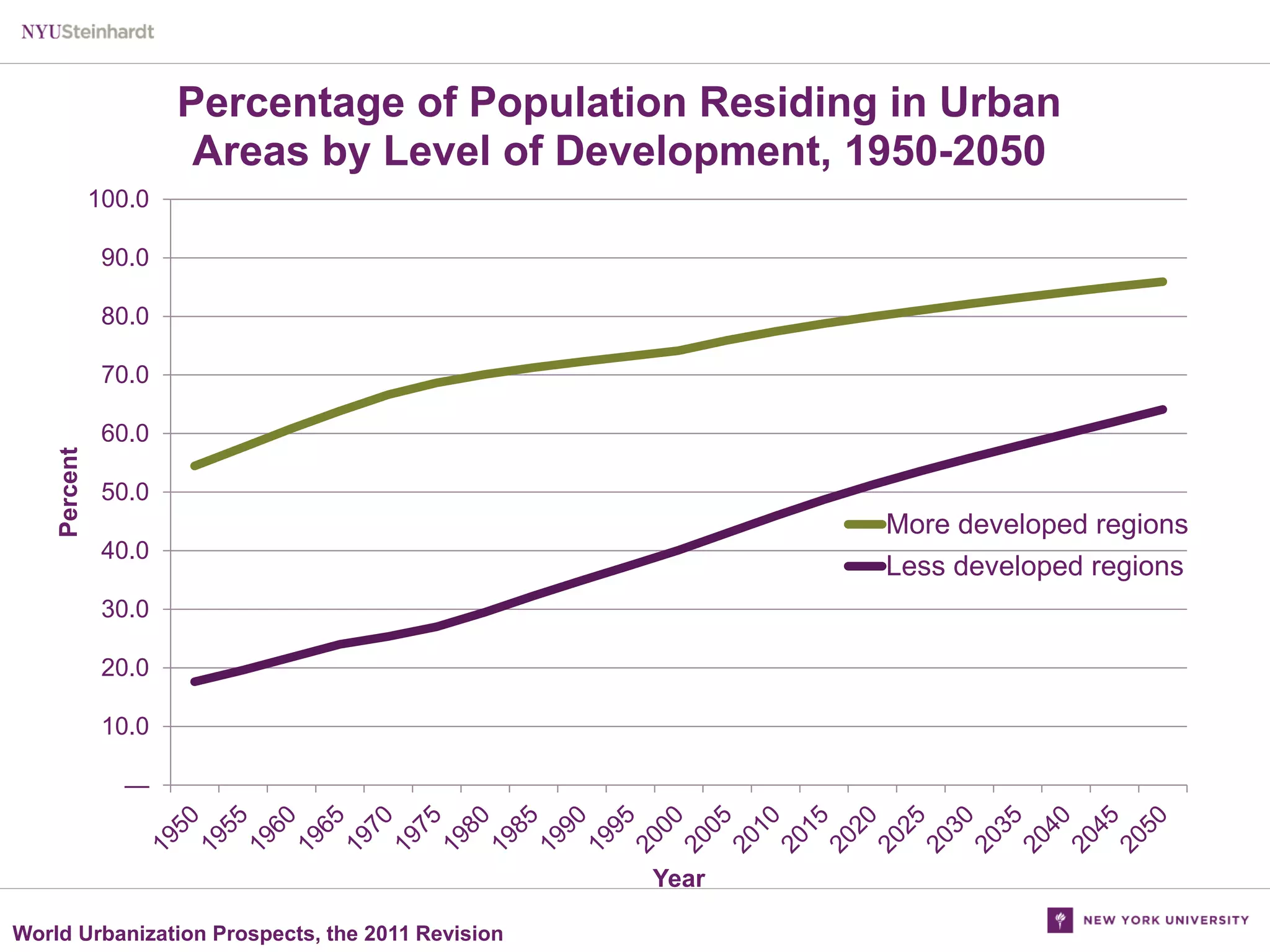
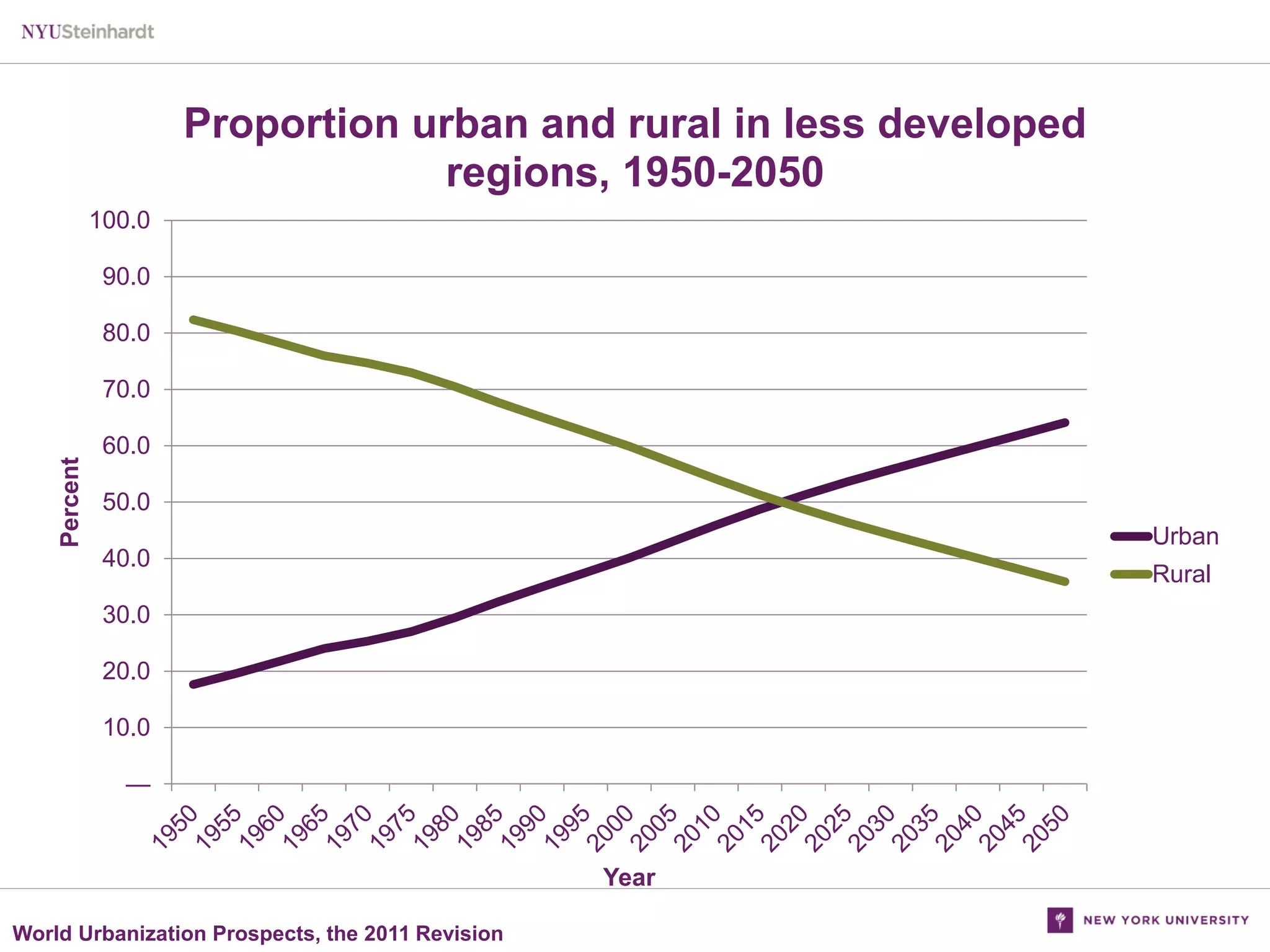
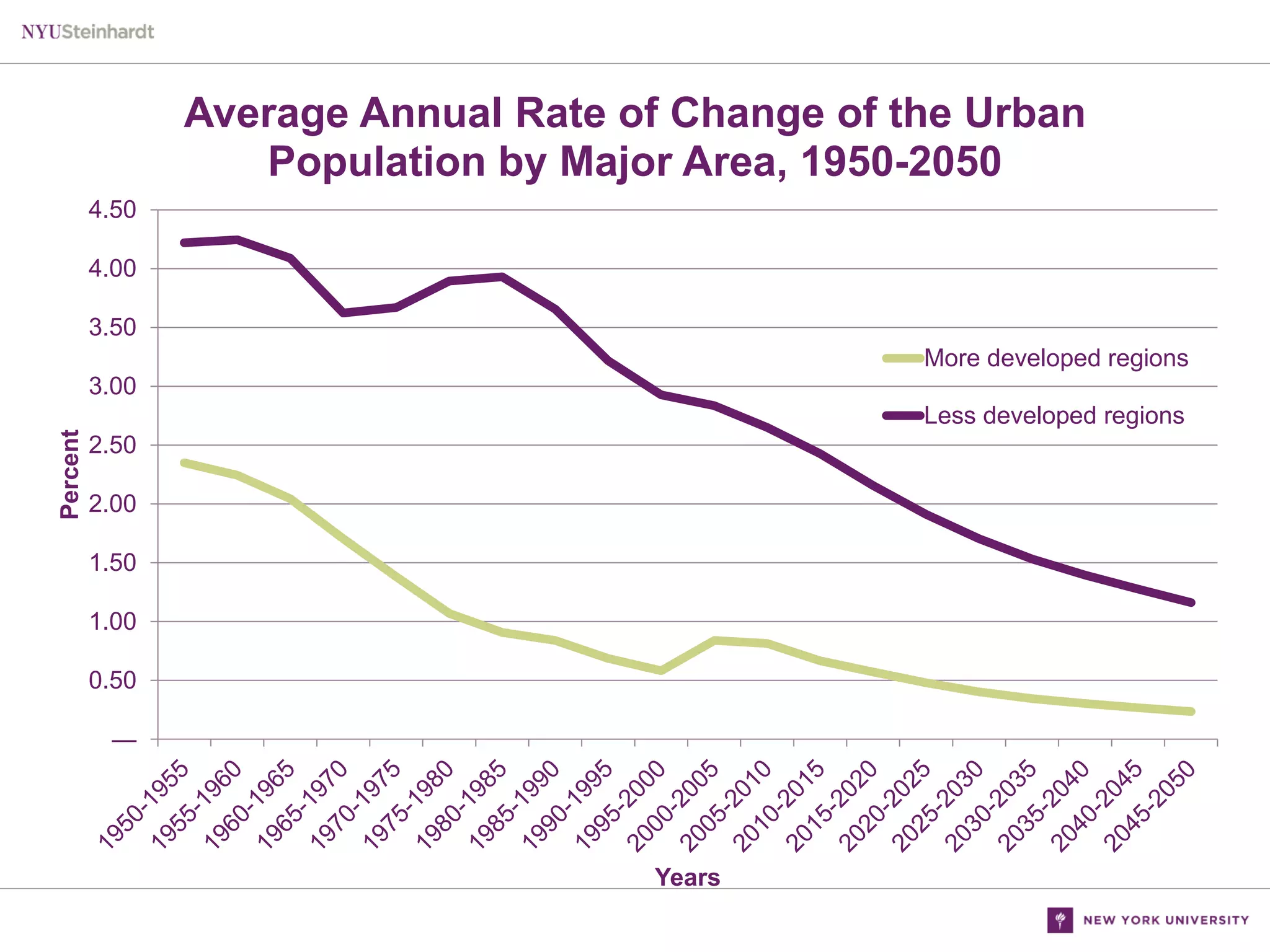
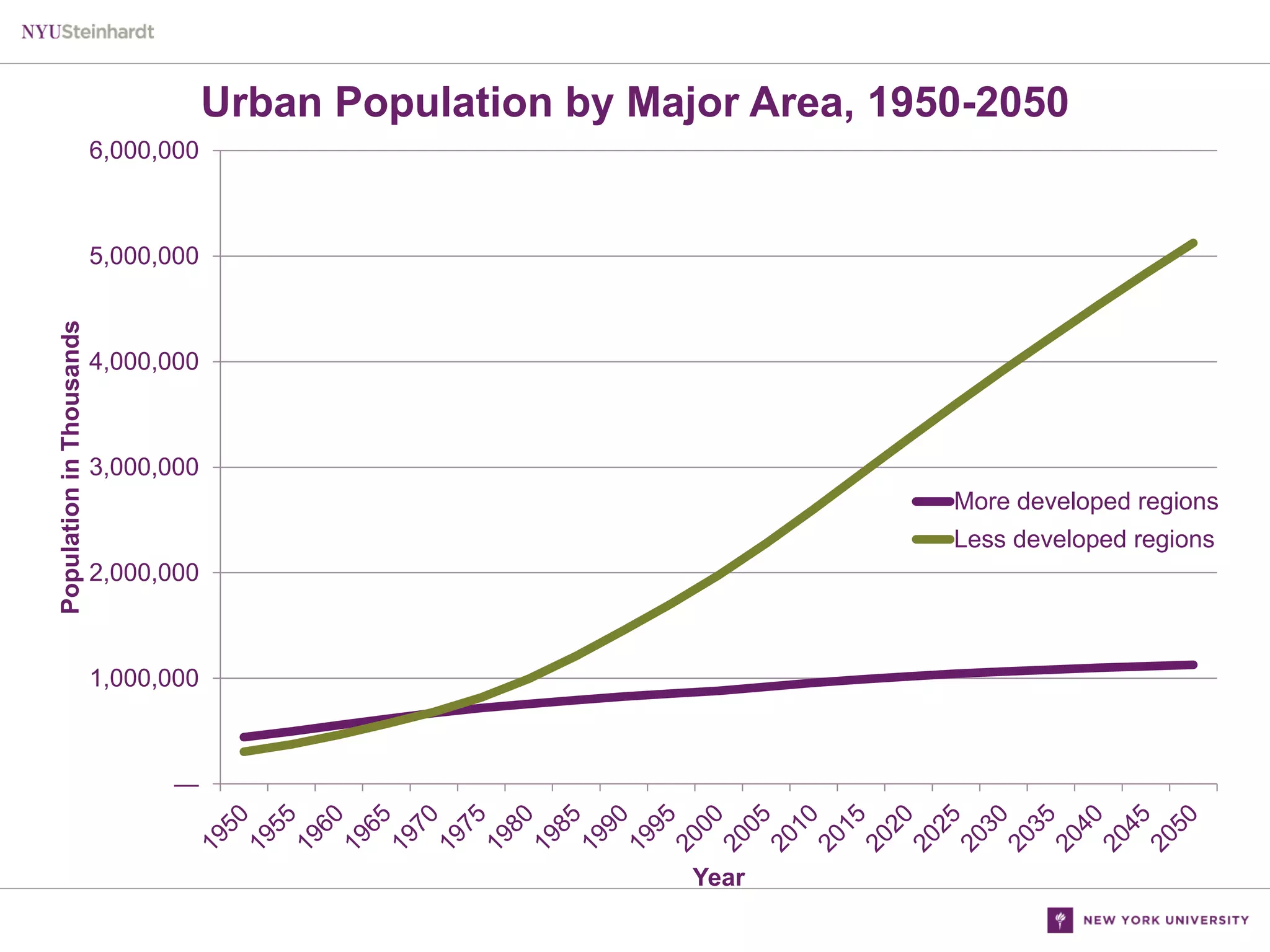
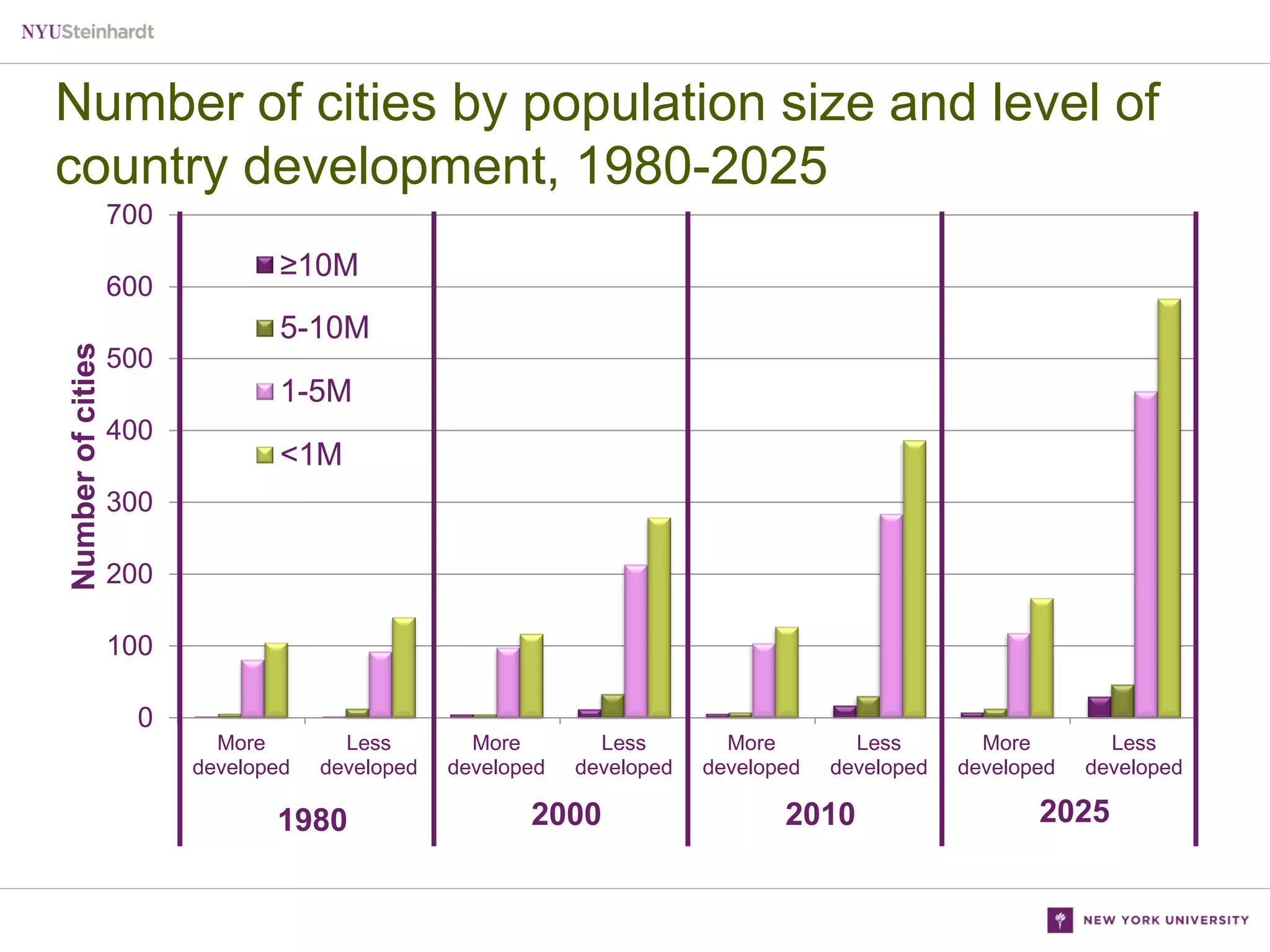










Urbanization is increasing globally, with more people living in urban areas. This presents challenges for distributing adult vaccines. The document reviews different strategies used in various settings to increase adult vaccination rates. Hospital/clinic-based interventions like standing orders and reminders showed success. Community-based programs distributing vaccines in non-traditional settings also increased rates. While many focused on the elderly, few targeted high-risk adults or children. A limitation is reaching those not engaged in healthcare.























































































