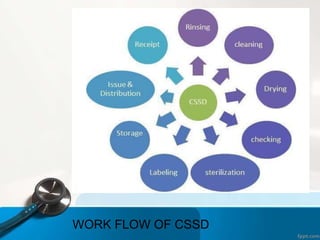
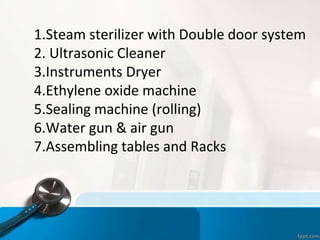
The document describes the Central Sterile Supply Department (CSSD) in a hospital. The CSSD receives, sterilizes, processes, packs, stores and distributes sterile and non-sterile supplies throughout the hospital. It has separate areas for receiving soiled supplies, cleaning, packing, sterilizing via steam or gas, storing sterile items temporarily, and distributing supplies to user departments. The CSSD aims to provide sterilized materials and reduce hospital infections through strict protocols and quality assurance measures during each step of the process.