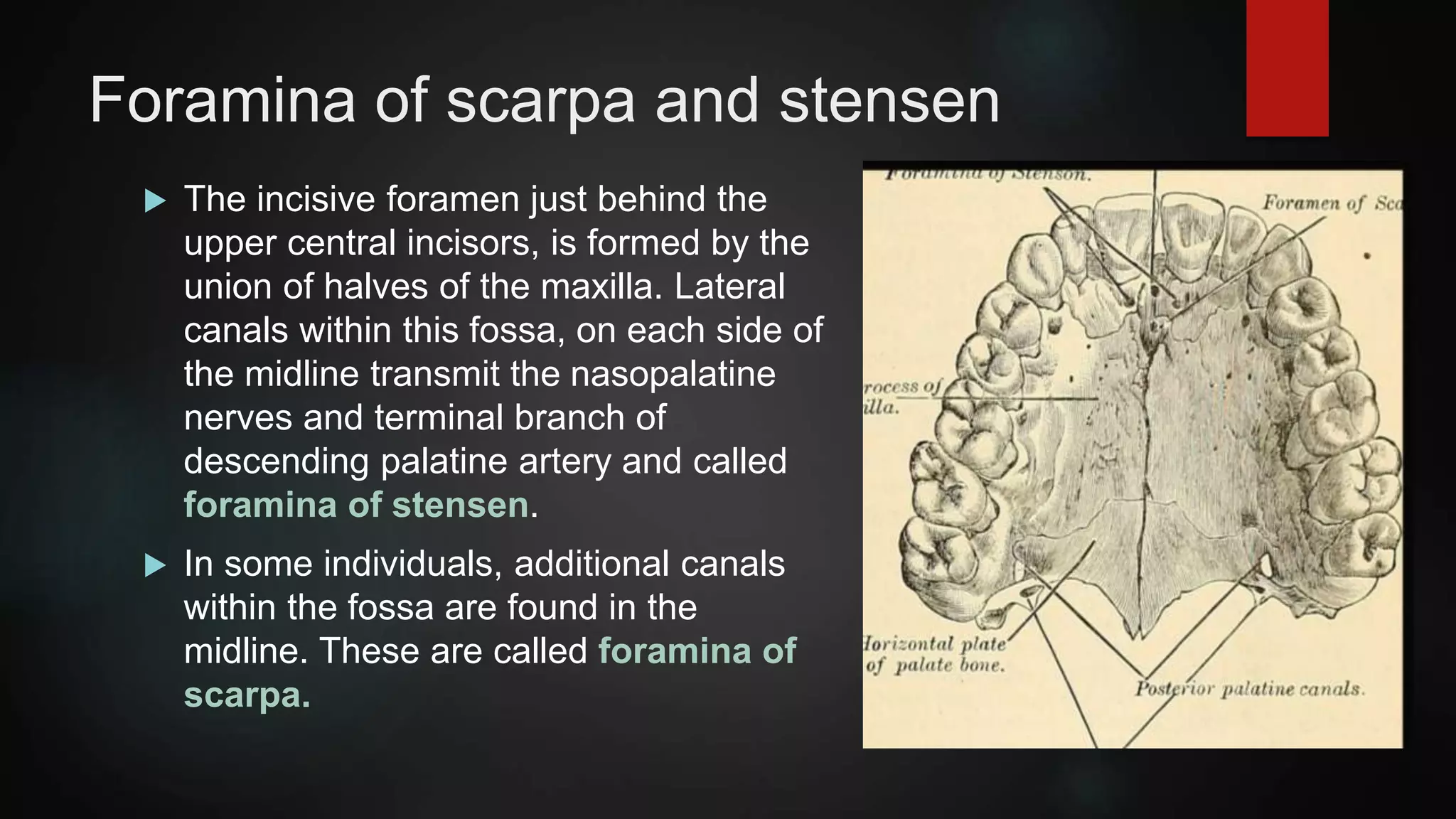
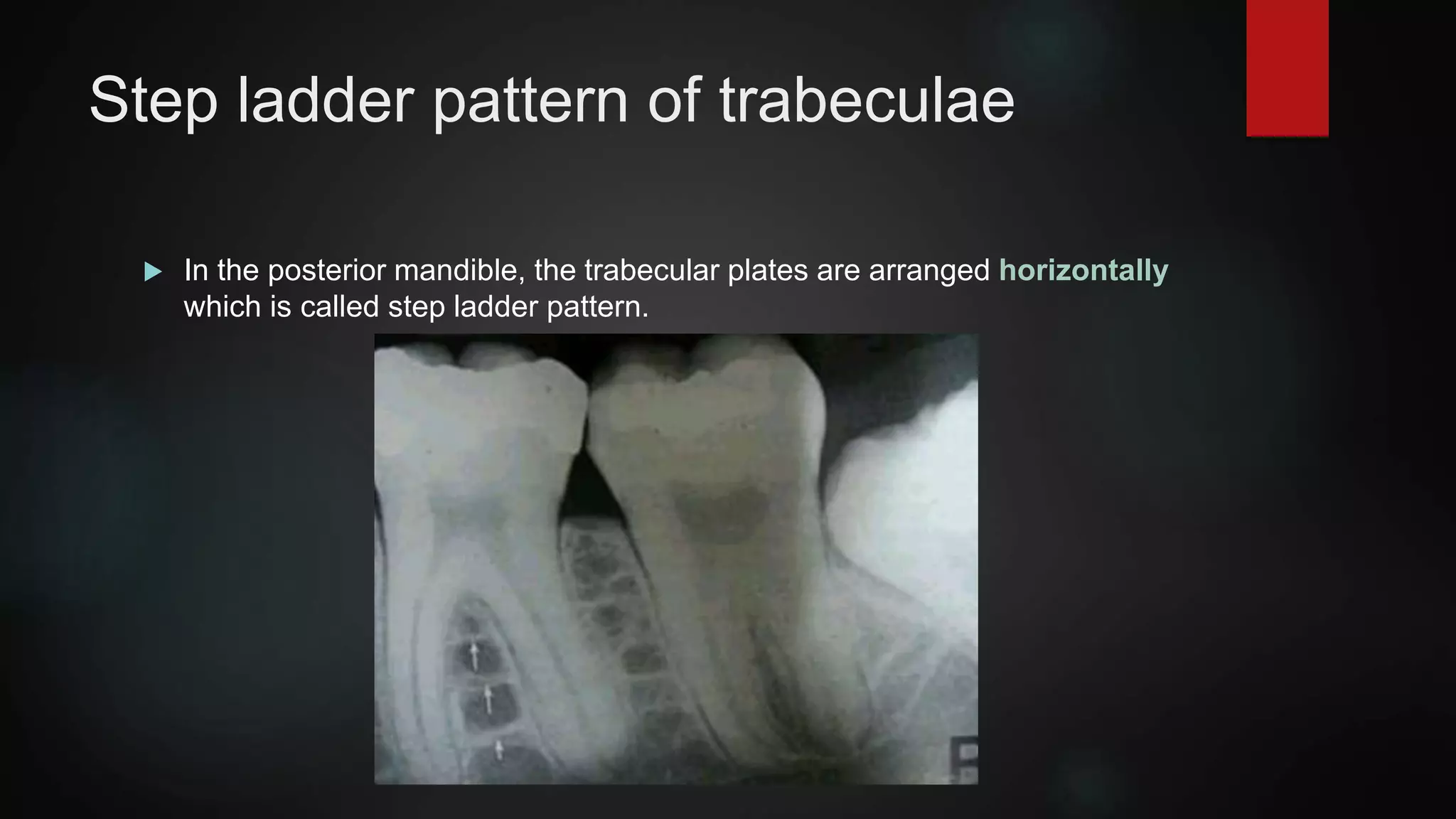
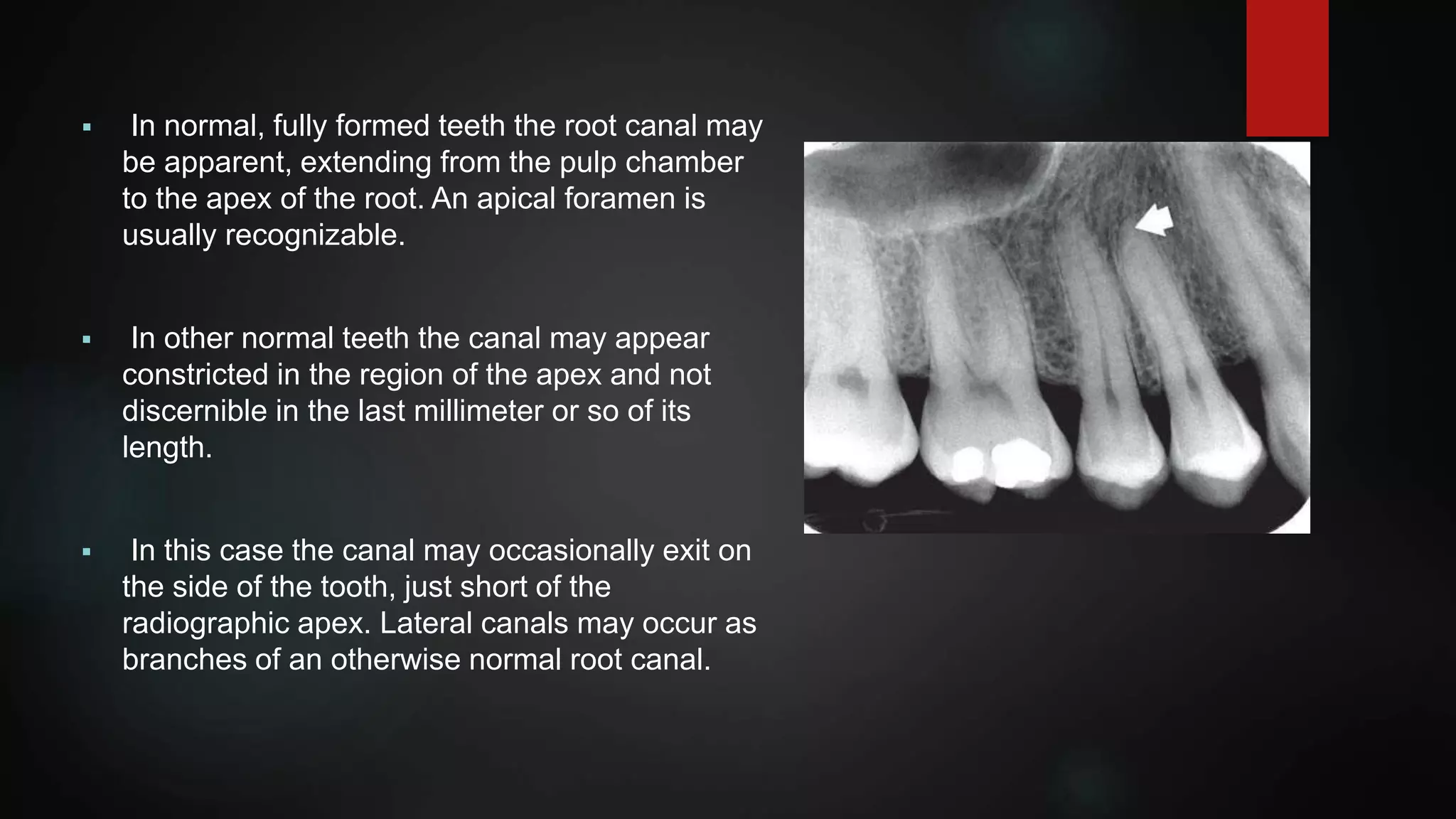
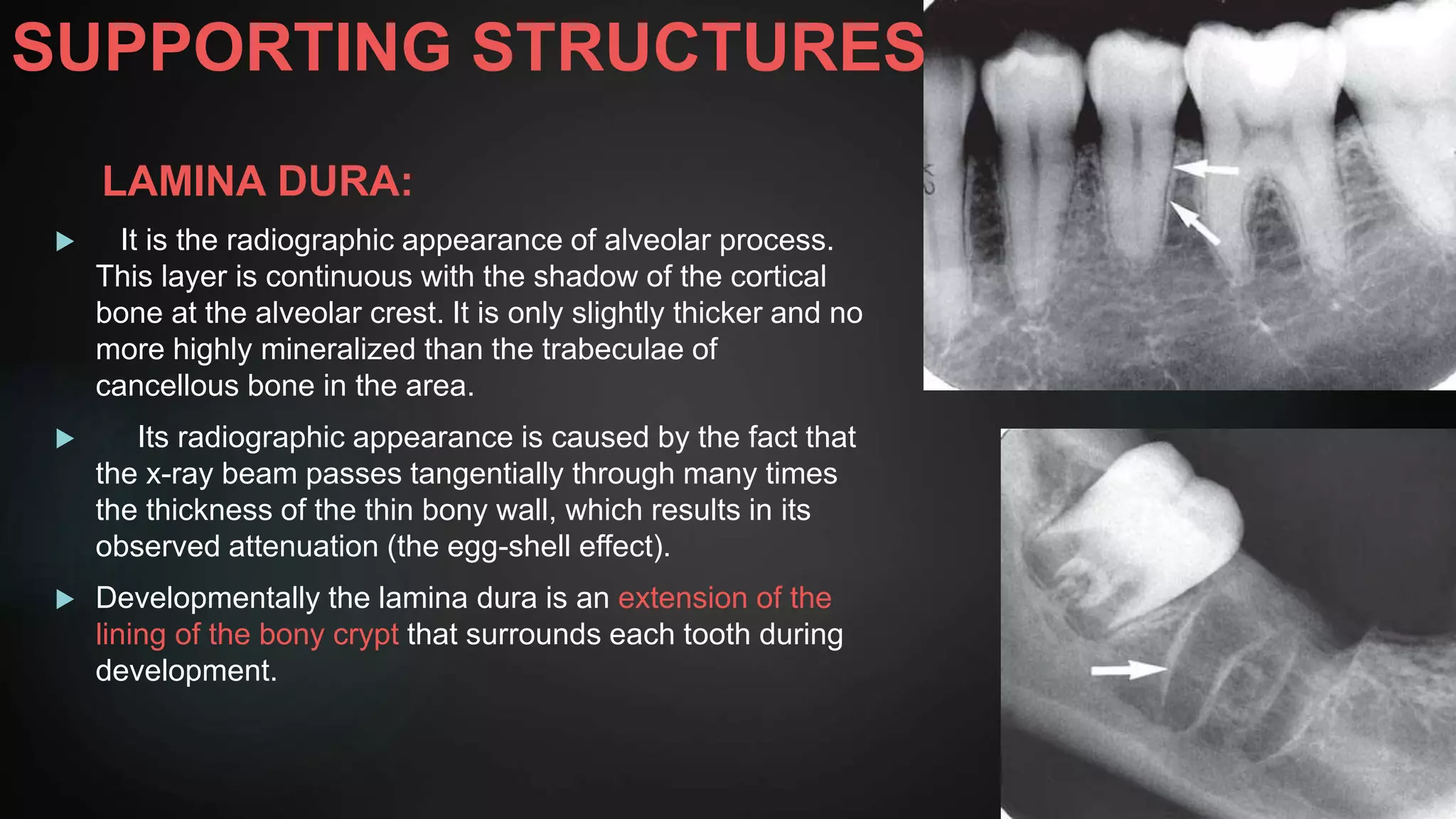
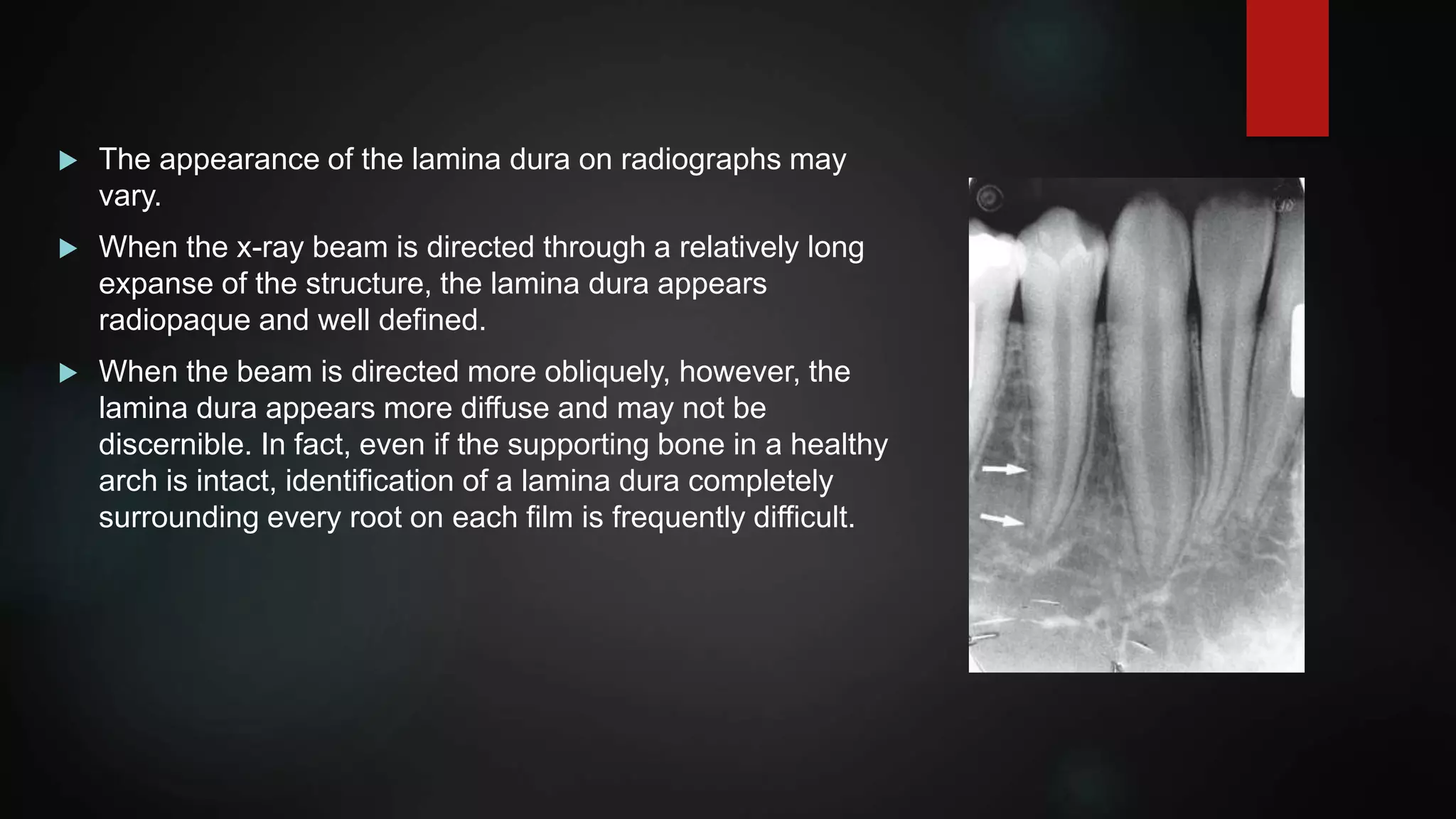
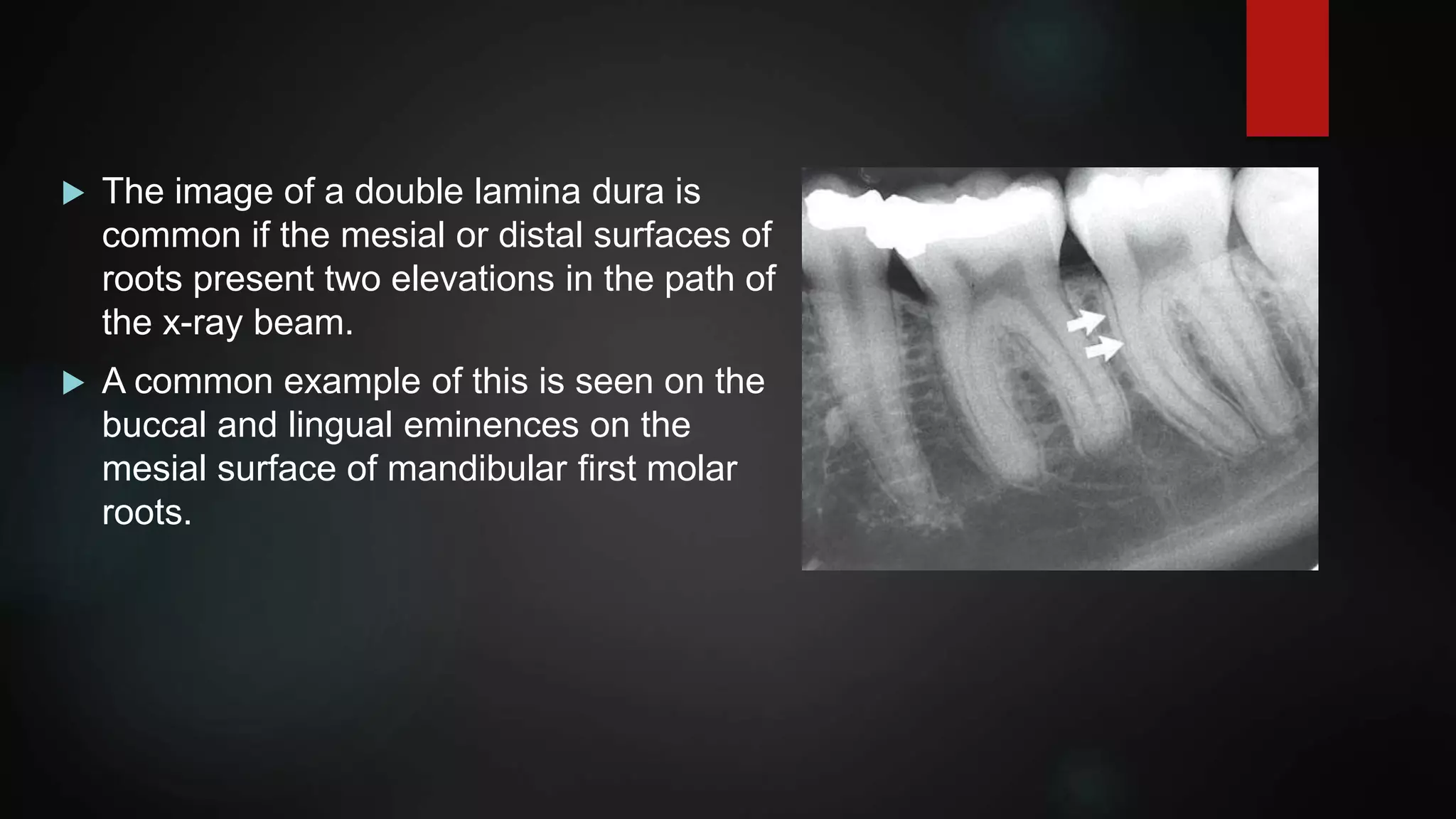
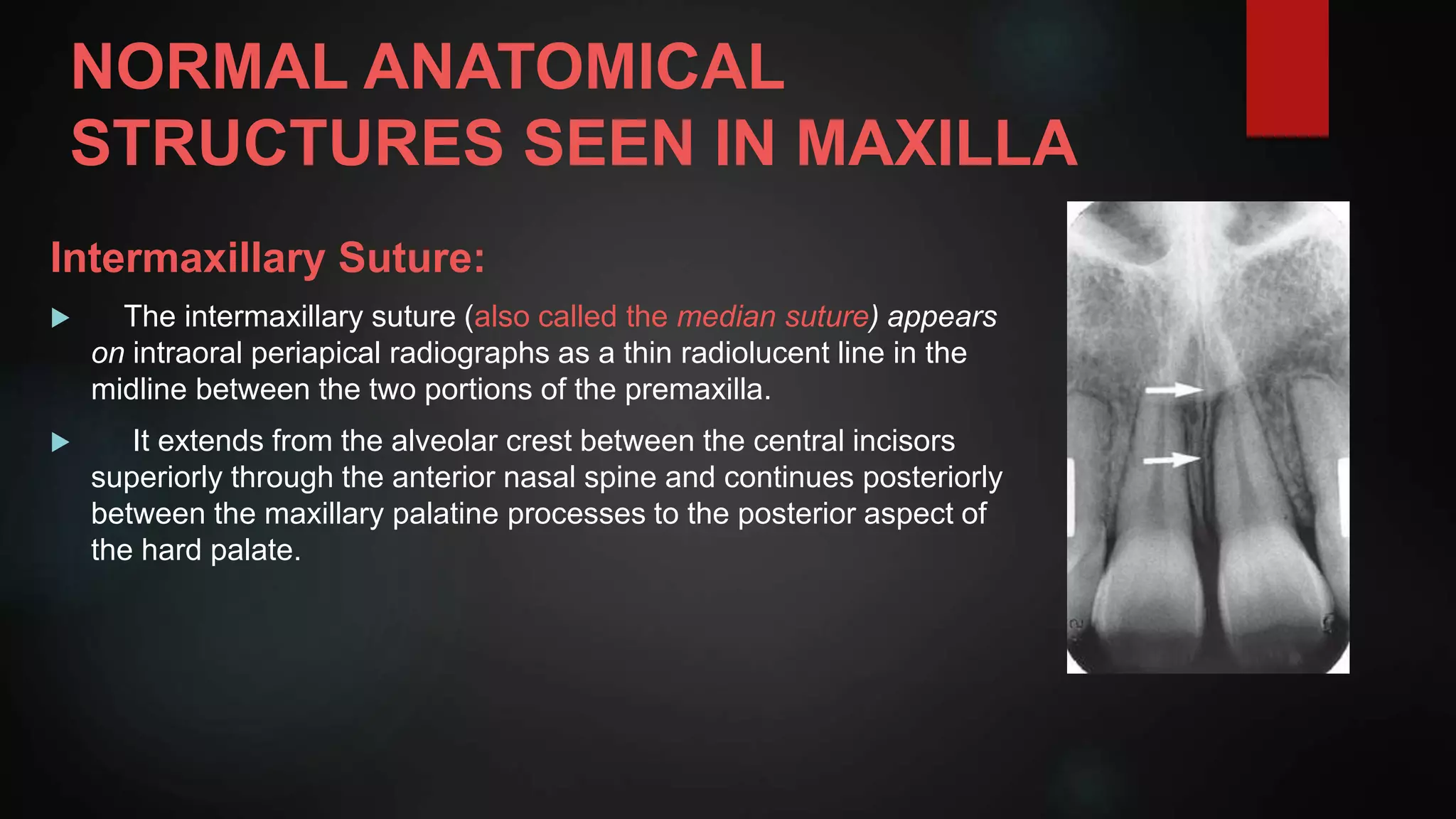
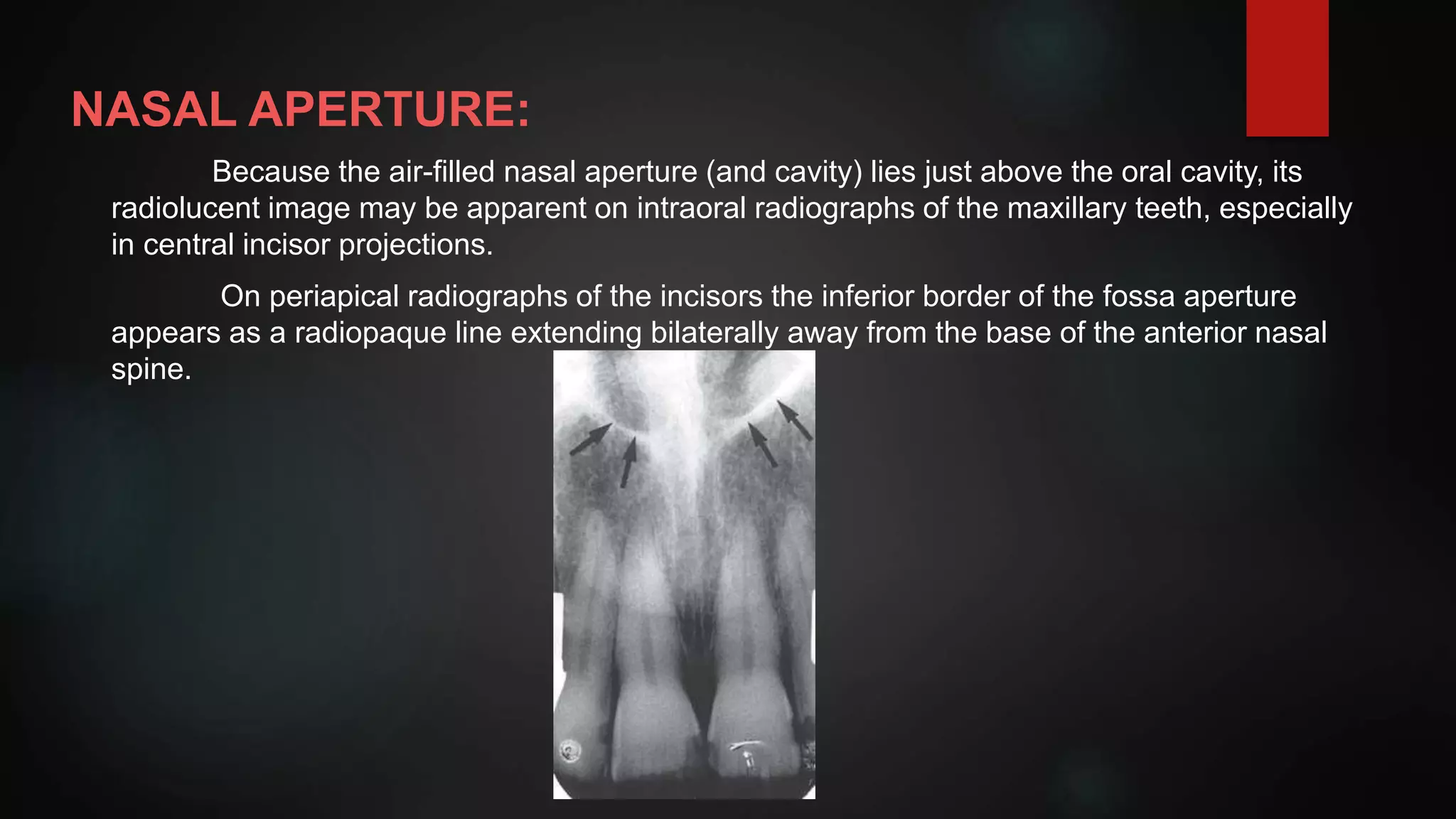
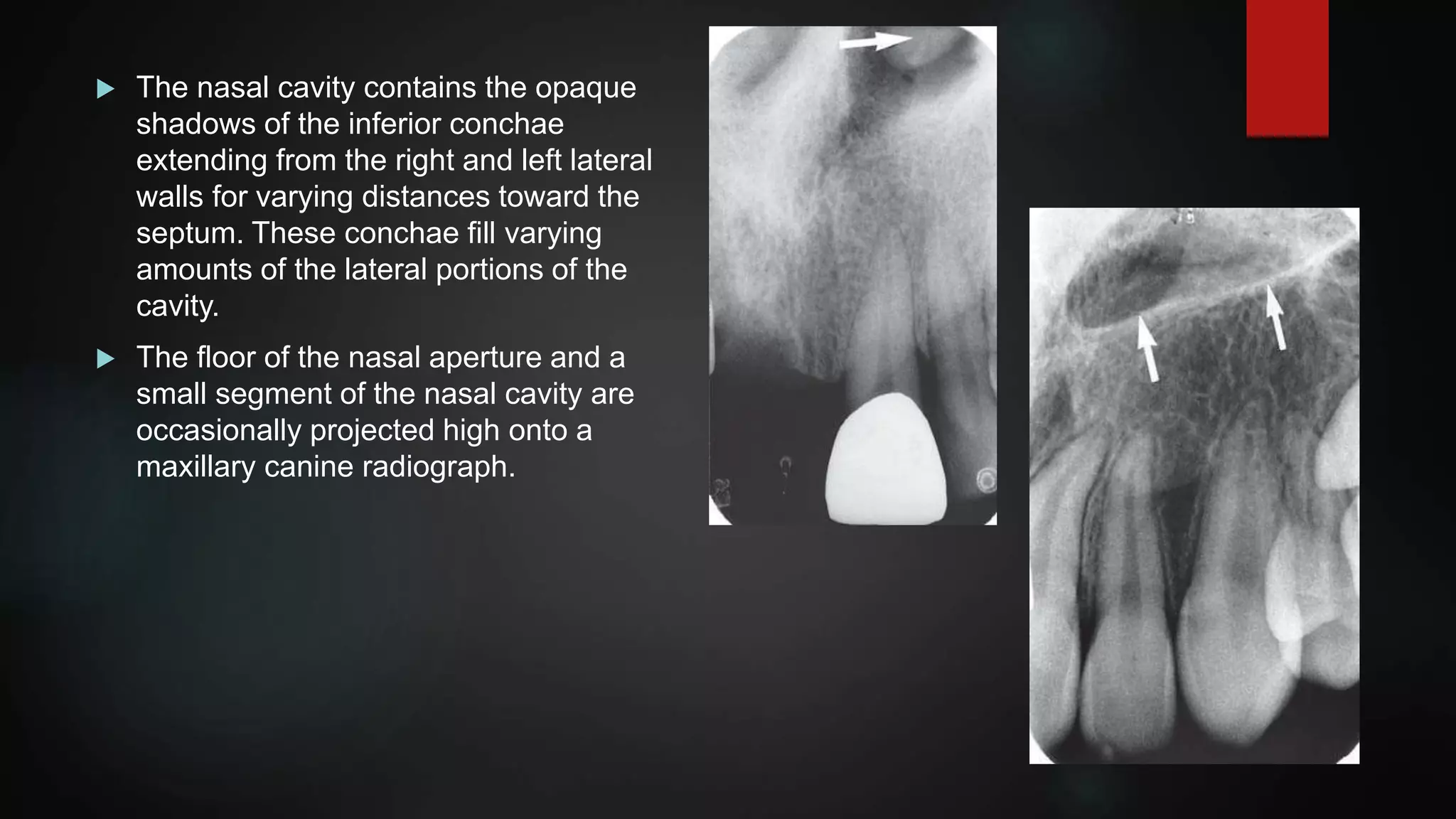
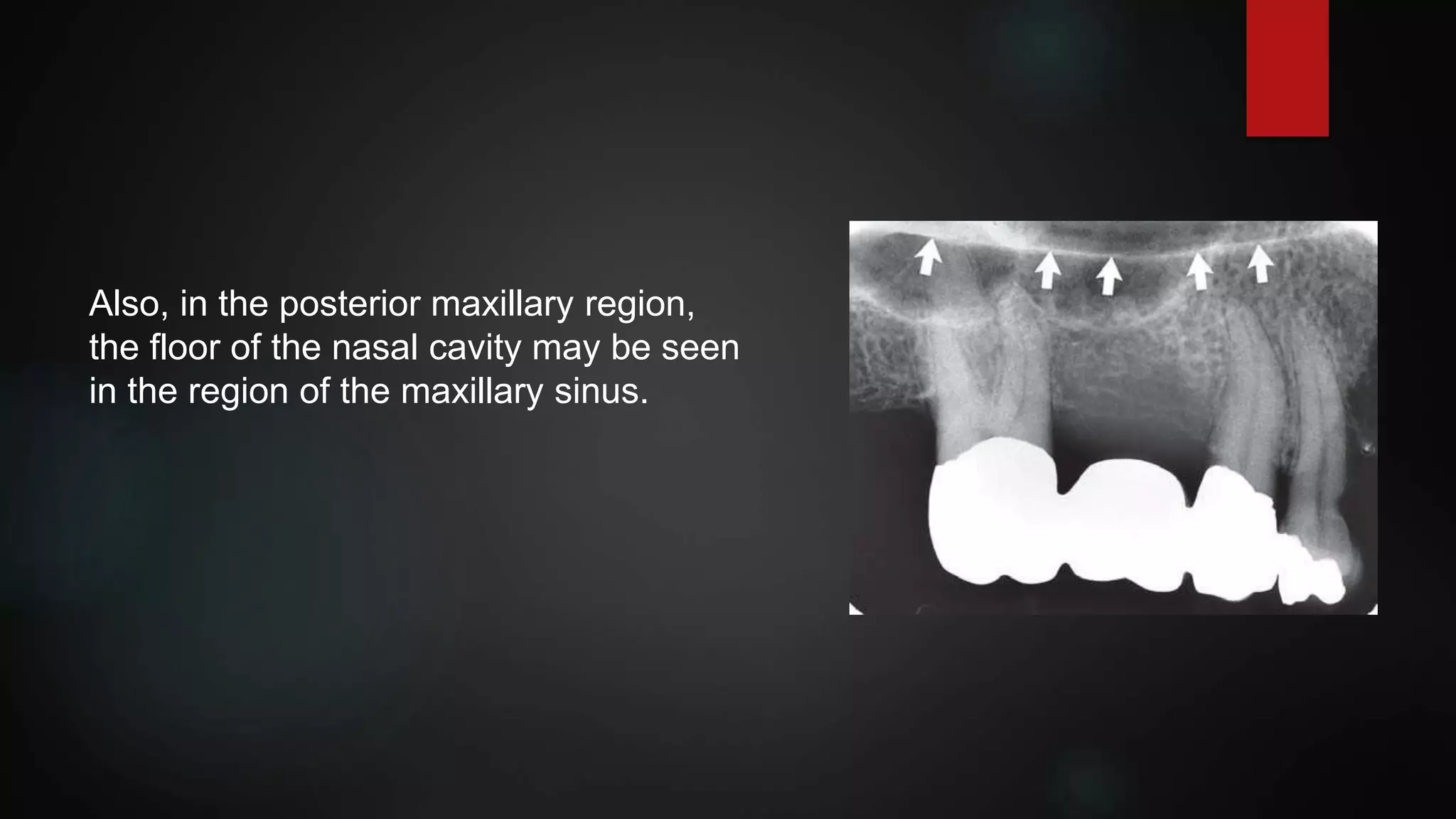
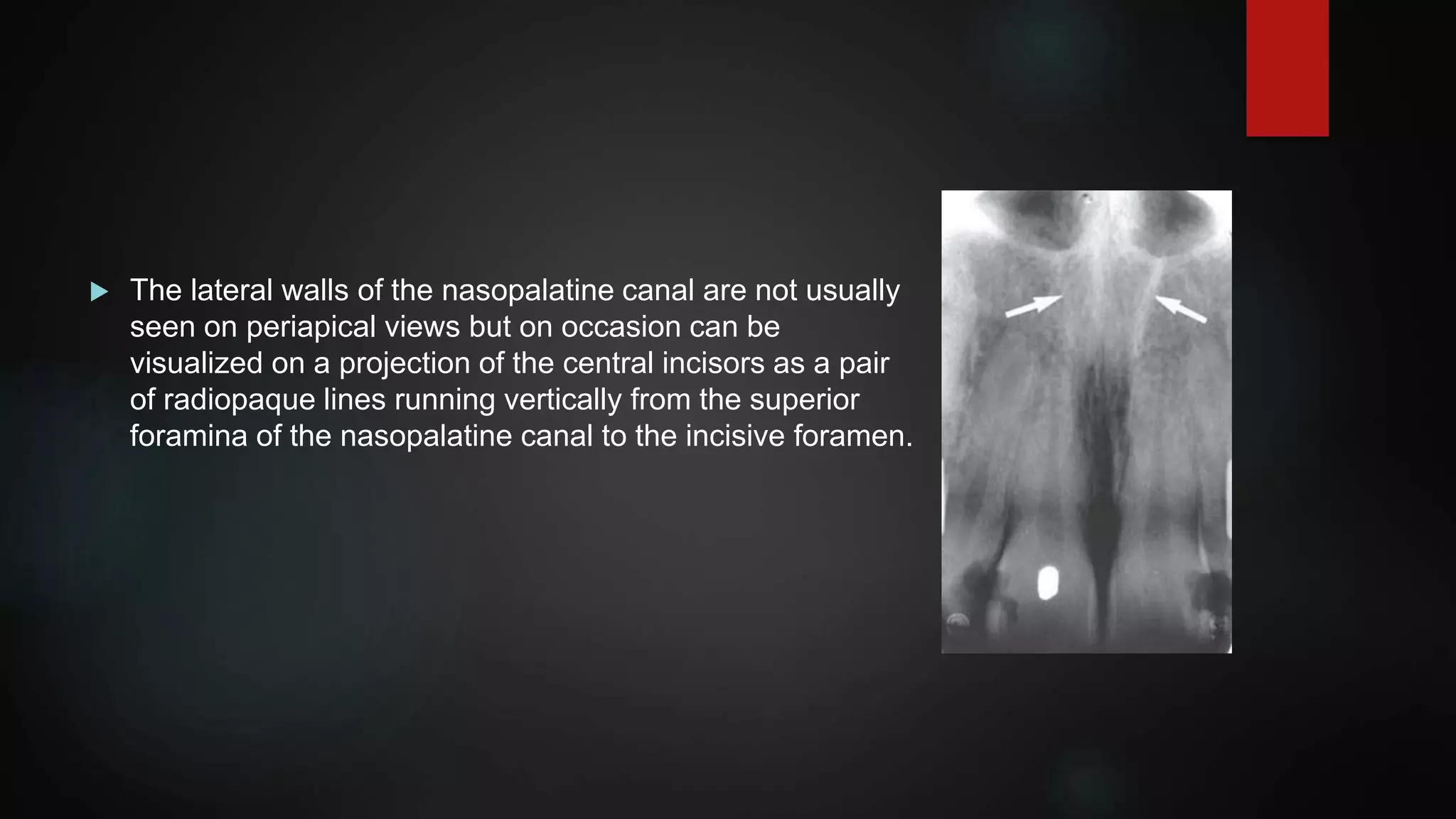
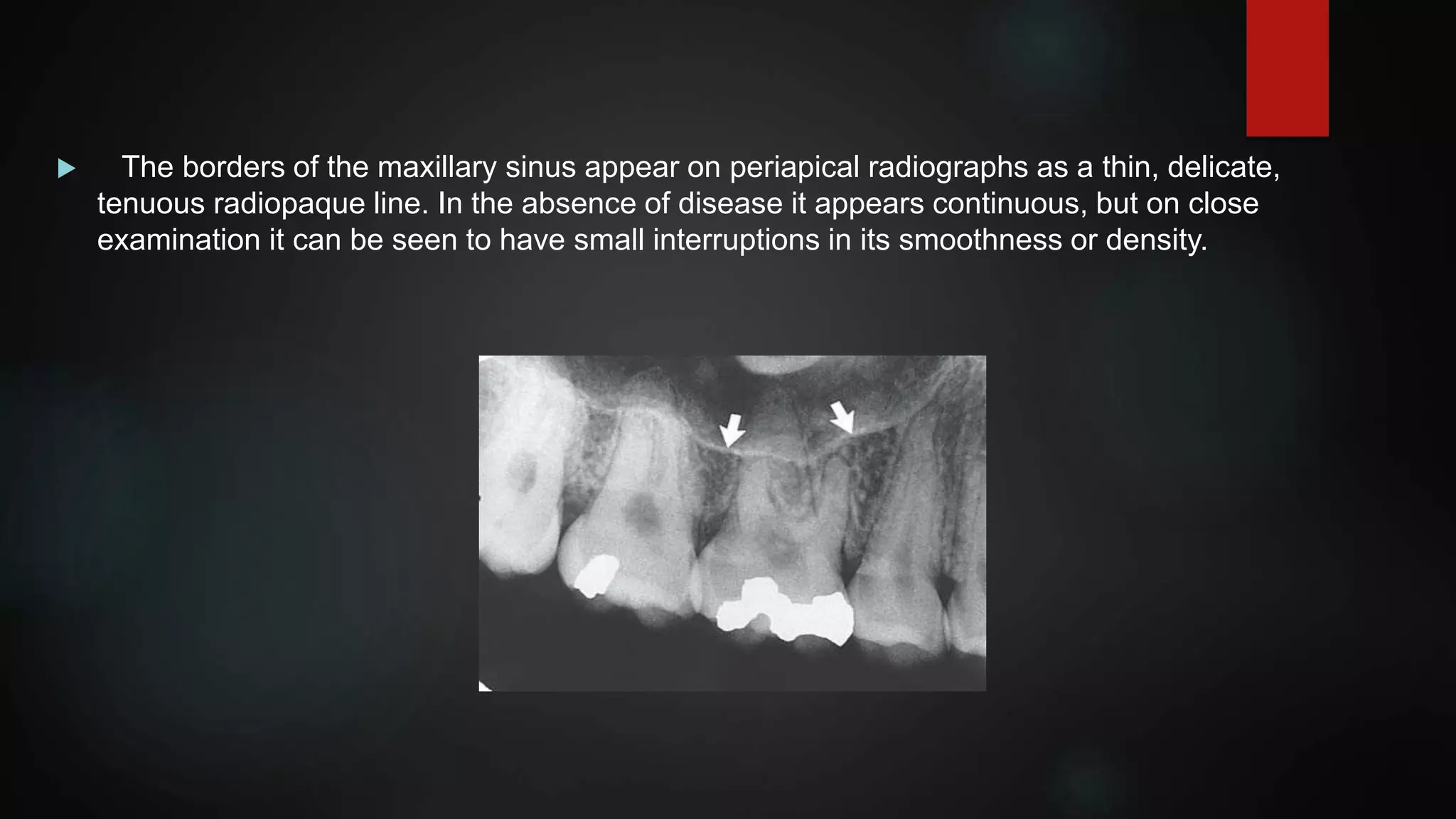
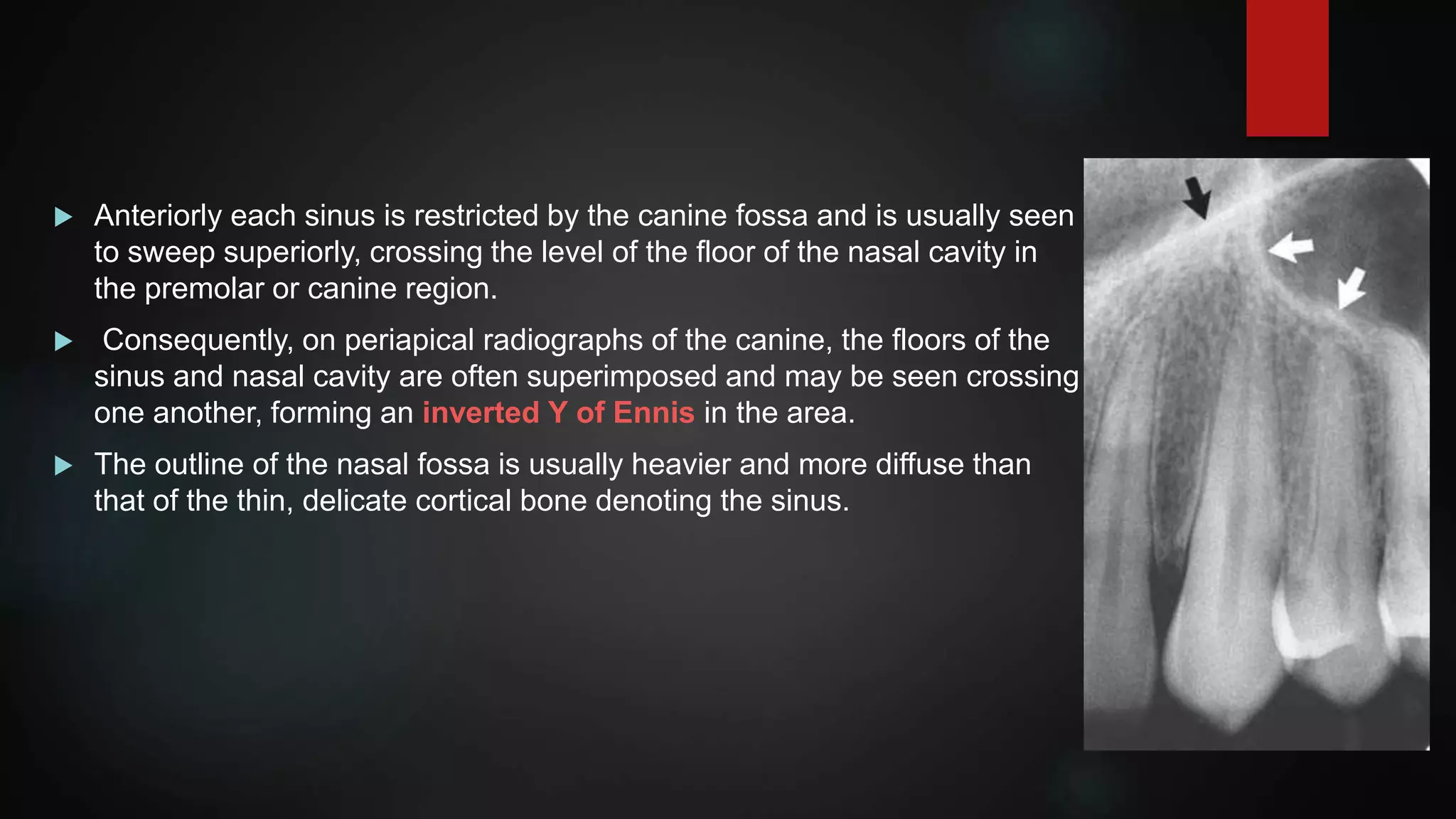
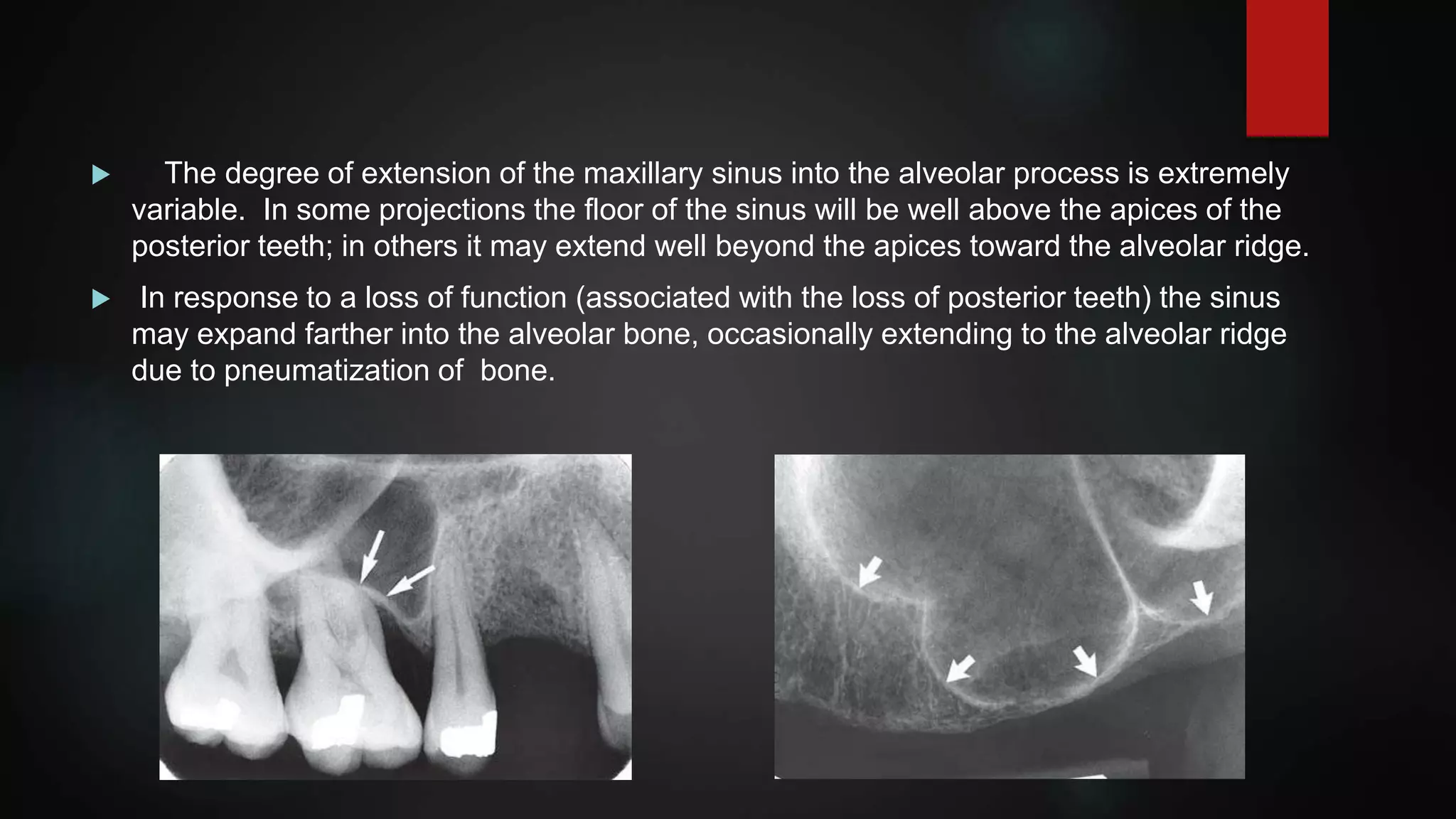
This document provides an overview of normal anatomical structures that can be visualized on intraoral periapical radiographs. It describes the radiographic appearance of teeth, supporting structures like the lamina dura and periodontal ligament space, and cancellous bone. It also outlines specific structures seen in the maxilla, including the intermaxillary suture, anterior nasal spine, nasal aperture, incisive foramen, and lateral walls of the nasopalatine canal. Structures in the mandible like the trabecular pattern are also discussed. The document emphasizes that understanding normal anatomy on radiographs is essential for accurate diagnosis by recognizing variations in anatomy and distinguishing normal features from potential pathology.