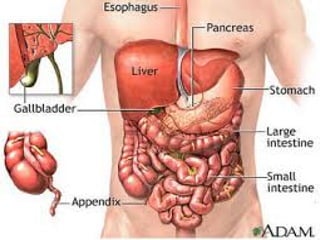
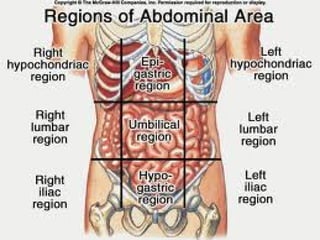
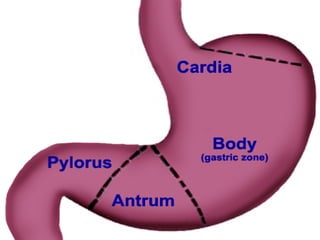
THE ABDOMEN
The abdomenis divided for
descriptieve puposes in to nine
regeions by the intersection of
imaginary planes, two horiczontal
and two sagital .
The upper horizontal plane lies at the
level of the first lumber vertebra ,
midway between the suprasternal
notch and the sysmphysis pubis, the
lower plane passes through the upper
border of the iliac crest.
SYMPTOMS AND SIGNSOF
GASTROINTESTINAL DISEASES
Some important symptoms are:
Abdominal pain
Nausea and vomiting
Heart burn
Altered bowel habits (diarrhea,
constipation)
Abdominal distension
Bleeding
Jaundice
9.
ACUTE GASTRITIS
a)
Definition :inflammationof stomach lining
from irritation of gastric mucosa(normally
protected from gastric acid and enzymes by
mucosa barrier ).
Types
Acute Gastritis
1) Disruptin of mucosa barrier allowing
hydrochloric acid an pepsin to have contact
with gastric tissue leads to irritation,
inflammation, superficial erosion.
2) Gastric mucosa rapidly regenerates self
limited disorder.
10.
Causes of acutegastritis
a)Irritants include aspirin and other
NSAIDS corticosteriods, alcohol
and caffeine .
b)Ingestion of corrosive substance:
alkali or acid .
C) Effects from radiation therapy ,
certain chemotherapeutic agents .
11.
Manifestations
A) Mild: anoxia,mild epigastric
discomfort , belching .
B) More severe : abdominal pain ,
nausea vomiting .
C) Erosive : not associated with
pain bleeding occurs two or
more days post stress events .
12.
Chronic gastritis
Progressive disorderbeginning with
superficial inflammation and leads to
atrophy of gastric tissue .
It has two types
1) Autoimmune Gastritis (Type A
Gastritis)
This is characterized by the involvement
of fundus and body of the stomach.
Circulating autoantibodies are found
against parietal cells and intrinsic factor.
This type of gastritis is generally
asymptomatic.
14.
2) Helicobacter PyloriGastritis (Type B
Gastritis)
its more common and occurs with the aging
caused by chronic infection of mucosa by
H.pylori associated with risk of peptic
ulcer disease and gastric cancer .
Diagnosis test
a. Gastric analysis :asses hydrochloric acid
secretion
b.Hemoglobin ,hematocrit ,red blood cell
indices :anemia including iron deficiency.
Uncommon Types ofGastritis
Other types of gastritis are
granulomatous gastritis
(tuberculosis,sarcoidosis,
candidiasis, syphilis, Crohn’s
disease),eosinophilic gastritis
and lymphocytic gastritis.
18.
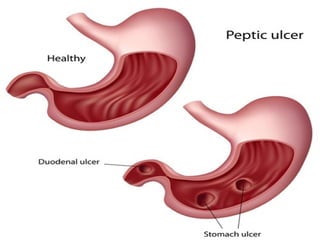
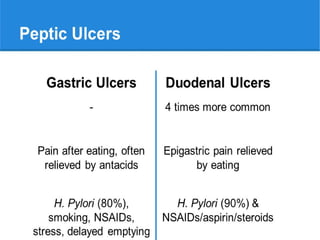
Peptic ulcer
Definition
Breaks inmucus lining of GI tract when it
comes in to contact with gastric juice .
Sites of ulcer formation
a. Duodenal ulcers : most common
affect mostly males ages 30-55 ulcer
found near the pyloris.
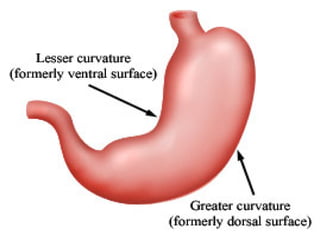
b. Gastric ulcers: affect older persons
ages 55-70 found on the lesser
curvature and associated with
increased incidence of gastric cancer .
22.
Risk factors ofpeptic ulcer
Smokers
Users of NSAIDS
Blood group O
Alcohol
Cigarettes
Diagnosis of pepticulcer
Endoscopy with ulcer
looking for H.pylori
TREATMENT
Antiacids eg:malox syrup
H2-receptor blockers : ranitidine and
famotine
Proton –pump inhibitors : Omeprazole for 8
weeks or 3 to 6 months .
WHAT IS THEDIFFERENCE
BETWEEN GASTRITIS AND
PUPTIC ULCER ?
27.
Gastric carcinoma
There aretwo types of gastric carcinoma
1.Intestinal –type adenocarcinoma
It arises from gastric mucous cells that
have undergone intestinal metaplasia
due to chronic gastritis .
Chronic gastritis may be caused by
H.pylori or it maybe autoimmune
associated with perniciuos anemia .
It occurs primarily after ago 50yrs .
Risk factors
1.
2.
A. Intestinal–type adenocarcinoma
Chronic gastritis
Nitrite
B. Diffuse carcinoma
1.Risk factors unknown
2.Slight increased associated with blood
group A.
3.Infection with H.pulori
Clinical features
Early gastriccarcinoma is a
symptomatic .
Advanced gastric carcinoma :
Abdominal discomfort
weight loss
Dysphagia
Gastric outlet obstruction
Case Scenario
When youare in the borama general
hospital you meet patient that
complain anoxia, mild epigastric
discomfort , belching ,
abdominal pain , nausea ,
vomiting what is the diagnosis
of this case ?
35.
DIARRHEA
Diarrhea are increasedstool mass
frequency or fluidity .
DYSENTRY
Low volume ,painful bloody diarrhea
are known dysentery.
Acute diarrhea
1.
2.
Acute diarrheais caused mainly by
infections (90%). It may also be
caused by drugs, ischemia, toxins
and other conditions.
CAUSES
Infectious
Non-infectious
38.
Clinical Manifestations
Fever.
Abdominal pain.
Bloody diarrhea (dysentery).
Inflammatory type such as sheigellosis,
salmonellosis, E. coli.
Watery non-bloody diarrhea with nausea,
vomiting and abdominal bloating .
39.
Dysentery
Dysentery is definedas diarrhea
due to acute inflammation of the
large intestine characterized by the
presence of blood and mucus in the
stool.
Two types of dysentery
1. Bacillary dysentery
2. Amoebic dysentery
40.
Causes
Important causes ofbacillary
dysentery are :
1.sheigella.
2.E. coli .
Amoebic dysentery is caused
by
1.E. histolytica.
41.
Clinical features ofdysentery
Diarrhea.
Fever.
Abdominal pain.
Tenesmus .
Stools are usually small and contain
blood .
The colon is tender to palpate.
Diagnosis depends on stool
examination and culture.
Food poising
Food poisoningis
gastroenteritis of infective or
non-infective origin.
The important infective
causes are S. Aureus ,
salmonella, and E. coli.
Non-infective causes are
allergy to sea foods, fish or
fungal toxins.
45.
Sign and symptomof food poising
Nausea
Vomiting
Watery diarrhea
Abdominal pain and cramps
Fever
46.
Treatment of foodpoisoning `
Replacement of lost fluids. Fluids and
electrolytes — minerals such as sodium,
potassium and calcium that maintain the
balance of fluids in the body.
Antibiotics. Food poisoning caused by
listeria needs to be treated with
intravenous antibiotics .
During pregnancy, prompt antibiotic
treatment may help keep the infection
from affecting the baby.
Complication
The most commonserious
complication of food poisoning is
dehydration .
Infants, older adults and people
with suppressed immune systems
or chronic illnesses may become
severely dehydrated when they
lose more fluids than they can
replace.
49.
Case
A 22years oldwoman comes to
you in your dental practice. She
has multiple symptoms which
are Diarrhea, Fever, abdominal
pain,tenesmus,Stools are usually
small and contain blood or
purulent material, The colon is
tender to palpate.
What is the diagnosis ?
50.
Malabsorption
Disorders of digestionand diminished
absorption of dietary nutrients (one or more)
are referred as malabsorption syndromes.
Various diseases with varied etiologies can
lead to malabsorption and may present with
different clinical manifestations.
Normal digestion and absorption may be
divided into three phases and malabsorption
can result from abnormalities in one or more of
these phases
51.
Phases of malabsorption
1.Intraluminal Phase
There is inadequate hydrolysis and
solubilization of dietary nutrients
(protein, fat and carbohydrates) leading
to malabsorption. This is mainly due to
insufficient bile or pancreatic enzymes.
The important causes are pancreatic
diseases, biliary obstruction, cholestatic
liver diseases and decreased
enterohepatic circulation of bile salts.
52.
Cont..
2.Mucosal Phase
The damageto the intestinal epithelium or
resection of a part of small intestine diminishes
the surface area for absorption. The brush
border enzyme defects may also lead to
malabsorption.
3. Absorptive Phase
Lymphatic obstruction prevents proper uptake
and transport of absorbed lipoproteins and
chylomicrons. Increased pressure in lymphatics
may cause leakage of absorbed nutrients back
into the intestinal lumen leading to steatorrhea
and protein loosing enteropathy.
53.
Causes of malabsorption
Biliaryblockage .
Bowel resection .
Cancers, such as lymphoma or pancreatic
cancer .
Celiac disease .
Certain medications, including tetracycline,
diet drugs, and some antacids
Crohn’s disease
Food intolerances
Liver disease .
Parasite infections
Whipple disease
Haemorrhoids (piles)
Hemorrhoids alsocalled piles,
are swollen and inflamed veins in
anus and lower rectum.
Hemorrhoids may result from
straining during bowel
movements or from the increased
pressure on these veins during
pregnancy, among other causes.
58.
Causes of hemorrhoids
Theveins around anus tend to stretch under
pressure and may swell. Swollen veins
(hemorrhoids) can develop from an increase in
pressure in the lower rectum. Factors that might
cause increased pressure include:
Straining during bowel movements
Sitting for long periods of time on the toilet
Chronic diarrhea or constipation
Obesity
Pregnancy
Low-fiber diet
59.
Sign and symptom
Painlessbleeding during bowel
movements
Itching or irritation in anal
region.
Pain or discomfort.
Swelling around anus.
A lump near anus, which may
be sensitive or painful.
Leakage of feces.
60.
Examination
In early casesno abnormality out
side the anal verge .
In late cases prolapsing piles can be
seen .
COMPLICATION
1.Profuse bleeding and anemia
2.Thrombosis
3.Ulceration
61.
Management
•
•
Primary haemorrhoids
First andsecond degree conservative
treatment.
Third and fourth degree is
recommended .
For secondary haemorrhoids
treatment is direct to the cause.
Early cases high fiber deit,small doses
of laxatives and avoidance of staining




















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




