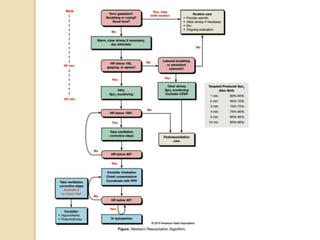
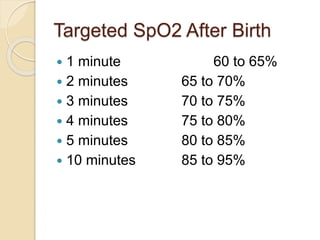
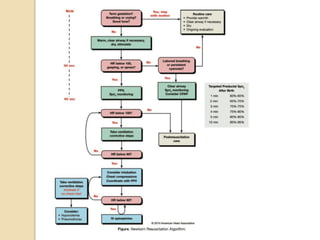
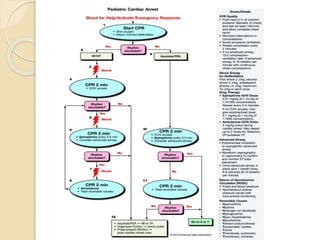
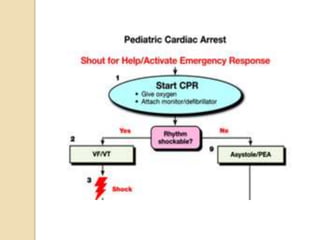
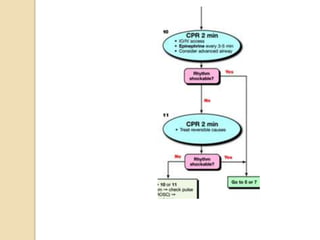
This document provides guidelines for neonatal and pediatric resuscitation. It covers BLS for infants and children, neonatal resuscitation, and pediatric advanced life support (PALS). Key points include procedures for assessing responsiveness and providing breaths or chest compressions. It also outlines the initial steps and interventions for neonatal resuscitation, including warming, clearing airways, and assessing heart rate and breathing. Target oxygen saturation levels are provided. The document also discusses resuscitation for meconium exposure, apnea, prematurity, and PALS techniques like high-quality CPR, defibrillation doses, drug therapies, and reversible cardiac arrest causes.