





![Additional tests
First trimester screening (10–13 weeks of gestation),
which includes serum screening for pregnancy-associated
plasma protein A (PPA) and beta-hCG, and an ultrasound
assessment of nuchal transparency.
Second trimester screening (15–20 weeks of gestation)
consisting of triple (maternal serum α-fetal protein
[MSAFP], estriol, and hCG) or quadruple (“quad”)
(MSAFP, hCG, estriol, and inhibin) screening tests.
Ultrasound examination for neural tube defects, in the
second trimester](https://image.slidesharecdn.com/1-introductiontoobstetrics-120929011207-phpapp02/75/1-Introduction-to-obstetrics-15-2048.jpg)






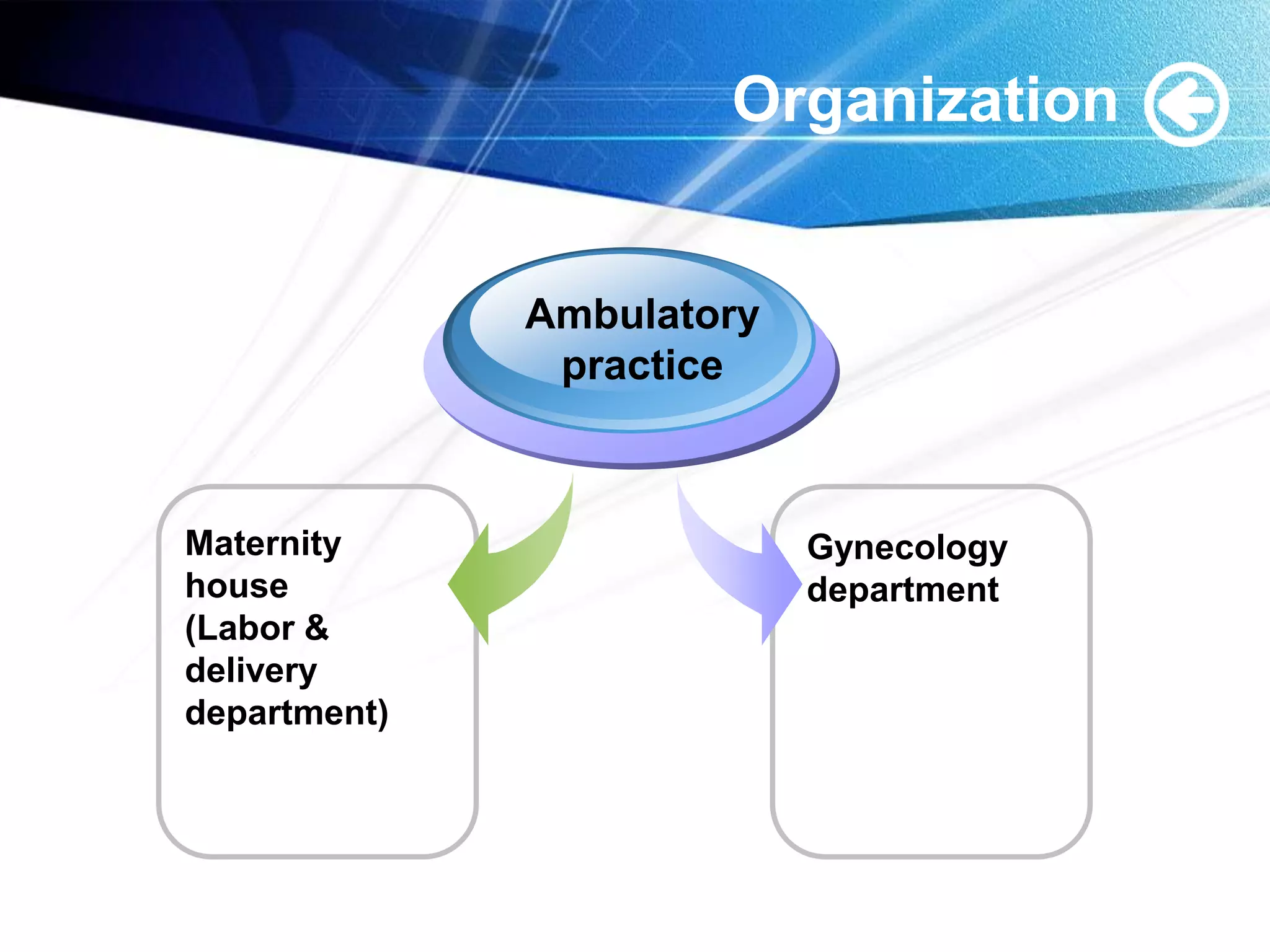
The document provides an overview of obstetrics and gynecology (OB/GYN) including: 1. OB/GYN deals with surgical care of the female reproductive system, including care for pregnant and non-pregnant patients. 2. There are several OB/GYN subspecialties focused on areas like high-risk pregnancies, infertility, cancers, and pelvic issues. 3. OB/GYN care is organized through ambulatory practices, maternity houses, gynecology departments, and various levels of hospitals.























































































