
Recommended
More Related Content
What's hot
What's hot (20)
Similar to 1. a case study on dcm with severe pah
Similar to 1. a case study on dcm with severe pah (20)
More from Dr. Ajita Sadhukhan
More from Dr. Ajita Sadhukhan (17)
Recently uploaded
Recently uploaded (20)
1. a case study on dcm with severe pah
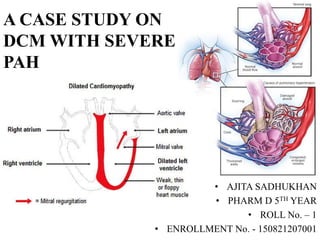
- 1. A CASE STUDY ON DCM WITH SEVERE PAH • AJITA SADHUKHAN • PHARM D 5TH YEAR • ROLL No. – 1 • ENROLLMENT No. - 150821207001
- 2. SUBJECTIVE EVIDENCE: Patient OPD No. 19126109 Patient IPD No. 19016981 Department Male Medicine Ward Unit II Age 45 years Gender Male Date of Admission 28.06.19 Date of Discharge 03.07.19 26-03-2020 2
- 3. Reason for admission : C/O: - cough with expectorant - dyspnoea × 2 months - oedema of feet × 15-20 days Past Medical History: NAD Past Medication History: NAD Family History: NAD Social History: Ex- smoker Previous Allergies: NKA 26-03-2020 3 Bowel + Bladder habits: Regular Sleep: Adequate S/O: - Cardiomegaly with pericardial haziness Physical Examination: - T/P/R: normal/118 bpm/normal - B.P.: 110/70 mm Hg - RS: BLAE crepts +
- 4. Complete Blood Count (28.06.19) LABORATORY PARAMETERS OBSERVED VALUE NORMAL RANGE UNIT Hb 13.5 12.5-16 g/dL WBC 6580 4000-10500 /mcgL Neutrophils 70 50-70 % Eosinophils 3 0-7 % Lymphocytes 24 20-40 % Monocytes 03 <10 % Basophils 0 <1 % RBC 6.23 4.20-5.40 Millions/mcgL MCH 21.7 27-31 pg Platelets 2.52 1.5-4.5*10^5 /mcgL MCV 67 78-100 fL Hematocrit (PCV) 41.7 37-47 % MCHC 32.4 32-36 g/dL RDW-CV 15 11-14.6 % 26-03-2020 4
- 5. • 28.06.19 1. ECG: - Extreme tachycardia - Poor R wave progression - Inverted T wave - Excessive overload of atria • 29.06.19 1. Renal function test: a. S. Creatinine: 1.1 mg/dL (0.5-1.5 mg/dL) 2. Serum Electrolytes: a. Se. Na+: 128 mmol/L (135-145) b. Se. K+: 4.2 mmol/L (3.5-5) c. Se. Cl-: 95 mmol/L (98-107) 3. 2D Echo: Carotid Doppler Test: - Dilated LV with global hypokinesia with poor systolic function - Dilated cardiomyopathy with poor systolic function with severe PAH • 30.06.19 1. Lipid Profile: a. Se. Cholesterol: 114 mg/dL (<200) b. Se. Triglyceride: 71 mg/dL (<150) c. Se. HDL Cholesterol Direct: 41 mg/dL (<40) d. Se. LDL Direct: 58.8 mg/dL (<100) e. Se. VLDL: 14.2 mg/dL (7.0-35) f. Cholesterol : HDL: 2.7805 (0-4.9) g. Se. LDL : HDL : Cholesterol: 1.4341 (upto 3.5) 2. TSH (3rd gen.): 1.221 uIU/mL (0.3- 5.6) 26-03-2020 5
- 6. ASSESSMENT • Provisional Diagnosis: Dilated cardiomyopathy with severe PAH • Justification: • A 45 year old male patient was admitted to male medicine ward unit 2 with complaints of cough with expectorant, dyspnoea since 2 months and oedema of feet since 15-20 days. • Based on subjective evidence, ECG and 2D Echo, the patient was diagnosed with dilated cardiomyopathy with severe PAH .26-03-2020 6 Final Diagnosis: Dilated cardiomyopathy with severe PAH
- 7. GOALS OF TREATMENT • Dilated cardiomyopathy: The primary goal is to improve cardiac function and reduce the symptoms, lifestyle modifications that decrease symptoms and hospitalizations and improve the quality of life. • Pulmonary arterial hypertension: The goals of the treatment are to alleviate the symptoms, improve the quality of life, slow the progression of the disease and improve survival. A general goal of PAH treatment is to correct the balance between vasoconstriction and vasodilation and prevent adverse thrombotic events to improve oxygenation and quality of life. 26-03-2020 7
- 8. 2. PAH:TREATMENT OPTIONS 1. DCM: • Treatment of dilated cardiomyopathy is essentially the same as treatment of chronic heart failure (CHF) i.e., blood pressure control. ACE Inhibitors, ARBs, Beta Blockers, Aldosterone Antagonists, Cardiac Glycosides, Diuretics and Antiarrhythmics.
- 9. Day 2: 29.06.19 • Temp.: normal • Pulse: 74 bpm • BP: 120/80 mm Hg • SPO2: 98% 26-03-2020 9 Day 1: 28.06.19 • GC: stable • Temp.: normal • Pulse: 110 bpm • BP: 130/80 mm Hg • SPO2: 98% Day 3: 30.06.19 • GC: stable • Temp.: normal • Pulse: 86 bpm • BP: 130/78 mm Hg • SPO2: 98% • Adv.: SRD, cardio. Ref. today, Se. lipid profile pending, 2D Echo Day 6: 03.07.19 • GC: stable • Temp.: normal • Pulse: 96 bpm • BP: 100/60 mm Hg • SPO2: 96% • Adv.: CST, SRD, plan discharge Day 5: 02.07.19 • GC: stable • Temp.: normal • Pulse: 93 bpm • BP: 100/60 mm Hg • SPO2: 96% • Adv.: SRD Day 4: 01.07.19 • GC: stable • Temp.: normal • Pulse: 80bpm • BP: 118/76 mm Hg • SPO2: 99% • Adv.: Cardio. ref., collect report of lipid profile and TSH, SRD • Cardio. Ref.: C/O DCM/ Severe LVD, severe PAH • P/W: CCF→ now stabilized, plan medical management • Adv.: Tab. Ramipril 1.25 mg HS • Rest as per Rx chart • Follow up in OPD after 15 days
- 10. Day-wise Medication Chart 26-03-2020 10 DRUG DOSE ROUTE FREQU ENCY INDICATIONS D A Y 1 D A Y 2 D A Y 3 D A Y 4 D A Y 5 D A Y 6 Inj. Furosemide 10 mg (½ amp.) I.V. B.D. Pedal oedema √ Tab. Aspirin +Atorvastatin (75+10) mg P.O. 0-0-1 Prevention of heart attack and stroke √ √ √ √ √ √ Tab. Pantoprazole 40 mg P.O. 1-0-1 Prevention of gastric disturbances √ √ √ √ √ √ Tab. Carvedilol 3.125 mg P.O. ½-0-½ PAH and DCM √ √ √ √ √ Tab. Spironolactone + Torsemide (50+10) mg P.O. 1-1-0 Pedal oedema √ √ √ √ √ Tab. Ramipril 2.5 mg P.O. 0-0-½ PAH and DCM √ √ √
- 11. Discharge Medication Chart 26-03-2020 11 Adv.: (i) Take the above medications for 7 days (ii) Follow-up in OPD on Thursday DRUG DOSE ROUTE FREQUENCY INDICATIONS Tab. Methylcobalamin, alpha lipoic acid,benfotiamine, biotin, inositol, taurine, pyridoxine, Vit. E - P.O. 1-0-1 Nutritional vitamin and mineral supplement for healthy functioning of nerves and body Tab. Aspirin +Atorvastatin (75+10) mg P.O. 0-0-1 Prevention of heart attack and stroke Tab. Pantoprazole 40 mg P.O. 1-0-1 Prevention of gastric disturbances Tab. Carvedilol 3.125 mg P.O. ½-0-½ PAH and DCM Tab. Spironolactone + Torsemide (50+10) mg P.O. 1-1-0 Pedal oedema Tab. Ramipril 2.5 mg P.O. 0-0-½ PAH and DCM
- 12. GOALS ACHIEVED • No fresh complaints. • General condition of patient was stabilized. • Blood pressure was controlled. • Patient felt better. 26-03-2020 12
- 13. MONITORING PARAMETERS ❑ Disease related : 1. DCM: ECG, Exercise tests (treadmill test), Holter monitoring, echocardiogram, MRI, Electrophysiology study, Coronary angiography, myocardial perfusion scan, transoesophageal echocardiogram. 2. PAH: ECG, pulmonary wedge pressure ❑ Drugs related : 1. Furosemide → B.P., Se. Electrolytes, Se. Creatinine and BUN, BT and CT, LFT, RFT. 2. Aspirin + Atorvastatin → ECG, ESR, CRP + Lipid profile, LFT 3. Pantoprazole → Endoscopy, Urea Breath test, Se. Mg 2+, Se. Vit. B12 4. Carvedilol → B.P., ECG, symptomatic 5. Spironolactone + Torsemide → B.P., UOP, RFT, Se. Electrolytes, uric acid, blood glucose 6. Ramipril → B.P., ECG, Se. K+, RFT, WBC 26-03-2020 13
- 14. POINTS TO BE INTERVENED WITH THE DOCTOR Drug-Drug Interactions: – Aspirin + Ramipril → Moderate: may result in decreased effectiveness of ramipril. – Aspirin + Carvedilol → Moderate: May result in increased blood pressure. 26-03-2020 14
- 15. PATIENT COUNSELLING: 26-03-2020 15 ABOUT DISEASE: 1. Dilated cardiomyopathy (DCM) is a condition in which the heart's ability to pump blood is decreased because the heart's main pumping chamber, the left ventricle, is enlarged and weakened. In some cases, it prevents the heart from relaxing and filling with blood as it should. 2. Pulmonary arterial hypertension (PAH)is a type of high blood pressure that affects arteries in the lungs and in the heart. It is characterized by a progressive and sustained increase in the pulmonary vascular resistance that eventually may lead to right ventricular failure. It can be a life-threatening condition if untreated.
- 16. 26-03-2020 16 ABOUT DRUGS: •Aspirin + Atorvastatin: Take one tablet daily at night after dinner at the same time with a glass full of water. Stop taking the drug in case of any unusual or excessive bleeding, GI ulceration, rhabdomyolysis or myopathy. Side effects may include dyspepsia, agitation, confusion, dizziness, headache, lethargy, Reye’s syndrome, seizures, diarrhoea, UTIs, extreme pain, nasopharyngitis and arthralgias. Avoid excessive quantities of alcohol or grapefruit juice. • Pantoprazole: Take one tablet each at least 30 mins before meal once at morning and the other at night. Stop the drug in case of cutaneous or SLE. Side effects may include osteoporosis related fractures (on long term use), abdominal pain, nausea, vomiting, diarrhoea, flatulence, dizziness, headache, fever, rash and arthralgia. • Carvedilol: Take ½ tablets once in morning and another at night with food. Don’t discontinue the drug suddenly. Immediately report to your physician in case of hypotension, arrythmias, syncope, palpitations, angina or edema. Side effects may include diarrhoea, nausea, vomiting, arthralgia, dizziness, back pain, myalgia, headache, vision disorder, erectile dysfunction, reduced libido or fatigue. • Spironolactone + Torsemide: Take the tablet consistently before or after meal once in the morning and another at afternoon. Consult the physician in case of gynaecomastia, dehydration, hypotension, ototoxicity, light-headedness, syncope or symptoms of worsening renal function. Side effects include diarrhoea, nausea, vomiting, abdominal cramping, fever, leg cramps, lethargy, mental confusion, decreased libido, excessive urination and rash. Avoid the use of non-prescription NSAIDs. • Ramipril: Take ½ tablet everyday at night with or without food. Avoid activities requiring mental alertness or coordination. Stop taking the drug in case of angioedema, unusual bleeding or infections, Side effects may include dizziness, nausea, vomiting, persistent cough and fatigue. Arise slowly from a sitting or lying position. Maintain adequate hydration. Avoid potassium supplements. •Dibnerve: Take 2 tablets a day after meal once in morning and another at night.
- 17. LIFESTYLE MODIFICATIONS: i. DCM: a) Salt restriction, no excessive activities, bedrest. b) Eat Healthy. Eating a variety of fruits, vegetables, and whole grains and choosing lean meats and fish can help improve the patient’s heart health. ii. PAH: a) Immunizations against influenza and pneumococcal diseases should be provided. b) Hypoxemia may aggravate vasoconstriction in such patients, therefore they may require supplemental oxygen, particularly when using air travel. c) Patients should adhere to a low-sodium diet to avoid fluid retention predisposing to right heart failure. d) Cardiopulmonary rehabilitation improves functional status and is safe and important for patients with PAH. 26-03-2020 17
- 20. REFERENCES : • A textbook of Pharmacotherapy : By Joseph P. Dipiro and Robert L. Talbert, 7th Edition, Mc- Graw Hill Publications • Medscape • Cims • Micromedex • Mayoclinic.com
- 21. 26-03-2020 21