Medicine: Critical Care,18
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
CRITICAL CARE IN MEDICINE
Cardiopulmonary resuscitation
- Basic Life Support (BLS) - Advance Cardiovascular Life Support (ACLS)
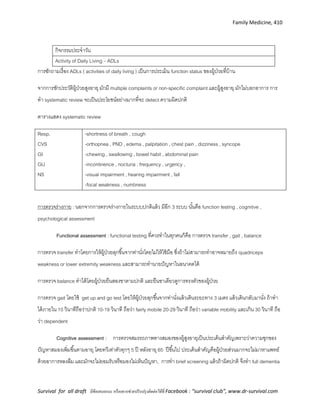
BLS for Adult, Children, and Infants
Component Adult Children Infants
Recognition Unresponsive, No breathing or only gasping, No pulse in 10 S
CPR sequence C-A-B A-B-C (เว้นเด็กโรคหัวใจ)
Rate At least 100/min
Depth 2 นิ้ว ( 5 cm ) ½ of AP diameter 1.5 นิ้ว (4cm)
Ratio 30 : 2
(ไม่ว่ากี่คนก็ตาม)
30 : 2 (single rescuer)
15 : 2 ( 2 rescuer)
การเลือกท่อช่วยหายใจ
19.
Medicine: Critical Care,19
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
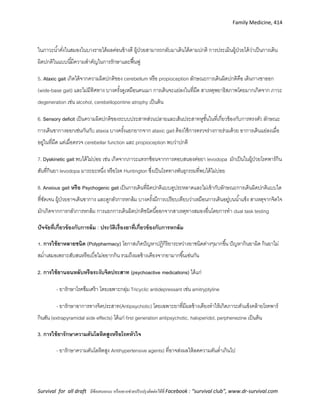
Cardiac arrest
แก้ไข reversible cause
Hypovolemic
Hypoxia
Hydrogen ion
Hypo/Hyper K
Hypothermia
Tension pneumothorax
Temponade, cardiac
Toxin
Thrombosis, pulmonary
Thrombosis, coronary
Adrenaline 1
mg IV q 3-5
min
Unshock able
(Asystole/PEA
)
+ Amiodarone 300
mg
Start
CPR
Shock able
(VF/VT)
CPR 2
min
CPR 2
min
+ Amiodarone 150
mg
CPR
ROSC
Adrenaline 1
mg IV q 3-5
min
Dose เด็ก
RLS หรือ NSS 20 cc/kg ใน 20 นาที
Adrenaline 0.01 mg/kg(dilute 1 amp
เป็น 10 cc แล้วให้0.1 cc/kg)
NaHCO3 1-2 mEq/kg/dose Z µ
20.
Medicine: Critical Care,20
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
ข้อเปลี่ยนแปลงของ BLS ใน Guidelines 2010 รายละเอียด + สาเหตุ
1. เริ่ม CPR ด้วย C-A-B แทน A-B-C
ยกเว้นใน Infant ที่สาเหตุหลักยังเกิดจาก
asphyxia มากกว่า
ให้ทาการกดหน้าอก 30 ครั้งก่อนช่วยหายใจ
จะทาให้เพิ่มการกดหน้าอก ช่วยชีวิตได้เร็วกว่า
2. Recognition ยกเลิกตาดูหูฟัง ,ใช้การมองว่าหมดสติ/หยุดหายใจ/หายใจเฮือก
บุคลากรคลา pulse ถ้าลังเลมากกว่า 10 วินาทีให้ถือว่าไม่มี
3. Good Quality CPR
- Push hard, Push fast
- No hyperventilation
- Less interuption
- กดลึกอย่างน้อย 2 นิ้วในผู้ใหญ่และ 1 นิ้วในเด็กเล็ก
- กดเร็วกว่า 100 ครั้ง/ min, และให้มี Fully recoiled
- No tube = 30:2, with tube = 6-8 sec/ครั้ง
- หยุดเฉพาะคลาชีพจร/ช็อกไฟฟ้ า/advance airway ต้อง<10 S
4. Used AED ให้ใช้ได้ในทุกคน(ของเก่าไม่ให้ใช้ในเด็ก) ถ้าเป็นเด็กควรมี pediatric
dose แต่ถ้าไม่มีอนุโลมให้ใช้เท่าผู้ใหญ่ได้
5. ไม่ใช้ Atropine เว้นแต่สาเหตุของ PEA / Asystole นั้นเกิดจาก vagal effect
6. เพิ่มการใช้ Quantitative waveform
capnography
Keep ET-CO2 > 10 mmHg, If > 4o mmHg = ROSC
7. เพิ่ม Post- cardiac arrest Care - Keep O2 sat> 94% (no excessive Oxygenation)
- Therapeutic Hypothermia if indicate(ข้อห้ามคือมี bleeding)
- CAG if indicate
8. Neonatal resuscitation ให้เริ่ม PPV ด้วย room air และ monitor O2 satที่แขนขวาเพื่อปรับความ
เข้มข้นของ Oxygen
21.
Medicine: Critical Care,21
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Arrhythmia
แบ่งได้เป็น 1. Tachycardia : HR > 100/min 2. Bradycardia : HR < 60/min
ขั้นแรกต้องประเมิน stability ของคนไข้ ได้แก่
- Hypotension
- Acute altered mental status
- Sign of shock (hypoperfusion)
- Ischemic chest discomfort
- Acute congestive heart failure
Bradycardia Tachycardia
- Oxygen mask with bag 10 LPM / On ET-Tube
- NSS 1,000 ml IV
- LAB investigation + cardiac enzyme/TFT
- EKG 12 lead, EKG monitoring
If unstable
- Atropine 1 amp (0.6 mg) IV then repeat q 3-5 min (MAX 3
mg) ,Then
- Transcutaneous pacing (rate 80 – 100, Amplitude 70 – 100
ขึ้นอยู่กับ EKG ว่า trigger ไหม)
- หรือ Dopamine (1:1) IV 15 - 60 ml/hr
หรือ Adrenaline (1:10) IV 3 – 20 ml/hr
If stable just monitoring
- Oxygen mask with bag 10 LPM / On ET-Tube
- NSS 1,000 ml IV
- LAB investigation + cardiac enzyme
- EKG 12 lead, EKG monitoring
If unstable ดู EKG
- SVT : Adenosine 6mg -> 12 mg ->cardioversion 50 -100 J
(adenosine ออกฤทธิ์ภายใน6S ดังนั้นถ้าให้แล้วไม่ดีหรือที่รพ.ไม่มี
อาจพิจารณา cardioversion ต่อเลย )
- Irregular narrow QRS : cardioversion 120-200 J
- Wide QRS (VT) : Defibrillation 100 J
If stable ดู EKG
- Narrow QRS
SVT -> vagal maneuver -> Adenosine 6mg IV double
syringe technique - 5 min -> Adenosine 12 mg -> IV
verapamil or IV diltiazem or IV beta-blocker -
>cardioversion 50 -100 J
Medicine: Critical Care,23
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Common drug doses in emergency conditions
Cardiopulmonary resuscitation
Pulseless arrest
Adrenaline 1 mg (1amp) iv q 3-5 mins
Amiodarone 300 mg + 5%DW 20 ml iv push in 5 m then 150 mg iv + 5%DW 20 ml iv push in 5 m
MgSO4 1 gm (1amp) + 5%DW 10 ml iv push
Tachyarrhythymia
Adenosine 6 mg iv push (Double syringes technique), then 12 mg iv push then 12 mg iv push
Amiodarone
150 mg + 5%DW 20 ml iv push in 10 mins, if VT recurs Follow by maintainace
infusion 1 mg/min iv drip in first 6 hrs, then 0.5 mg/min iv drip in next 18 hrs
Total Max dose 2.2 gm/day, practical ให้: 900 mg + 5% DW 1000 ml iv drip in 24 hrs
Digoxin 0.25 - 0.5 mg iv push
Bradyarrhythmia
Atropine 0.6 mg (1amp) iv push q 3-5 mins, Maximun 3 mg (5amp)
Dopamine 2-10 mcg/kg/min, practical (Pt.50kg) : (2:1) iv drip 3-15 mcd/min
Adrenaline 2-10 mcg/min, practical (Pt.50kg) (12:1000) iv drip 10-50 mcd/min
6H5T
Hypovolumia Isotonic – NSS RLS Acetar, Colloid – Dextran Voluven
Hypoxia ET-Tube
24.
Medicine: Critical Care,24
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Hydrogen(acidosis) 7.5% NaHCO3 1-2 amp iv push
Hypokalemia Elixir KCL 30 cc Oral q 3-4 hr
Hyperkalemia
10%CalciumGluconate 10 ml iv push + 50%Glucose 50 ml + RI 10 u iv push
7.5% NaHCO3 1 amp iv push + Kayexalate – Kalimate – Ventolin NB
Hypothermia Keep Warm – Bair Hugger therapy
Hypoglycemia 50% Glucose 50-100 ml iv push
Tension
Pneumothorax
ICD
Cardiac tamponade Pericardiocentesis
Toxins Antidote
Thrombosis (MI PE) …
Shock and initial management before admission
Cardiogenic shock
Dobutamine 2-20 mcg/kg/min, practical (Pt.50kg) : (2:1) 3-30 mcd/min
Septic shock
Dopamine
เตรียม 1:1 (mg:ml),
2:1,4:1 in NSS or
5%DW
practical (Pt.50kg) : (2:1) 3-30 mcd/min dose 2-20 mcg/kg/min
1-5 µg/kg/min: reduce SVR through dopamine receptor
5-10 µg/kg/min: +inotropic & chronotropic effect through β1 adrenergic receptor
10-20 µg/kg/min: increase SVR through α1 adrenergic receptor
25.
Medicine: Critical Care,25
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Norephineprine
4:500, 4:250, 8:250
(mg:ml) in 5%DW
1-40 mcg/min, practical (Pt.50kg) : (1:25) 2-60 mcd/min
Adrenaline
1:10 (mg:ml) in
NSS or 5%DW
0.05-1 µg/kg/min
Anaphylactic shock
Adrenaline 0.5 mg (1/2 amp) im stat
Dexamethasone 8 mg iv stat then 4 mg iv q 6 hrs
CPM 10 mg (1amp) iv stat
Ranitidine 50 mg (1amp) iv stat
Adrenal shock
Hydrocortisone 200 mg iv stat then 100 mg iv q 8 hrs(or 300 mg drip in 24hr)
Respiratory failure
Sedative drug
Valium 10 mg iv stat
Dormicum 5 mg iv stat
26.
Medicine: Critical Care,26
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Post resuscitation care
1 Optimizing physiology
- Body temp. therapeutic hypothermia , keep mild hypothermia (32-340
c)by external cooling device or cold
air for 24 hr then rewarming to >35o
c in 8 hr(ระวัง arrhythmia, coagulopathy)
- Blood pressure keep MAP<65 mmHg ,urine output 0.5-1 ml/kg/hr, SBP> 120 mmHg is preferred
- Glycemic control close monitor BS 80-110 mg/dl
- Acid-base-electrolyte avoid severe acidosis, hyper/hypo kalemia, hypomagnesemia, Keep O2 sat > 94% (
no excessive Oxygenation )
2.Revascularization in coronary disease PCI /Thrombolysis/CABG ขึ้นกับ condition ของผู้ป่วย
3. Anti-arrhythmic therapy ควรใช้ B-blocker ทุกรายถ้าไม่มีข้อห้าม หากมี arrhythmia รุนแรง เช่น recurrent VT
พิจารณาใช้ amiodarone หรือ implantable cardioverter defibrillator (ICD)
4.Anticonvulsant therapy ภาวะชัก พบได้ 30-40% ยาที่ใช่บ่อยเป็น phenytoin และ thiopental ซึ่งมีฤทธิ์กันชักและเป็น
neuroprotective ,ไม่แนะนา Routine prophylaxis ด้วยยากันชักในทุกราย
Other - หากมีการใช้ therapeutic hypothermia ต้องระวังภาวะ sepsis เนื่องจากอาจบดบังอาการ
- ventilator setting ให้ใช้เป็น normocarbia คือ PaCO2 35-40 mmHg.ไม่แนะนา hyperventilation เพื่อลด ICP
Poor prognosis
1. เมื่อไม่มี corneal reflex ที่ 24 hr
2. ไม่มี papillary reflex ที่ 24 hr
3. ไม่มี withdrawal response to pain ที่ 24 hr
4. ไม่มี motor response ที่ 24 hr
27.
Medicine: Critical Care,27
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
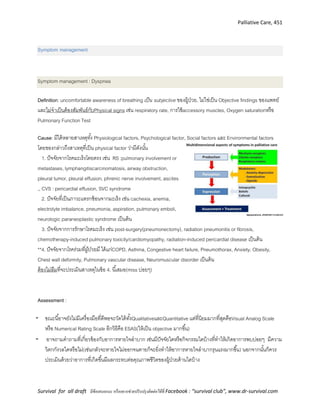
Acute Respiratory Failure
Causes, มี 4 ชนิด Clinical Presentation Investigation
Ventilatory resp. failure
- CNS depression
- Drug overuse
- Neuromuscular
diseases
Perioperative resp. failure
- จากภาวะ atelectasis
Hypoxemic resp. failure
- Respiratory system
- Cardiovascular system
- Upper airway
obstruction
Hypoperfusion state
(shock)
- ซึม, coma, cyanosis
- tachypnea, use of
accessory respiratory
muscles, air hunger, พุด
ไม่จบประโยค,ขาดเป็น
ห้วงๆ, Tachycardia,
Abdominal paradox
- ABG
- CXR
- If pulmonary
edema is
suspected,
consider ECG
and cardiac
enzymes
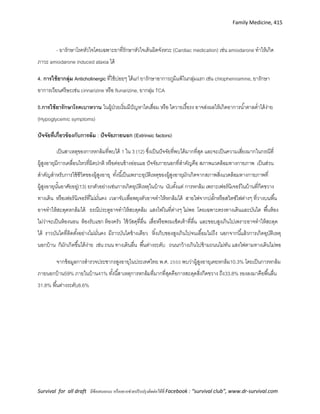
Diagnostic criteria of acute respiratory failure (2/4)
1. Acute dyspnea
2. PaO2 < 50 mmHg
3. PaCO2 > 50 mmHg
4. Significant respiratory acidemia
กลไกการเกิด hypoxemia : 6 ชนิด ได้แก่ Hypoventilation, diffusion defect, shunt, V/Q mismatch, low FiO2, low
mixed venous oxygen ภาวะเหล่านี้ส่วนใหญ่จะมี (A-a) gradient กว้าง แต่ ภาวะ hypoventilation และ low FiO2
จะมี (A-a) gradient ปกติ
Evaluation of hypoxemia : ควรตรวจหาสาเหตุและให้การรักษาอย่างเหมาะสม
ระวัง! เมื่อเจอ air hunger ควรจะคลา carotid pulse คนไข้ เพราะสภาพ air hunger เจอได้ตั้งแต่ก่อน arrest จนถึง
arrest ไปแล้วช่วงหนึ่ง
ในกรณีเร่งด่วน ให้การวินิจฉัยจากลักษณะทางคลินิก เช่น อาการ
หอบเหนื่อยร่วมกับ central cynaosis, ซึมลง เป็นต้น ควรรีบรับไว้
รักษาในโรงพยาบาล
PaCO2 increased
no yes
↑ (A-a) gradient ? Hypoventilation
↑( A-a) gradient ?
no yes
↓ Inspired
PO2
(low FiO2)
Response to
100% O2 ?
noyes
Hypoventilation alone
- ↓ Respiratory drive
- Neuromuscular
Hypoventilation +
another mechanism
ShuntV/Q mismatch
noyes
Medicine: Cardiology, 51
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
condition characteristic location duration
Unstable angina เจ็บแน่นหน้าอก อึดอัด เหมือนมี
อะไรมาทับ เกิดขณะพัก
Retrosternal, often radiation to or isolated
neck, jaw, shoulders, arms frequently on left
มักนาน 20-30 min
Acute MI เหมือนข้างต้นแต่รุนแรงกว่า Same ≥ 30 mins
**ระวังผู้ป่วยที่เป็น DM, geriatricและ female อาจไม่ได้มาด้วย chest pain แต่มา present ด้วย acute heart failure
Management : ACS
1. History and physical examination (อย่าลืมซักประวัติ C/I of fibrinolytic drug)
2. EKG 12 leads
- Unstable angina หรือ NSTEMI : ST depress at least 0.5 mm or dynamic T wave inversion ขณะที่มีchest pain หรืออาจไม่
เปลี่ยนแปลงได้ (ทั้งสองภาวะรักษาไปในทางเดียวกัน)
- STEMI : ST elevation at least 1 mm in lead that present in the same wall at least 2 leads or New LBBB (ในผู้ป่วยที่มา
present ด้วย chest pain ถ้าไม่มีEKGเดิมเทียบ ให้ถือว่าเป็น new LBBB เอาไว้ก่อน) *อย่าลืมทาlead V3R V4R(ติดlead V3
และ V4 ไว้ข้างขวา)เพื่อดูRV infarction (ฝากไว้ให้ช่วยดูใน STEMI ว่า QRS ไม่กว้าง, ใน lead เดียวกัน ควรมี QRS หน้าตา
เดียวกัน และดู reciprocal change ถ้ามีก็ช่วยให้มั่นใจขึ้น)
3. Cardiac enzymes : ที่ ER จะไม่ดู cardiac enzyme เนื่องจากใน 4-6 ชม.แรก
sensitivityต่า
4. Initial management “ M O N A” ระยะแรกรักษาเหมือนกันทั้ง STEMI, NSTEMI และ UA
-Oxygen therapy : จาเป็นต้องให้ใน 6 ชม.แรก keep oxygen sat ≥ 90 %
-Aspirin : 160 – 325 mg เคี้ยว (ถ้ากินไม่ได้ให้ 300 mg rectal supp.)
- ISDN (5) 1 tab sublingual prn for chest pain ช่วยลด pain แต่ไม่ลด mortality rate (ยามีผลลดBP ห้ามให้ใน
ผู้ป่วย BP drop โดยเฉพาะที่มี RV infarction ร่วมด้วย) ) ให้ผู้ป่วยอมได้มากที่สุด 3 ครั้ง หากยังไม่หายอาจพิจารณา
ให้ NTG IV drip หากไม่มีข้อห้าม - systolic BP < 90 mmHg หรือต่าลงกว่าของเดิมเกิน 30 mmHg, HR < 50 หรือ
> 100 bpm, หรือสงสัย RV infarction
-Morphine :2-4 mg IV dilute repeat q 5-15 min. ให้ในกรณีที่ใช้ NTG แล้วไม่ทุเลา ไม่ควรใช้ในกรณีที่สงสัย RV
infarction
5. Specific treatment แยกตาม UA, NSTEMI และ STEMI จะกล่าวต่อไป
V7 - posterior axillary line
V8 - tip of scapula
V9 - paraspinal border
ทั้งสามติดในระดับ 5th Lt.ICS
52.
Medicine: Cardiology, 52
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
EKG in ACS : STEMI
การอ่าน EKG STEMI in clinical practice คือ
Pitfall ที่ 1 ใน Pericarditis ST elevate ได้แต่จะยกแบบ Diffuseและยกใน wall เดียวกัน มีหน้าตาต่างกันได้และไม่มี
reciprocal
Pitfall ที่ 2 การจะอ่าน ST ยกหรือไม่นั้น ต้องอยู่บนฐานของ Narrow QRS complex เพราะถ้า Wide QRS จะอ่านได้
ยาก หรืออ่านไม่ได้ เช่น LBBB จะมี wide QRS ST ยกได้ โดยไม่ใช่ STEMI
Pitfall ที่ 3 กรณีที่เกิด prinzmetal angina ST จะยกได้ แต่เป็นการยกที่ไม่ใช่ของจริง พวกนี้อาจมาด้วย Chest painซึงมัก
เป็นตอนอากาศเย็นๆ เพราะจะกระตุ้นให้เกิด vasospasm ของ coronary artery ได้ หลังจากอมยาใต้ลิ้นแล้ว อาการจะดีขึ้น
พอทา EKG หลังจากอาการดีขึ้นแล้วจะพบว่า ST elevation หายไป ตรวจสอบให้สิ่งสายพาน ST ที่ยกจะหายไปได้โดยไม่ต้อง
ทาอะไรเลย
Pitfall ที่ 4 กรณีที่เป็น Early repolarization ST จะยกได้ แต่ยกแบบท้องช้าง pattern คือ มี notch แล้วยกแบบ
downslope จะพบได้สูงสุดใน mid precordial ( V 3 – 4) แต่ยก
สูงไม่เกิน 3 ช่อง พวกนี้จับวิ่งสายพานแล้วจะหายหมดเลย
Pitfall ที่ 5 กรณี ST ยกเฉพาะที่ V 5 -6 แล้วเรามอง Anterior
MI แต่ทา Echo แล้ว พบว่า Anterior ปกติ ให้ลองกลับ EKG จะกลายเป็น Posterior MI ได้
Pitfall ที่ 6 ST ยก และ QRS กว้าง เป็น Hyper K เช่น on ยา ACEI และไตไม่ดี
Pitfall ที่ 7 Bugada จะพบ RBBB ST Elevate ใน V 1 – 3 ได้
53.
Medicine: Cardiology, 53
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Pitfall ที่ 8 ST ยก โดยมี QRS กว้าง และเล็ก ให้คิดถึง AF with WPW พวกนี้defib ก่อน แล้วจะทาให้ rate ช้าลง แล้วจึงจะ
เห็น delta ได้ชัดเจน (เพราะเป็น WPW rate จะเร็ว)
Pitfall ที่ 9 ST elevation ที่เป็นอยู่เดิม คือเทียบกับ EKG ของเดิม แล้วไม่เปลี่ยนแปลง อาจเกิดจาก aneurysm ของผู้ป่วยอยู่
เดิมได้
STEMI
specific treatment : keep door to needle time < 30 mins and door to balloon time < 120 mins
STEMI onset
< 3 hrs 3-12 hrs >12 hrs
Fibrinolytic(efficacyเท่ากับทาPCI) Cardiogenic shock or ongoing chest pain
Streptokinase 1.5 mu IV drip in 1 hr No
(หรือ rt-PA,tenecteplase ตามที่รพ.มี) Yes
ขณะให้เผ้าระวัง hypotension, bleeding
C/I ของการให้ fibrinolytic drug
Absolute C/I Relative C/I
1.hx of ICH
2.hx of brain tumor or AVM
3.hx of ischemic stroke in 3 months
4.สงสัย aortic dissection
5.bleeding tendency
6.hx of head trauma in 3 months
1.hypertension (SBP≥180,DBP≥110)
2.prolonged CPR
3.hx of internal bleeding in 2-4 wk
4.pregnancy
5.cogulopathy
6.previous Streptokinase use
ให้ LMWH 8 days or until D/C
- Fondaparinoux 2.5 mg SC OD
- Enoxaparin 0.6 ml SC BID
(ปรับdoseตาม age และ CrCl)
PCI
54.
Medicine: Cardiology, 54
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
LMWH dose
6. Adjunctive therapy : “S A A B” ให้เหมือนกันทั้ง STEMI, NSTEMI และ UA
- statin : simvastatin (20) 1 tab OD keep LDL-c < 100 mg/dl
- antiplatelets : ASA (300) 1 tab OD then 75-162 mg OD lifelong
Clopidrodrel (300,75 mg.) 300 mg. stat then 75 mg. OD 1 year
ไม่ว่าจะเป็น Bare metal or DES
ถ้าให้ thrombolytic ให้นาน อย่างน้อย 14 วัน หรือ 1 ปีถ้าเป็นไปได้
UA/NSTEMI ( ไม่ได้ทา PCI) ให้นาน อย่างน้อย 1 เดือน หรือ 1 ปีถ้าเป็นไปได้
or Ticargrelor (90mg) 180 stat then 90mg bid
or Prasugrel (10,60 mg) 60 mg. stat then 10 mg. od (ใช้เฉพาะ case ที่จะทา CAG/PCI)
- ACEI : enalapril (5) 1 tab BID
- Beta blokers : ให้ได้ทุกตัวในไทย (ห้ามให้ใน CHF, bradycardia, hypotension )
age standard dose Severe renal impairment (CrCl < 30 )
<75 Enoxa. 0.3ml IV bolus + 0.6ml SC then 0.6ml SC BID
Fondaparinux 2.5 mg sc od
0.3ml IV bolus + 0.6 ml SC then 0.6ml SC OD
Avoid Fondaparinux
≥ 75 EoxaparinNo bolus dose. ให้ 0.4ml SC BID
Fondaparinux 2.5 mg. sc od
No bolus dose. ให้ 0.6 SC OD
Avoid Fondaparinux
ลด recurrence
ลด mortality
ลด recurrence
55.
Medicine: Cardiology, 55
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
NSTEMI and Unstable angina
clopidogrel 300 mg (4 tab) stat then 75 mg/day, LMWH : ให้ 3-8 days
CAG +/- PCI : พิจารณาทาภายใน 12-24 ชม.เฉพาะกลุ่ม high risk
- Recurrent angina/ischemia at rest or low level activities - Troponin-T positive
ทั้งๆที่ได้ intensive medical treatment - LVEF < 40%
- Refractory angina/ischemia - Hemodynamic instability
- Previous PCI within 6 months - Sustain VT
- Previous CABG - New ST depression
- ผล Exercise stress test เป็น high risk - New congestive heart failure
- High TIMI risk score (TIMI risk score ≥ 3 ช้อ) - New/ worsing mitral regurgitation
Acute pulmonary embolism (APE)
ภาวะลิ่มเลือดอุดตันในหลอดเลือดแดงในปอดชนิดเฉียบพลัน เป็นภาวะฉุกเฉินที่ให้การวินิจฉัยได้ยาก เนื่องจากมี
อาการและอาการแสดงไม่จาเพาะ จาเป็นต้องได้รับการรักษาอย่างรีบด่วน
เพราะมีผลต่อการเกิดภาวะแทรกซ้อนและอัตราการรอดชีวิตของผู้ป่วย
ภาวะนี้มีผลต่อทั้งระบบไหลเวียนเลือดและระบบการหายใจ ผลต่อระบบ
ไหลเวียนเลือดมักเกิดขึ้นเมื่อ มีการอุดตันของ pulmonary arterial bed
มากกว่าร้อยละ 30-50 เพิ่ม pulmonary vascular resistance
TIMI risk score
1. Age > 65 yrs.
2. CAD risk factor ≥ 3 ข้อ (HT or on HT drug ,
DM , HDL < 40 ,Fx Hx of premature CAD –
male less than 55 female less than 65 ,
smoking <ไม่รวม age>)
3. Prior CAG พบมี coronary a.
stenosis ≥ 50 %
4. ASA use in last 7 days
5. chest pain > 2 times in last 24 hr
6. ST deviation ≥ 0.5 mm
7.elevated cardiac enzyme
56.
Medicine: Cardiology, 56
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
เพิ่ม pul.arterial pressure เพิ่ม RV afterload RV dilate + dysfunction RV failure Cardiogenic shock
ผลต่อระบบหายใจ Hypoxemia V/Q mismatch mixed venous oxygen ต่า +/- pul. Infarction
Clinical presentation ผู้ป่วย APE จะมาด้วยอาการและอาการแสดงได้หลากหลาย ตั้งแต่ไม่มีอาการจนถึงเสียชีวิต
อาการที่พบบ่อยได้แก่ เหนื่อยหอบ เจ็บหน้าอก ไอเป็นเลือด หน้ามืด หมดสติ ความดันโลหิตต่า
Initial evaluation เนื่องจากเป็นกลุ่มอาการที่ไม่จาเพาะจึงมีการจัดทาแนวทางการประเมินเบื้องต้น เพื่อเป็นแนวทางในการ
management อย่างรวดเร็ว โดยเราต้องประเมิน 2 ประเด็นหลักคือ Pretest probability และ Severity
a. การประเมิน Pretest probability ที่ยอมรับกันคือ Wells score และ revised Geneva score
b. การประเมิน Severity ของ APE แบ่งตามลักษณะทาง
clinic ดังนี้
I. High-risk PE/ Massive PE(MPE) (short-term mortality.15%). คือ
ผู้ป่วยที่มีความดันโลหิตต่าหรือช็อกที่มีสาเหตุจาก APE จาเป็นต้อง
ได้รับการวินิจฉัยและรักษาอย่างรีบด่วน
II. Non-high-risk PE แบ่งเป็น
a. Intermediate-risk PE (short-term mortality.3-15%).
คือผู้ป่วยที่มี ลักษณะอย่างใดอย่างหนึ่ง ของ RV dysfn
57.
Medicine: Cardiology, 57
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
หรือ myocardial injury แต่ไม่มี hypotension or shock
b. Low-risk PE (short-term mortality.<1%). คือผู้ป่วยที่ไม่มีลักษณะ ของ RV dysfn
หรือ myocardial injury
Diagnostic management algorithm
58.
Medicine: Cardiology, 58
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Investigation
Investigation Finding comment
CXR Westermark’s sign (focal oligemia)
Hampton hump (Low sen/spec)
มีประโยชน์ช่วยแยกโรคอื่นและแปลผล
ร่วมกับ V/Q scan
d-Dimer +เมื่อ > 500 ng/ml Sen >95% low spec
Troponin –T/I แยก MI ,severity of PE
EKG Sinus tac, T-wave inv,S1Q3T3 ,RBBB,RAD Non-specific
Compression U/S and CTV of leg DVT Sen>90% , Spec= 95%
V/Q scan 1 Normal/low probability นึกถึง APE น้อย
2 Intermidiate prob. 3 High prob
ต้องแปลผลร่วมกับ clinical
probability score
CT chest Positive or Negative APE -ต้องแปลผลร่วมกับ clinical
probability score
-MDCT ดีกว่า SDCT
Pulmonary angiography เป็น gold standard ในการวินิจฉัย APE แต่ invasive และ
มี complication มาก จึงมักใช้ MDCT chest มากกว่า
Ecocardiography เป็นประโยชน์มากในผู้ป่วย high-risk PE จะช่วยแยกภาวะอื่น
เช่น cardiogenic shock,aortic dissection เป็นต้น
หากไม่พบ RV overload /Dysfn
ไม่น่าจะช็อกจาก APE
59.
Medicine: Cardiology, 59
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
อย่าลืม !!!!
-CAB ก่อนเสมอ
-O2therapy
- IV access
- consult specialist
- Refer ถ้าอยู่ รพช
Treatment
-CT angiography of chest or pul.angiography
to confirm diagnosis
-Continuous therapy
No
UHF or LMWH or fondaparinux
Yes
- UHF( keep aPTT ratio 2-3)
- IV fluid resuscitation
- Inotropic drug
immediate echocardiography
High RV pressure with shock/hypotension High RV pressure with stabilized BP
- Thrombolytic if no C/I
- Refer for pul.thrombectomy if C/I
CT angiography of chest or pul.angiography
to confirm diagnosis
Suspected APE
Hypotension/shock ?
Hypotension/shock
Continuous therapy
- Consult specialist
- หาสาเหตุของ thrombosis
- bridging ด้วย warfarin
keep INR 2-3 จนกว่าจะแก้เ
cause of thrombosis ได้
- ส่งปรึกษา ผู้เชี่ยวชาญพิจารณา
IVC filter หากมีข้อห้าม ต่อ
warfarin หรือมี recurrent
thrombosis
60.
Medicine: Cardiology, 60
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Acute aortic dissection
Acute aortic dissection แบ่งเป็น
1. Proximal type (Sanford type A)
คือมี dissection ที่ ascending aorta
2. Distal type (Sanford type B)
คือมี dissection ที่ descending aorta
History Symptom and sign Investigation
Predisposing factor
Proximal type : ผู้ป่วยอายุน้อยหรือวัย
กลางคน มี medial degenerative
disease Marfan syn,Ehlers-danlos
syn. CNT dis
Distal type : HT ,atherosclerosis
Other : S/P aortic Sx , chest trauma
Proximal type : severe sharp-
shooting chest pain , Distal type :
severe back pain
esp.interscapular area
Signs : ขึ้นอยู่กับบริเวณที่เกิด dissection
อาจทาให้เกิด hypovolemic shock,
Ao Obs.,Ao.regur, cardiac
temponade , coronary a.
dissection , stroke ,
paraplegia(dissect. Intercostal a.)
anuria
Bowel ischemia
CXR : enlarge aortic
knob,mediastinum calcified
double contour of aorta
Lt.pleural effusion
CT/MRI chest : true and false
aortic lumen
TEE : septum,false lumen
thickening aortic wall,
Ao. Regur, compression of
lt.atrium, pleural/pericardial
effusion
61.
Medicine: Cardiology, 61
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Managements
C-A-B ตาม ACLS
IV access, foley’cath, lab pre-op
IV B-blocker , vasodilator ( keep SBP 100-120 mmHg , HR 50-60 bpms)
o SNP 0.25-10 mcg/kg/min
o NTG 5-100 mcg/min ปรับ 5 mg/hr q 15 min
o Nicardipine 5-15 mg/hr ปรับ 5 mg/hr q 15 min
o Labetalol initial 20 mg iv over 2 min q 10 min then 40-80 mg iv q 10 min or 1-2
mg /min continuous iv infusion
ข้อบ่งชี้การผ่าตัด
- Proximal type เป็น emergency condition ต้อง consult CVT ผ่าตัดรีบด่วน
- Distal type surgery vs medication ให้ผลใกล้เคียงกัน ต้อง consult CVT พิจารนาก่อน
Acute Heart failure
History Physical exam Investigation
dyspnea (~NYHA class 2-4)
leg edema, orthopnea,
paroxysmal nocturnal dyspnea
อย่าลิมซักเพิ่มเพื่อหา cause of HF
(มีรายละเอียดกรอบข้างล่างต่อไป)
Pitting edema, increase JVP,
hepatomegaly, lung : fine
crepitation, displacement of PMI,
S3 gallop at apex
PE for cause of HF
-pulse irregular?
- heart sound : distant? Murmur?
Lab : CBC, BUN, Cr, electrolyte
CXR : cardiomegaly, pulmonary
edema, pleural effusion
EKG: ใช้ในการหาcause ของ HF
BNP และ NT-pro BNP ใช้แยกกับ
pneumonia โดยใน HF BNP>400,
NP-pro BNP >2000
Cause of Heart failure and approach
Medicine: Cardiology, 67
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Common EKG in cardiac arrhythmia
ในที่นี้จะแสดงให้เห็นตัวอย่างและวิธีสังเกตในเบื้องต้น ส่วนการรักษาและการให้ยา ให้ศึกษาจาก AHA guide line for CPR ในส่วนของ
cardiac arrhythmia
Normal Sinus Rhythm
•Rhythm – Regular •Rate - (60-100 bpm)
•QRS Duration – Normal •P Wave - Visible before each QRS complex
•P-R Interval - Normal (<5 small Squares. Anything above and this would be 1st degree block)
Sinus Bradycardia
•Rhythm – Regular •Rate - less than 60 beats per minute
•QRS Duration – Normal •P Wave - Visible before each QRS complex
•P-R Interval – Normal •Usually benign and often caused by patients on beta blockers
Rx
Sinus Tachycardia Supraventricular Tachycardia (SVT)
68.
Medicine: Cardiology, 68
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
•Rhythm – Regular
•Rate - More than 100 beats per minute
•P Wave - Visible before each QRS complex
•P-R Interval – Normal
•QRS Duration – Normal
Rx
1.หา cause
2.อาจบรรเทาอาการด้วย B-blocker
•Rhythm – Regular
•Rate - 140-220 beats per minute
•P Wave - Often buried in preceding T wave
•P-R Interval - Depends on site of
supraventricular pacemaker
•QRS Duration - Usually normal
Rx
Ventricular Tachycardia (VT)
•Rhythm – Regular
•Rate - 180-190 Beats per minute
•QRS Duration – Prolonged
•P Wave - Not seen
• Pulseless algorithm must perform !!!!!
Ventricular Fibrillation (VF) Abnormal
•Rhythm – Irregular
•Rate - 300+, disorganised
•QRS Duration - Not recognizable
•P Wave - Not seen
•This patient needs to be defibrillated!!
QUICKLY
Atrial Fibrillation Atrial Flutter
69.
Medicine: Cardiology, 69
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
•Rhythm - Irregularly irregular
•Rate - usually 100-160 beats per minute but
slower if on medication
•QRS Duration - Usually normal
•P Wave - Not distinguishable as the atria are firing
off all over
•P-R Interval - Not measurable
•Rhythm – Regular
•Rate - Around 110 beats per minute
•QRS Duration - Usually normal
•P Wave - Replaced with multiple F (flutter)
waves, usually at a ratio of 2:1 (2F - 1QRS) but
sometimes 3:1
•P Wave rate - 300 beats per minute •P-R
Interval - Not measurable
Premature Ventricular Complexes
•Rhythm – Regular
•Rate – Normal
• 2 odd waveforms are PVC
•QRS Duration – Normal
•P Wave - Ratio 1:1
•P Wave rate - Normal and same as QRS rate•P-R
Interval – Normal
Junctional Rhythms
•Rhythm – Regular
•Rate - 40-60 Beats per minute
•QRS Duration – Normal
•P Wave -Ratio 1:1 if visible. Inverted in lead II
•P Wave rate - Same as QRS rate
•P-R Interval - Variable
1st
Degree AV Block 2nd
Degree Block Type 1 (Wenckebach)
70.
Medicine: Cardiology, 70
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
•Rhythm – Regular
•Rate - Normal
•QRS Duration – Normal
•P Wave - Ratio 1:1
•P Wave rate – Normal
•P-R Interval - Prolonged (>5 small squares)
•Rhythm - Regularly irregular •Rate - Normal
or Slow
•QRS Duration – Normal
•P Wave rate - Normal but faster than QRS rate
•P-R Interval - Progressive lengthening of P-R
interval until a QRS complex is dropped
2nd
Degree Block Type 2
•Rhythm – Regular
•Rate - Normal or Slow
•QRS Duration – Prolonged
•P Wave - Ratio 2:1, 3:1
•P Wave rate - Normal but faster than QRS rate
•P-R Interval - Normal or prolonged but constant
3rd
Degree Block
•Rhythm – Regular
•Rate - Slow
•QRS Duration – Prolonged
•P Wave - Unrelated
•P Wave rate - Normal but faster than QRS rate
•P-R Interval - Variation
•Atrioventricular dissociation
ในที่นี้จะขอเขียนลงรายละเอียดเฉพาะ AF, SVT
71.
Medicine: Cardiology, 71
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Atrial fabrillation
o การแบ่งประเภทเป็นแบบ paroxysmal AF (เป็นๆหายๆ), persistent AF)เป็นต่อเนื่อง > 7วัน( และ permanent AF)เป็น
ต่อเนื่อง > 1 ปี
o การอ่าน rate AF ให้เลือกนับว่าใน 30 ช่องใหญ่มี
QRS กี่ตัว นาจน.ที่นับได้คูณ 10 จะได้ rate คร่าวๆ
o การรักษา
พบครั้งแรก พิจารณาหาสาเหตุ)ครั้งแรกที่เจอ
ตรวจ CBC, TFT, BUN, Cr, +/- LFT
o หัวใจเอง )VHD esp MS,MR, ACS, pericarditis, cardiomyopathy โดยในคนแก่ เจอเพิ่มขึ้น รวม
0.36% ของคนไทยทั่วไป(
o โรคปอด เช่น pneumonia
o โรคไทรอยด์เป็นพิษ
o ความดันโลหิตสูง
o อื่นๆ เช่น สมองขาดเลือด อ้วน pheochromocytoma
เป้ าหมายการรักษา
1. Stabilize hemodynamic status และ control of ventricular rate
2. Prevention of thromboembolic complication
3. Restore and maintain sinus rhythm
Rx ระยะสั้น ดูก่อนว่า มี accessory pathway หรือไม่ มี CHF รึป่าว
มี accessory pathway(WPW syndrome)
o BP drop Sync cardioversion (biphasic 100 j)
o BP ดี amiodarone 150 mg IV ช้าๆ stat
มี CHF
o Amiodarone 150 mg + 5%D/W 100 cc IV in 30 min , then 900 mg in 24 hr (ข้อเสีย BP ต่า
,ปอด-ตับอักเสบ)
o Digoxin 0.5 mg IV stat, then 0.25 mg IV q 6 hr (ข้อเสีย ventricle arrhy.)
ไม่มี CHF
o Diltiazem IV or verapamil
Rx ระยะยาว
Medicine: Cardiology, 75
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
VALVULAR HEART DISEASE
Mitral stenosis
Cause: Mostly Rheumatic heart disease very rarely congenital in origin
Symptoms:
1. Heart failure
2. Palpitation due to atrial fibrillation (AF)
3. Stroke from cardiogenic emboli caused by AF
4. Hemoptysis due to pulmonary hypertension
Physical examination:
1. Peripheral pulse: normal, or irregular from AF
2. Carotid pulse: normal
3. Precordium:
PMI normal
Apical heaving absence
±Parasternal heaving
±Apical diastolic thrill
4. Heart sound:
S1 ดังกว่าปรกติเนื่องจากมีเลือดค้างใน left atrium มาก valve จึงเปิดออกกว้างทาให้ปิดด้วยเสียงดัง
S1 อาจเบากว่าปรกติได้ด้วยในกรณีที่ mitral valve มี calcification อย่างมากทาให้ motion ของ valve
ผิดปรกติไป
S2 can be loud (loud P2) in the presence of pulmonary hypertension.
Opening snap (OS): The calcification of the mitral valve usually extends to include cordae
muscle. The stiff cordaes restrict the mitral valve leaflets from opening freely. The sudden
tensing of the valve leaflets after they have completed their opening excursion causes an
opening snap (สะบัด).
S1
P2A2
S1
OS S3
S2
Opening snap heard in mitral stenosis
76.
Medicine: Cardiology, 76
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Distinguish opening snap from P2 and S3 gallop
Sound Unique feature
P2 Vary according to respiration (physiologic splitting)
OS No respiratory variation
S3 Listen to S3 with bell, then covert the bell to a diaphragm by pressing the bell
tightly against the patient’s chest wall, the S3 sound will disappear.
5. Murmur: Diastolic rumbling murmur at apex (low pitch, listen with bell)
Investigations
EKG : Left atrial enlargement, atrial fibrillation, RVH
CXR : Left atrial enlargement , pulmonary congestion
Refer to cardiologist for echocardiogram
Management :
1. Medical treatment
Decrease preload with diuretics: Furosemide 20 mg oral OD
Slow heart rate to allow more diastolic filling time and relieve left atrial volume load: Beta-
blocker: propanolol 40mg oral bid (Depend on HR; Keep 60-80 bpm at rest)
Rheumatic heart prophylaxis: primary secondary
Level of Prevention Medications
Primary prevention
(streptococcal eradication)
Penicillin V (250)1 tab, oral qid. For 10 days
Secondary Prevention
(prevent recurrence)
Rheumatic fever with no carditis: Penicillin V (250) 1
tab, oral bid. For 5 years
Rheumatic fever with carditis but no residual
valvular disease: Penicillin V (250) 1 tab, oral bid.
For 5 years or till 20 years old whichever is longer.
Rheumatic fever with residual valvular defect:
Penicillin V (250) 1 tab, oral bid. For 10 years or till
40 years old whichever is longer
If AF is presence, provide wafarin (Warfarin 5 mg initial , keep INR 2-3) Because of its
teratogenicity, contraception is necessary for female patients.
2. Surgical treatment indication (Mitral valulotomy, percutaneous or open surgery)
Severe MS
77.
Medicine: Cardiology, 77
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Clues for severe MS
Pulmonary hypertension (loud P2, parasternal heaving in the absence of pulmonic
stenosis)
The longer the diastolic rumbling murmur the more severe the stenosis เนื่องจาก valve
ตีบมากเลือดจึงใช้เวลานานขึ้นในการไหลจาก left atrium มา left ventricle
เสียง A2 และ opening snap ใกล้กัน atrio-ventricular pressure gradient ที่สูงทาให้เกิด
earlier mitral valve opening after aortic valve closure.
Symptomatic
Pulmonary hypertension ไม่ว่าจะมี symptoms หรือไม่
Mitral Regurgitation
Causes:
1. Restricted valve motion: Rheumatic MS and MR, Ischemic heart disease from abnormal regional wall motion
2. Annular dilatation: Dilated cardiomyopathy
3. Excessive motion: mitral valve prolapsed
Symptoms: Heart failure
Physical examinations
1. Peripheral pulse: high amplitude, high BP (end diastolic left ventricular volume is higher than normal resulting in
higher preload and stroke volume)
2. Carotid pulse: normal
3. Precordium:
PMI shift to the left
Apical heaving
±Parasternal heaving
±Apical systolic thrill
4. Heart sound:
S1 soft from restricted valve motion
S2 can be loud (loud P2) in the presence of pulmonary hypertension.
ถ้ามี prolapsed mitral valveจะพบ systolic click (a crescendo murmur at mid to late systolic phase เนื่องจาก
prolapsed จะเป็นมากขึ้นเมื่อ left atrium chamber volume is small)
5. Murmur: systolic murmur at apex radiated to axilla, มีได้หลายแบบขี้นกับความเรื้อรังของโรค
78.
Medicine: Cardiology, 78
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Acute MR: early systolic murmur, เนื่องจาก left atrium ยังยืดขยายได้ไม่มากจึงรับได้แค่ small regurgitated
blood volume เลือดจึงไหลผ่าน valve ในเวลาอันสั้นก็หยุด
Chronic MR: Pansystolic murmur, left atrium is enlarged and has high compliance. Large amount of blood
can regurgitate back along the entire systolic phase.
Investigation
EKG : Left atrial enlargement , left ventricular hypertrophy , atrial fibrillation
CXR : Left atrial enlargement , left ventricular hypertrophy and pulmonary edema
Echocardiography : for diagnosis and severity evaluation
Management
1. Medical treatment: not very effective
If HT ให้ ACEI
If LV dysfunction, HF, มีอาการ ให้ ACEI ±digitalis, diuretic, และผ่าตัด
If AF , Warfarin 5 mg oral initial , keep INR 2-3
Refer to cardiologist
2. Surgical treatment (mitral valve replacement, mitral valve repair)
Indication
Symptomatic : History of functional class changed, heart failure, AF
No symptom
- Left ventricular enlargement ; LV end systolic diameter ≥ 45 mm
- Evidence of pulmonary hypertension
- LVEF<60% regardless of regurgitated degree or symptoms. LVEFจะสูงกว่าปรกติอยู่แล้วใน MR ดังนั้น
ผู้ป่วยที่มี LVEF<60% แปลว่ามี poor left ventricular function แล้ว, จึงสมควรเข้ารับการผ่าตัดเพื่อ prevent
further irreversible deterioration.
ในกรณี LVEF<30% ควรเลือก Mitral valve repair เป็น first choice เพราะดีกว่า valve replacement เนื่องจาก
สามารถคงสภาพ valve anatomy เดิมไว้ได้ ในขณะที่ valve replacement จะ distorts valve anatomy ทาให้
LVEF ลดลงหลัง surgery ได้ , ดังนั้นกรณีผู้ป่วยที่ LVEF<30% ที่ valve พังจน repair ไม่ได้ ควรรักษาแบบ
supportive medical treatment ดีกว่าไปทา surgical valve replacement
Aortic Stenosis
Cause:
1. Calcified aortic stenosis from aging change (age > 60 yr.)
2. Rheumatic heart disease (age < 60 yr.)
79.
Medicine: Cardiology, 79
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
3. Congenital bicuspid aortic valve (age < 60 yr.)
Symptoms: ให้จาว่า “ASD 5,3,2”
1. Angina pectoris: Once angina occur the survival period is 5 years.
2. Syncope: from hypotension, once occur the survival period is 3 years.
3. Diastolic heart failure: concentric left ventricular hypertrophy จาก increase in afterload ทาให้ left
ventricular diastolic filling capacity ลดลง The survival rate once occurred is 2 years.
Physical examination:
1. Peripheral pulse: normal
2. Carotid pulse: slow upstroke (pulsus tardus), low amplitude (pulsus parvus)
3. Precordium:
±PMI shift (LV hypertrophy)
Apical sustained heaving (sustained heaving is indicative of pressure load, nonsustained
heaving is found in volume load)
±Systoic thrill at right upper parasternal border
4. Heart sound:
S1 normal, S2 normal ( if severe can be very soft or absent)
Reverse split S2 is heard in severe AS. ปรกติ A2 มาก่อน P2 และระยะระหว่างทั้งสองจะกว้างขึ้น
ในช่วงหายใจเข้าเนื่องจากการเพิ่มขึ้นของ venous return delays pulmonic valve closure เมื่อ aortic
valve แข็งการเปิดปิดซึ่งช้าลงทาให้ได้ยินเสียง A2 ทีหลัง P2 จะทาให้มีผลต่อระยะ A2-P2 splitting ดัง
ภาพด้านล่าง ซึ่งช่วง inspiration มี splitting แคบลงตรงข้ามกับในสภาวะปรกติ
S1
P2A2
S1S2
P2A2
Inspiration
Expiration
P2 A2
P2 A2
Inspiration
Expiration
NormalAorticstenosis
“Reverse S2 splitting”
5. Murmur:
Systolic ejection murmur at right upper parasternal border radiated to the neck
Gallavardin murmur, heard in severe AS, is a systolic ejection murmur ที่ดังมากจนได้ยินไปถึง
80.
Medicine: Cardiology, 80
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
cardiac apex area ด้วยทาให้คล้าย murmur of MR. ใช้ hand grip maneuverในการแยกโรคได้โดย
ให้ผู้ป่วยออกแรกกามือผู้ตรวจไว้ขณะที่ผู้ตรวจฟังเสียง murmur, การเพิ่ม systemic vascular
resistance ด้วยวิธีดังกล่าวทาให้ mitral valves regurgitate มากขึ้นและก่อ louder MR murmur.
6. Clues for severe AS
LVH
Pulsus parvus et tardus
Late peaking murmur: กรณีที่ valve ตีบมากกว่าเลือดจะไหลผ่าน valve มากพอที่จะก่อ murmur ได้
ต้องรอให้ pressure ใน LV สูงมากกว่าปรกติ ดังนั้นยิ่ง valve ตีบมากก็จะยิ่งได้ยินเสียง murmur late ใน
systolic
Investigation:
EKG : left ventricular hypertrophy with strain
CXR : left ventricular hypertrophy and calcified aortic valve
Echocardiography : for diagnosis and severity evaluation
Management :
1. Medical: Diuretic for heart failure symptom, Digitalis and inotropic drugs should be avoid because
the symptom can worsen, Statins are not longer believed to help prolong valve function.
2. Indication for surgery:
1. Severe AS
2. Symptomatic (ASD 532)
3. LVEF<50%
4. Moderate and severe AS without symptom: When open heart surgery is planned for other
reasons (in order to reduce the risk of undergoing the surgery twice)
Aortic Regurgitation
Cause:
1. Vulvular pathology: Rheumatic heart, IE, syphilis, prolapse (from myxematous change)
2. Root dilatation: Marfan, Ehler-Danlos, Takayasu arteritis
Symptoms:
1. Acute onset: Heart failure, Cardiogenic shock
2. Chronic: Heart failure
Physical examination:
1. Peripheral pulse:
81.
Medicine: Cardiology, 81
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Bounding pulse from wide pulse pressure (pulse pressure> 50% of systolic BP -diastolic BP)
Bifid pulse: pulse with two amplitude peaks resulting from aortic elastic recoil in response to
high stroke volume.
2. Carotid pulse: visible carotid pulse (Corrigan signs)
3. Precordium :
PMI shift from LVH
Non-sustained apical heaving
±Diastolic thrill at left upper parasternal border
4. Heart sound:
S1 soft, เบาเนื่องจาก the regurgitated blood jet ดัน mitral valve ทาให้เปิดปิดลาบากขึ้น
5. Murmur:
Diastolic blowing murmur at left parasternal border (high pitch noise, Listen with diaphragm)
To and fro murmur from relative aortic stenosis as a result of high end diastolic volume.
Through and flow murmur.
Austin-Flint murmur is a diastolic rumbling murmur of MS caused by the pressure exerted on
the mitral valve resulting from the regurgitated systolic blood jet.
6. Peripheral signs:
Corrigan’s sign (visible carotid pulse)
Muller’s sign (vibration of uvular)
De musset’s sign (head bobbing)
Landolfi’s sign (pulsatile pupil)
Water hammer pulse (increase intensity of radial pulse when lifting the arm above the head.)
This is because the radial artery is collapsed when the arm is lifted, therefore the bounding
pulse will be sensed as increase in intensity.
Quinche’s sign (อ่านว่า quing-kae) Visible pulsatile nail bed observed when pressuring the nail
Pistol shot (listen to the femoral atery)
Duroziez (du-ro-si-ae) exert slight pressure over the femoral artery using bell, a bruit can be
heard.
S1 S1S2
82.
Medicine: Cardiology, 82
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Hill’s sign (Leg BP>arm BP more than 60 mmHg) it’s presence indicates severe AR.
Investigation:
EKG : Left atrial enlargement , left ventricular hypertrophy
CXR : Left atrial enlargement , left ventricular hypertrophy and dilated aorta
Echocardiography : for diagnosis and severity evaluation
Management :
1. Medical treatment: vasodilator such as nifedipine , no evidence of IE prophylaxis
2. Surgical treatment
Severe AR : LVH, presence of peripheral sign
Symptomatic: NYH class II-IV
LVEF<50%
LV dimension: diastolic phase > 75 mm, Systolic phase > 55 mm
Management of Warfarin
INR Management
< 1.5 Increase 10-20-% of warfarin
1.5 -1.9 Increase 5-10% of warfarin
2 - 3 Continous same dose
4 – 4.9 Hold warfarin 1 day then decrese 10%
5 – 8.9 no bleeding Omit 1-2 doses, Vit K 1 mg orally
9 no bleeding Vit K 5-10 mg orally
Major bleeding with any INR Vit K 10 mg IV plus FFP
repeat Vit K every 12 hrs if needed
83.
Medicine: Cardiology, 83
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
AHA Guidelines for IE Prophylaxis 2007
1. Dental disease may increase IE risk, but emphasis should shift from antibiotic prophylaxis for dental
procedures to improved dental care and oral health in patients with conditions that carry the highest risk for IE.
2. IE prophylaxis is reasonable (Class IIb, level of evidence C) for dental procedures that involve gingival tissues
or the periapical region of a tooth and for procedures that perforate the oral mucosa, in patients with cardiac
conditions associated with the highest risk for adverse outcomes from IE:
Prosthetic cardiac valve
Previous IE
Unrepaired congenital heart disease (including palliative shunts and conduits) : Tetralogy of Fallot,
Transposition of the great vessels, Ebstein's anomaly, Tricuspid atresia, Total anomalous pulmonary
venous return, Truncus arteriosus, Hypoplastic left heart syndrome, Critical pulmonary valvular stenosis,
Interrupted aortic arch, Pulmonary valve atresia, Coarctation of the aorta, Pulmonic stenosis
Completely repaired congenital heart defect with prosthetic material or device, during the first 6 months
after the procedure
Repaired congenital heart disease with residual defects at the site or adjacent to the site of a prosthetic
patch or device
Cardiac transplantation recipients who develop cardiac valvulopathy
3. If administered, antibiotics should be given in a single dose one hour before the procedure. The preferred
antibiotic is amoxicillin (2 g in adults and 50 mg/kg in children).
4. IE prophylaxis is no longer recommended for patients with mitral valve prolapse.
5. IE prophylaxis is not strongly recommended for respiratory tract procedures and not recommended at all for
bronchoscopy, unless incision of the respiratory tract mucosa is necessary.
6. IE prophylaxis is not recommended for GU or GI procedures.
Infective Endocarditis
Clinical Manifestation
Pathogenesis Clinical manifestation
Destruction of heart valve Murmur, heart failure, aortic aneurysm
Dislodge of vegetation Embolic phenomenon; infarction ; extremities, bowel, brain, heart, retina
Infection spreading Sepsis
Immunologic process Glomerulonephritis, petichial hemorrhage, microhemorrhage of retina (Roth
spot), skin, finger nail (Osler node), rheumatoid factor
84.
Medicine: Cardiology, 84
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Other signs: constitutional symptoms, clubbing of fingers, splenomegaly
Diagnostic criteria (Modified Duke criteria)
2 majors
1 major + 3 minors
5 minors
Major criteria
Positive blood culture Typical organisms from two separate blood culture, or
Any organism persistently > 12 hr, or > ¾ of samples
Evidence of endocardial
involvement
Echocardiogram : vegetation, valvular abscess
Minor criteria
Predisposing risk factor Heart condition, IV drug abuse
Fever > 38
Vascular phenomena Arterial emboli, petichial hemorrhage, conjunctival hemorrhage,
Janeway lesions, splinter hemorrhage (nail)
Immunological phenomena Glomerulonephritis, Osler’s node, Roth spots, rheumatoid factor
Microbiological evidence + hemoculture, echocardiogram แต่ไม่เข้า major criteria
Management :
- Viridans streptococci and Streptococcal bovis :
-Fully susceptible to penicillin : 4 wks of Penicillin G 12-18 million U/day IV q 4 h
or 2 wks of Penicillin G 12-18 million U/day IV q 4 h + 2 wks of Gentamycin 3mg/kg/day IV OD
-Relatively resist to penicillin : 4 wks of Penicillin G 24 million U/d IV q 4 h + 2 wks of Gentamycin 3 mg/kg IV OD
-Penicillin resistant : 4 wks of Vancomycin 30 mg/kg/day IV q 12 h + 2 wks of Gentamycin 3 mg/kg IV OD
- Staphylococci :
-MSSA : Cloxacillin 12 gm/day 4-6 wk+ gentamicin 3 mg/kg/day devide q 8 h 3-5 day
-MRSA : Vancomycin 30 mg/kg/day IV q 12 h 4-6 wks + Gentamycin 1 mg/kg IV devide q 8 h 3-5 day
- For prosthetic valve : Refer to cardiologist
Rheumatic Fever
Diagnostic criteria (Jones’ criteria)
2 major or 1 major + 2 minor + supporting evidence of Strep. Infection (↑ titer of Streptococcal antibodies (ASO,
Anti-DNase), Positive throat culture for gr. A Strep)
Major criteria
Carditis murmur, cardiac enlargement, congestive heart failure, pericardial rub
85.
Medicine: Cardiology, 85
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Polyarthitis Asymmetric, migratory, large joint involved, no permanent deformity,
spontaneous heal in 2-4 wks or respond well with NSAIDs,
Chorea (Sydenham’s) Involuntary purposeless rapid movements + muscular weakness + emotional
labiality
Erythema marginatum Trunk, ไม่นูน, ไม่เจ็บ, ไม่คัน, วงสีชมพูรอบบริเวณขาวซีดตรงกลาง
Subcutaneous nodules Not tender, firm, movable, usually found on tendons
Minor criteria
previous rheumatic fever / heart
Arthalgia
Fever
Acute phase reactant : ESR / CRP
EKG : prolonged PR interval
Management :
- Benzathine penicillin – 1.2 million U IM OD x 10 days, oral penV dose
- Anti-inflamatory drug - Steroids if carditis : dose 2 mkday (40-60 mg/day)
- NSAIDs if carditis : dose 100 mkday (6-8 g/day)
- Prophylaxis : - Primary – ATB when streptococcal sore throat
- Secondary – prevent of recurrent rheumatic fever – life long benzathine penicillin 1.2 mu IM q 1 mo. or Penicillin
V 250 mg bid
Myocarditis
History Physical examination Investigation
Fever, fatique, palpitation, CHF
in pt with LV dysfunction
Viral myocarditis มักเริ่มด้วย
URI, flulike syndrome, and viral
nasopharyngitis or tonsillitis
Fever
Tachycardia
Soft S1; S3 common
CK-MB : Isoenzyme and cardiac
troponins may be elevated in absence of
MI
EKG : Transient ST-T wave abnormalities
CXR : Cardiomegaly, pulmonary
congestion
Management
1. Rest and Oxygen
2. Standard therapy :
a) ACEI : Captopril (Capoten)
86.
Medicine: Cardiology, 86
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Adult : 6.25-12.5 mg PO tid; not to exceed 150 mg tid
Pediatric : 0.15-0.3 mg/kg PO bid/tid
b) Loop diuretics; Furosemide (Lasix) for CHF
Adult : 20-80 mg/d PO/IV; titrate up to 600 mg/d for severe edematous states
Pediatric : - 1-2 mg/kg/dose PO; not to exceed 6 mg/kg/dose; do not administer > q6hr
- 1 mg/kg IV/IM slowly under close supervision; not to exceed 6 mg/kg
c) Digoxin (Digitek, Lanoxicaps, Lanoxin)
Adult : 0.125-0.375 mg PO qd
Pediatric : - <5 years: Not established
- 5-10 years: 20-35 mcg/kg PO
- >10 years: 10-15 mcg/kg PO
- Maintenance dose: Use 25-35% of PO loading dose
i) Beta- blockers; Carvedilol (Caraten) (ห้ามให้ใน acute heart failure ต้อง control HF stable ก่อน)
Adult : 6.25-25 mg PO bid as tolerated (maximum of 75 mg/d if <85 kg, 100 mg/d if >85 kg)
Pediatric : Not established
3. Immunosuppression (Controversial benefit) : IVIG , steroids , azathioprine, cyclosporine cytoxan , OKT3
4. Refer to cardiologist
Medicine: Chest, 96
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Hemoptysis
คือมีไอเป็นเลือดปริมาณ 100 - 600 mL ภายใน 24 ชม.
แบ่งเป็น Massive hemoptysis และ non massive hemoptysis (มีเพียง 5% ที่เป็น massive แต่ mortality rate 80%)
Massive hemoptysis: เลือดออก > 150 ml ต่อครั้ง หรือ > 600 ml ใน 24 hr หรือมีการหายใจล้มเหลวถือเป็น
emergency condition
Essential Inquiries Investigation
- Nasopharyngeal or gastrointestinal
bleeding ?
- History of smoking or previous lung
infection เช่น TB
- Fever, cough, and other symptoms of
lower respiratory tract infection
- CBC, BUN/Cr และ coagulogram
- CXR: CA lung, TB, pneumonia
- Sputum analysis: cytology, gram stain, culture : TB
- Flexible bronchoscopy เพื่อดูตาแหน่งเลือดที่ออกว่าออกจากข้างใดหรือมี
endobronchial lesion หรือไม่ หรือทาเพื่อการรักษาเช่นการใส่ balloon เพื่ออุด
หลอดลมบริเวณปอดที่มีเลือดออก
- High-resolution chest CT (อาจพิจารณาทาในผู้ป่วยที่ผล CXR ปกติ เพื่อดู
ว่ามี bronchiectasis หรือ parenchymal หรือ vascular lesion ที่ผิดปกติหรือไม่)
Causes of hemoptysis
สาเหตุ อาจจา “BATTLE CAMP”: Bronchitis, bronchiectasis, aspergilloma, tumor, tuberculosis, lung
abscess, emboli, coagulopathy, autoimmune disorders, AVM, alveolar hemorrhage, mitral stenosis,
pneumonia โดย 90 % ของcases จะเป็น TB, Bronchiectasis, Lung abscesses
Airways COPD, bronchiectasis, and bronchogenic carcinoma
Pulmonary vasculature
Left ventricular failure, mitral stenosis, pulmonary embolism, arteriovenous
malformations (AVM)
Pulmonary parenchyma
Necrotizing pneumonia, inhalation of crack cocaine, or autoimmune diseases
(diffuse alveolar hemorrhage เช่นใน Goodpasture disease, Wegener
granulomatosis, microPAN
Infection Acute or chronic bronchitis, pneumonia, tuberculosis
Pulmonary venous hypertension mitral stenosis, pulmonary embolism
Iatrogenic hemorrhage
Transbronchial lung biopsies, anticoagulants, or pulmonary artery rupture due to
distal placement of a balloon-tip catheter.
97.
Medicine: Chest, 97
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
When to admit
- To stabilize bleeding process in patients at risk for massive hemoptysis
- To correct disordered coagulation (clotting factors or platelets, or both)
- To stabilize gas exchange
Management
Initial management : ABCD
• Clear airway : Suction เอาเลือดออก, ถ้า poor gas exchange, rapid ongoing hemoptysis, hemodynamic instability, or severe
shortness of breath พิจารณา Intubate (ถ้าไม่สาเร็จอาจทา cricothyroidotomy ไปก่อน)
• Oxygen supplement keep SpO2 > 95 %
• Bed rest, นอนศีรษะสูง, นอนตะแคงทับปอดด้านที่สงสัยว่าเลือดออกลงเพื่อป้ องกันไม่ให้ปอดที่ดีมีเลือดเข้าไปซึ่งจะเกิดปัญหาการ
แลกเปลี่ยนก๊าซ
• ให้การรักษาจาเพาะถ้าทราบสาเหตุ
• Consult intervention radiologist to stand-by emergency embolizaiton
Further Management : Massive pneumothorax
Localize the source of the bleeding
- early bronchoscopy is the procedure of choice.
- Flexible bronch. should be performed on patients (who should be intubated prior to this). If bleeding
is so rapid to make visualization difficult,then rigid bronch. can be used (more effective suction)
- If bronchoscopy is unsuccessful,angiography can be performed.
Consult for Stop bleeding
- Consult radiologist : Pulmonary angiography and embolization (ตามโรงเรียนแพทย์)
- Balloon tamponade via bronchoscopy
- Placement of a double lumen ETT specially designed for selective intubation of the right or left
mainstem bronchi
- Consider surgery for lateralized uncontrollable massive hemoptysis unresponsive to other measures
หาและแก้ไข cause
Management : Non massive pneumothorax
Mild to moderate(non massive): conservative by medication ตามสาเหตุที่เกิด
98.
Medicine: Chest, 98
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Asthmatic Attack & COPD with exacerbations
History Clinical Presentation Investigation
- History of asthma
- Triggers เช่น
Infection (โดยเฉพาะ viral infection),
pollution
- Frequency, duration, severity
- Current medications
- Increase cough and sputum
- Dyspnea, tachypnea
- prolonged expiratory phase and
wheezing
- Respiratory failure : ซึมลง, absent
breath sound, pulsus paradoxus,
abdominal paradox, PaO2 < 60,
PaCO2 >45 mmHg
- CXR : ไม่จาเป็นทุกราย อาจทาเมื่อสงสัย
ภาวะอื่นร่วมด้วย เช่น FB, pneumonia,
CHF, pneumothorax เป็นต้น
- ABG in severe case
- PEFR access severity (ถ้าทาได้)
Management ( COPD ที่มาด้วยเหนื่อยมากขึ้น ต้องระวังภาวะ pneumothorax ไว้ด้วย)
1. พิจารณา Intubation เมื่อมี respiratory failure ดังนี้ )อาจ try พ่นยาก่อน 2-3 ครั้ง(
RR > 35, O2 sat > 90%, SpO2 < 70 , SpCO2 > 55 (except in chronic retainers)
2. O2 supplement ; asthma keep SpO2 90-92%, COPD keep 90 – 92% ระวังอย่าให้ O2 conc. ที่มากเกินไป
3. Short acting 2 agonist
- Fenoterol + ipratropium bromide (Berodual®
) 4 – 8 puffs ผ่านทาง spacer ทุก 20 min หรือให้เป็น solution 2 ml ผสม
NSS 2 ml ผ่านทาง nebulizer ก็ได้ หรือ
- Salbutamol (Ventolin®
) (2.5 mg/ml) 1-2 ml ผสมใน NSS 2-3 ml พ่นผ่านทาง nebulizer โดยใช้ O2 flow 6 – 8 LPM ทุก
15 – 30 นาที ในชั่วโมงแรก หรือใช้ MDI device โดยพ่น 2-4 puff ผ่านทาง spacer
- Beradual ดีกว่า ventolin ในเรื่องมีปัญหาใจสั่นน้อยกว่า,ออกฤทธิ์ได้นานกว่า,ช่วยลด secretion ได้มากกว่า (ventolin ราคาถูกกว่าและ
ออกฤทธิ์เร็วกว่าเล็กน้อย)สาหรับ asthma จะ ventolin หรือ beradual ก็ไม่ต่างกันนัก
4. Oral prednisolone (30 mg/day) or dexamethasone 5 mg iv q 6 hr (ในไทยเป็น 4 mg IV q 6 hr)
If stable, continue oral prednisolone 30 mg/day นาน 5 – 7 วัน
5. Other medications
- Antibiotic ในรายที่สงสัย bacterial infection หรือกรณีที่ผู้ป่วยมีอาการเหนื่อยร่วมกับปริมาณเสมหะมากขึ้นและ/หรือเสมหะเปลี่ยนสี
- หลีกเลี่ยง sedative drugs เนื่องจากมีฤทธิ์กดการหายใจได้
- Mucolytics: not supported by data
6. พิจารณา Admission เมื่อ (ง่ายๆ ให้ดูว่าเหนื่อยจนไม่สามารถถามตอบครบประโยคได้ก็พิจารณา admit)
Asthma
- Patient’s condition doesn’t improved or PEFR < 200 despites 60 min of treatment
- History of severe asthmatic attack or intubation
- Co-morbidity, high risk for death from the attack
COPD
- Not response to initial treatment, cyanosis, dyspnea at rest, signs of respiratory failure
99.
Medicine: Chest, 99
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
- Multiple comorbidities เช่น CHF, coronary artery disease, chronic kidney disease เป็นต้น
7. Monitoring
- Serial physical examination, pulse, RR, BP
- CXR, ABG ใน severe case หรือไม่ตอบสนองต่อการรักษา หรือมีการวินิจฉัยแยกโรคอื่นๆ ด้วย
- ใน asthma อาจ Serial PEFR q 1 -2 hr (ถ้าทาได้)
8. After discharge : แนะนาเรื่องการใช้ยาและวิธีการใช้ยาสูดที่ถูกต้อง, หลีกเลี่ยงสิ่งกระตุ้น, รักษาโรคร่วมที่สาคัญ เช่น allergic rhinitis, GERD
และพิจารณาปรับยาควบคุมอาการหากก่อน exacerbations ครั้งนี้ผู้ป่วยยังคุมอาการไม่ดี
SVC Obstruction
not an emergency unless there is tracheal compression
History Physical examination Investigation
Causes
Malignant tumor
(common) : Lung
cancer, Lymphoma
Nonmalignant (rare)
: Thrombosis, Goiter,
Aortic aneurysm
- Distended neck vein
- Isolated upper limbs edema, periorbital
and facial edema with flushing
- Pulmonary manifestations : dyspnea,
tachypnea, cough, crackles, rales
- More severe symptoms in recumbent
position or after sleeping
- Prominent chest wall collateral vein (in
slow growing tumor)
- Sequelae of increased intracranial
pressure (less common)
- Special test : Pemberton’s test
Lift the arms over the head for >1 min
Observe : elevated JVP, increased facial
cyanosis/plethora, inspiratory stridor
- Investigations :
CXR : Pleural effusion (aspiration :
transudate pleural effusion)mass,
widening mediastinum
CT chest with contrast (Test of choice) or
MRI (if C/I for contrast)
Managements :
Initial management : symptomatic treatment
100.
Medicine: Chest, 100
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
- ABCs, O2 therapy and head elevation 30 – 45 degree
- Dexamethasone 4 mg/6 hr : for increase ICP and lymphoma/thymoma
- Diuretics and low salt diet
- Treat IICP if presented : hyperventilation, mannitol (loading dose 1mg/kg of 20% manitol solution) with fluid
replacement (input = urine output)
- ห้ามทาหัตถการที่แขนข้างนั้น
REFER for specific treatment
- Tissue Dx and specific Rx :
- Radiotherapy : Non-small cell CA lung, metas. solid tumor
- Chemotherapy : Small cell CA lung, lymphoma, germ cell CA
- Balloon venoplasty and SVC stenting
Approach to Acute Dyspnea
Causes : respiratory, cardiovascular and metabolic (anemia, metabolic acidosis)
Causes History Physical examination
Pneumonia - Fever
- Cough , sputum, pleuritic chest pain
- Fine crackles
- Signs of consolidation or pleural effusion
Pulmonary
embolism
- Risk : prolonged immobilization, recent
surgery (esp. lower limb), malignancy,
DVT, oral contraceptive pills
- Desaturation, tachypnea, respiratory
distress
- อาจพบ edema of legs (DVT), primary
cancer site, ตรวจร่างกายทางระบบหายใจมักจะ
ปกติ
Spontaneous - Sudden onset dyspnea and pleuritic - Trachea shift to contralateral site
101.
Medicine: Chest, 101
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
pneumothorax
(primary or
secondary)
chest pain,
- Young tall thin (primary)
- History emphysema / interstitial lung
disease (secondary)
- อาจพบ subcutaneous emphysema
- Decreased breath sound, vocal
resonance and fremitus
- Hyperresonance on percussion
Asthma - Recurrent wheezing, dyspnea or cough
esp. at night or after exercise
- Hx or family Hx of atopy or asthma
- Associated with specific events/agents
- ตรวจร่างกายมักจะปกติ
- Expiratory wheezing during
exacerbations
Foreign body
aspiration
- ประวัติ aspiration หรือในกลุ่มเสี่ยง เช่น
neurologic diseases, alcoholism เป็นต้น
- Localized wheezing / crackles
- Decreased BS at involved side
(atelectasis)
Non-cardiogenic
pulmonary edema
- ARDS
- Noxious gas in halation
- High altitude without acclimatization
- Neurogenic pulmonary edema
- ARDS- shock, conjuctival and axillary
petechiae (fat embolism), blood
transfusion (TRALI)
- Noxious gas - conjunctivitis, pharyngitis,
wheeze
Cardiogenic
pulmonary edema
- CHF - dyspnea, orthopnea, PND, ankle
edema
- Acute MI – angina
- Edema, distended neck vein
- Cardiomegaly, fine moist crackles,
expiratory wheeze
Hyperventation
syndrome
- Anxious mood and associated with some
events
- Carpopedal spasm, tachypnea
- ตรวจร่างกายอยู่ในเกณฑ์ปกติ
Trick •Dyspnea ถ้าแยกสาเหตุตามBlood gas จะมี 1) Hypercapnea 2) Hypoxemia 3) Metabolic acidosis ทั้ง
Wide/normal AG และ hypercatabolic state เช่นไข้ , SIRS 4) สุดท้ายอย่าลืม psychogenic, แต่กรุณา rule out สาเหตุ
อื่นก่อน
•ระวัง ! คนไข้หอบ SpO2 ดีไม่ใช่ psychogenic เสมอไป ที่หลุดบ่อยคือ acidosis (DKA, AKA, sepsis, AKI, drug-
induced metabolic acidosis)
คนไข้หอบ Lungs clear น่ากลัวไม่แพ้มี lungs sign ^^
- lungs clear + hypoxemia ระวังกลุ่ม shunt effect โดยเฉพาะ Pulmonary emboli
- หอบ + lungs clear + O2 ดี ระวัง acidosis มากๆ
Medicine: Chest, 108
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Investigation อื่นๆใน chest medicine
Easy Chest X-ray
Normal chest X-ray : โครงสร้างและอวัยวะต่างๆ ที่เห็นจากภาพท่า PA และ lateral view PA chest X-ray
1 First rib 9 Left atrium
2 Trachea 10 Right ventricle
3 Aortic knob 11 Left ventricle
4 SVC 12 Right atrium
5 Carina 13 Descending Aorta
6 Right PA 14 IVC
7 Left PA 15 Air in stomach
8 Pulmonary trunk
Lateral chest X-ray
1 Trachea 10 Right ventricle
2 Scapula 11 Left ventricle
3 Aortic arch 12 Right diaphragm
4 Left PA 13 Left diaphragm
5 Ascending Ao 14 IVC
6 Right PA 15 Air in stomach
7 Left main bronchus 16 Breast
8 Retrosternal space A Minor fissure
9 Left atrium B Major fissure
A
B
109.
Medicine: Chest, 109
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
หลักเบื้องต้นการอ่านภาพรังสีทรวงอก
Right film? (right patient)
Technical consideration
Side marker (left or right)
Projection (PA or AP view)
ตาแหน่งที่ใช้สังเกต PA AP
- C-spine เห็น lamina ชัด, เป็นมุมแหลม เห็น vertebral endplate ชัด, เป็นสี่เหลี่ยม
- Clavicle Medial end ต่ากว่า lateral end Medial end สูงกว่า lateral end
- Scapula เงา scapula อยู่นอก lung field เงา scapula ซ้อนอยู่ใน lung field
- Air-fluid level เห็นในกระเพาะอาหาร (ท่า upright) ไม่เห็น air-fluid level ในกระเพาะอาหาร
Posture (supine or upright)
Rotation (เช่น เปรียบเทียบระยะจาก medial end ของ clavicle ถึงขอบของ vertebral body ที่ระดับเดียวกัน เป็นต้น)
Extension of inspiration (full inspiration anterior rib: 5th
- 6th
rib or posterior rib: 9th
- 11th
rib)
Exposure quality (poorly penetrated film: diffusely light, over penetrated film: diffusely dark)
5 densities : air, fat, water/soft tissue, bone, metallic
Silhouette sign : ขอบเขตรอยโรคกลมกลืนกับโครงสร้างอื่นที่มีความหนาแน่นใกล้เคียงกัน ช่วยระบุตาแหน่งรอยโรค ดังรูป
110.
Medicine: Chest, 110
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
ลักษณะของส่วนต่างๆ ที่เห็นจากภาพรังสีทรวงอก
Trachea ควรอยู่ตรงกลาง (midline)
Heart ขนาด < 1/2 ของความกว้างทรวงอก (cardiothoracic ratio), กรณีที่มี hyperinflation อาจพบลักษณะ tall และ narrow ได้
(tubular heart)
Mediastinum มีขนาดกว้างขึ้นในหลายกรณี เช่น
o Mediastinal mass
- Anterior mediastinal mass เช่น substernal thyroid, lymphoma, thymoma, teratoma
- Middle mediastinal mass เช่น aortic aneurysm, bronchogenic cyst
- Posterior mediastinal mass เช่น neurogenic tumor, paravertebral mass, esophageal
dilatation, aortic aneurysm
Hilar (ประกอบด้วย bronchus, lymph node และ pulmonary artery) ข้างซ้ายอยู่สูงกว่าขวาเล็กน้อย
o อาจถูกดึงรั้งขึ้นหรือลงจากตาแหน่งปกติหากเกิด fibrosis หรือ atelectasis
o Enlarged hila : hilar lymph node, pulmonary artery (pulmonary hypertension), lung mass
(bronchogenic CA)
o Calcification (lymph node) : old TB, silicosis (egg-shell calcification), histoplasmosis
Diaphragm ข้างขวาสูงกว่าข้างซ้ายเล็กน้อย
o Elevated hemidiaphragm : decreased lung volume (atelectasis, fibrosis), phrenic nerve palsy
(diaphragmatic paralysis), hepatomegaly, subphrenic abscess, subpulmonic effusion,
diaphragmatic rupture
Lung parenchyma : alveolar and interstitial (nodular, reticular and reticulonodular) infiltrates
o Nodular pattern : neoplasm, infection, granuloma (military TB), pneumoconiosis
o Reticular pattern : acute interstitial changes (cardiac / non-cardiac pulmonary edema (ระยะแรก),
atypical pneumonia), fibrosis (TB), neoplasm (lympangitis carcinomatosis จะเด่นบริเวณปอดส่วนล่าง
และอาจเห็น Kerley’s B lines), interstitial lung diseases (เช่น idiopathic pulmonary fibrosis)
o Alveolar pattern : pulmonary edema, ARDS, pneumonia, pulmonary hemorrhage, fat emboli เป็น
ต้น
o Ring shadow : bronchiectasis (honeycomb appearance), cavitating lesion (TB, necrotizing
pneumonia or lung abscess, tumor)
o Linear opacitites : septal lines (Kerley’s B lines), plate-liked atelectasis
111.
Medicine: Chest, 111
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Sputum examination
Sputum characteristics
o Clear & colorless : chronic bronchitis
o Yellow / green : pulmonary infection
o Red : hemoptysis
o Black : smoke, coal
o Frothy white / pink : pulmonary edema
Sputum tests
o AFB : TB
o Modified AFB : Nocardia spp.( also gram
positive stain)
o GMS, PAS : PCP, Histoplasmosis,
Aspergillosis, Candidiasis
Sputum gram stain
o True sputum Squamous epi < 10, PMN >25
HPF
o Gram negative bacilli (common) : P.
aeruginosa, E.coli,
o Gram negative diplococci : Neiseseria spp.
(intracellular)
o Gram positive diplococci : S. pneumoniae
o Gram positive cocci : S.aureus(cluster)
o Gram negative coccobacilli : A. baumannii,
H.influenza
Arterial blood gas (ABG) analysis
อ่าน oxygenation, ventilation และ acid-base balance
o ค่าปกติของ arterial blood gas
Parameter Normal value
pH
PaCO2
PaO2
HCO3
-
O2 saturation
7.35 – 7.45
35 – 45 mmHg
80 – 100 mmHg
22 – 26 mEq/L
97 – 100%
o ความปกติดุลกรดด่าง : ลูกศรไม่มีขีดกั้น เป็น 1o
disorder
ภาวะ PaCO2 HCO3
-
Metabolic acidosis
Metabolic alkalosis
Respiratory acidosis
Re piratory alkolosis
o สูตรที่ใช้บ่อย
PaO2 = 100 – (อายุ/4)
A-a gradient = PAO2 – PaO2 ; ค่าปกติ = 2.5 + (อายุ/4)
PAO2 = (FiO2 × 713) – (PaCO2/R) ; R = 0.8 เมื่อ FiO2 < 0.6
R = 1.0 เมื่อ FiO2 ≥ 0.6
Medicine: Chest, 113
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Doses of asthma relievers
Drugs: albuterol/salbutamol, fenoterol, levalbuterol, metaproterenol, pirbuterol, terbutaline
Pretreatment before exercise: 2 puffs MDI or 1 puff DPI
For asthma attack: 4-8 puffs q 2-4 hr หรือ q 20 min X 3 under medical supervision
Doses of asthma controllers
1. ICS (ขนาดยาใช้ในผู้ป่วยอายุมากกว่า 5 ปี)
114.
Medicine: Chest, 114
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Drugs Children daily dose (µg)
low medium high
Budesonide 100-200 >200-400 >400
Fluticasone 100-200 >200-500 >500
2. Oral corticosteroid: 5-40 mg/day of prednisolone equivalent, For acute attack 40-60mg/day in one or two
divided doses (adult), 1-2mg/kg daily (children)
Side effects=adrenal suppression, osteoporosis, growth retardation, muscle weakness, DM, hypertension,
cataract
3. Long acting β2 agonist:
Inhale Formoterol: DPI (12 µg) 1 puff bid., MDI 2 puffs bid.
Salmeterol DPI (50 µg) 1 puff bid., MDI 2 puffs bid.
Oral Salbutamol 4mg q 12 hr.
Terbutaline 10mg q 12 hr.
MDI= metered dose inhaler, DPI= dry powder inhaler
Side effects=tachycardia, skeletal muscle tremor, anxiety, hypokalemia, headache
4. Sustained release theophylline: 10mg/kg/day, maximum ไม่เกิน 800mg แบ่งกิน 1-2 doses ควร monitor theophylline
level หลังเริ่มให้
Side effects=tachycardia, arrhythmia, nausea vomiting, high serum level can cause seizure
5. Anti-leukotrienes:
Drugs Adults Children
Montelukast 10 mg oral hs 5 mg oral hs (อายุ 6-14 ปี)
4 mg oral hs (อายุ 2-5 ปี)
Side effects =
oral candidiasis,
hoarseness,
skin thinning
115.
Medicine: Chest, 115
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Pranlukast 450 mg oral bid
Zafirlukast 20 mg oral bid 10 mg oral bid (อายุ 7-11ปี)
Zileuton 600 mg oral qid
Side effects=no specific adverse effects to date, Zafirlukast และ Zileuton อาจพบ elevation of liver enzyme, มี
limited case report พบ reversible hepatitis and hyperbilirubinemia for Zileuton, Liver failure for Zafirlukast
6. Anti-IgE: Omalizumab maximum dose 150mg subcutaneously injected q 2-4 weeks
7. Combined ICS and Long acting β2 agonist:
116.
Medicine: Chest, 116
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
COPD : GOLD Guideline 2011
Diagnosis
Consider COPD if any indicators of these are present in an individual over age 40.
But spirometry is required to make a clinical diagnosis of COPD , the present of postbronchodilator
FEV1/FVC < 0.7 confirms the presence of persistence airflow limitation and thus of COPD
Degree of severity Assessment of stable COPD
117.
Medicine: Chest, 117
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
1. Non pharmacologic management
2. Pharmacologic management
(SA: Short acting , LA : Long Acting, ICS : Inhaled corticosteroid, PDE-4 : Phosphodiesterase-4 )
118.
Medicine: Chest, 118
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Spirometry
o Obstructive :FEV1 จะลดมากกว่า FVC ค่า FEV1/FVC ratio < 70%
o Reversibility : หลังพ่น bronchodilator ค่า FEV1 เพิ่มขึ้น >200 ml และ >12%
o Restrictive : FEV1 และ FVC ลดลงในสัดส่วนที่ใกล้เคียงกันดังนั้น FEV1/FVC ratio จะปกติ ( 70%) และค่า FVC ≤
80% predicted
Community-acquired pneumonia (CAP)
Symptoms Signs Investigations
- Fever
- Cough
- Dyspnea
- Pleuritic chest pain
- Fine crackles
- Signs of consolidation or pleural
effusion
- CBC: leukocytosis
- Chest x-ray : consolidation,
infiltrates, effusion
- Sputum G/S and Culture
- Hemoculture
การจาแนกความรุนแรง ทาได้หลายวิธี
1. CURB-65 score : confusion, urea (BUN) > 20 mg/dl, RR 30, BP < 90/60, Age 65
(score 0-1 : outpatient, 2 : admit to IPD, 3 : admit to ICU)
2. ATS guideline (2004) : ICU admission (1 major or 2 minor)
Major : mechanical ventilation, septic shock
Minor : SBP ≤ 90, multilobar disease, SpO2 < 90% or PaO2/FiO2 < 250
3. IDSA guideline (1995) : PSI scoring system
Management
OPD IPD : non-ICU
1. Previously healthy and no ATB in past 3 mo
- Clarithromycin (500 mg) PO bid x 5 days
[or] Azithromycin (500 mg) PO once,
then 250 mg OD x 4 d
[or] Doxycycline (100 mg) PO bid x 7-10 d
2. Comorbidities or ATB in past 3 mth
1.1 Levofloxacin 750 mg PO OD
[or] High-dose amoxicillin 1 g tid
[or] Amoxicillin/clavulanate 2 g bid หรือ
1. Levofloxacin (750 mg) PO or IV OD หรือ
2. Cefotaxime (1–2 g) IV q 8 hr
[or] Ceftriaxone (1–2 g) IV OD
[or] Ampicillin (1–2 g) IV q 4–6 hr
Plus
Clarithromycin (500 mg) PO bid
[or] Azithromycin 500 mg PO once,
then 250 mg OD
[or] Azithromycin 1 g IV once,
then 500 mg OD
119.
Medicine: Chest, 119
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
1.2Ceftriaxone 1–2 g IV OD
[or] Cefpodoxime 200 mg PO bid
[or] Cefuroxime 500 mg PO bid
plus Macrolides
2. สาหรับผู้ป่วย ICU และ special case เช่น
Pseudomonas และ CA-MRSA pneumonia แนะนาให้
ปรึกษาแพทย์ระบบทางเดินหายใจและโรคติดเชื้อร่วม
ประเมินและให้การรักษา
Health care-associated pneumonia (HCAP)
clinical as pneumoniaแบ่งเป็น
- Hospital-acquired pneumonia (HAP) เกิดหลังadmit 48 hr
- Ventilator-associated pneumonia (VAP) เกิดหลัง on ETT 48 hr
- Empiric broad-spectrum ATB in first 3-5 days
- Deescalator ATB ปรับลด spectrum ตาม sputum C/S & sensitivity
Management
ATB selection ( ATS guideline 2005) พิจารณาจาก
1.onset : early HAP in first 4 days
- late HAP admit ≥5 days สัมพันธ์กับการติดเชื้อดื้อยาและ poor prognosis
2.Risk for MDR pathogens
- Antimicrobial therapy in preceding 90 d
- Current hospitalization of 5 d or more
- High frequency of antibiotic resistance in the community or in the specific hospital unit
- Presence of risk factors for HCAP :
o Hospitalization for 2 d or more in the preceding 90 d
o Residence in a nursing home or extended care facility
o Home infusion therapy (including antibiotics)
o Chronic dialysis within 30 d
o Home wound care
o Family member with multidrug-resistant pathogen
o Immunosuppressive disease and/or therapy
Initial empiric therapy
a. Early onset or low risk MDR : H. influenzae, S. pneumoniae, MSSA, ATB-sensitive gram neg bacilli –E.coli, K.
120.
Medicine: Chest, 120
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
pneumoniae, Enterobactor spp.
1.1 Ceftriaxone 2 g IV OD
1.2 Quinolone : Levofloxacin,750 mg IV OD or Ciprofloxacin 400 mg IV q 8 h
1.3 Ampicillin/sulbactam
1.4 Ertapenem 1 g IV OD
b. Late onset or high risk MDR : P.aeruginosa, K. pneumoniae ( ESBL+), A.baumannii, MRSA, Legionella
pneumonia
2.1 Antipseudomonal cephalosporin
-cefepime 1–2 g IV q 8–12 h
-ceftazidime 2 g IV q 8 h
2.2 Antipseudomonal carbepenem
-imipenem 500 mg IV q 6 h or 1 g IV q 8 hr
-meropenem 1 g IV q 8 h
2.3 β-Lactam/β-lactamase inhibitor(piperacillin–tazobactam) plus Antipseudomonal
fluoroquinolone(ciprofloxacin or levofloxacin)
- Tazocin 4.5 g IV q 6h
2.4 Aminoglycoside (amikacin, gentamicin, or tobramycin) plus Linezolid or vancomycin
- Linezolid 600 mg IV q 12 h - vancomycin 15 mg/kg q 12 h
- Amikacin 20 mg/kg IV OD - gentamicin 7 mg/kg IV OD
- Tobramycin 7 mg/kg IV OD
Pulmonary Tuberculosis
Symptoms & Signs Investigation Diagnosis
- Chronic cough (>3 wks)
- Productive cough
- อาจมี hemoptysis
- Pleuritic chest pain
- Constitutional symptoms
- Fever
- Night sweats
1. CXR
2. Sputum AFB : เก็บเสมหะ
ตอนเช้าหลังตื่นนอน 2-3 วัน
3. Sputum culture
4. Others
- (Tuberculin skin test)
- Bronchoscopy
1. วัณโรคพบเชื้อ
1.1 AFB อย่างน้อย 1 ครั้ง ร่วมกับ CXR เข้าได้กับ
วัณโรคปอด
1.2 AFB อย่างน้อย 1 ครั้ง ร่วมกับ ผลเพาะเชื้อพบ
เชื้อวัณโรค
2. วัณโรคไม่พบเชื้อ
2.1 AFB และผลเพาะเชื้อ หรือไม่ทราบ แต่มี
121.
Medicine: Chest, 121
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
- Weight loss - PCR อาการทางคลินิก และ CXR เข้าได้กับวัณโรคปอด
2.2 AFB แต่ผลเพาะเชื้อพบเชื้อวัณโรค
Treatment : DOTS (direct observed therapy, short course)
1. First line drugs: 2HRZE + 4HR (สูตรอื่น เช่น 2HRE/7HR, 6RZE เป็นต้น)
CAT 2 : 2HRZES/1HRZE/5HRE
- Isoniazid (H) : 300 mg/d หรือ 5 mg/kg/d + Pyridoxine (Vitamin B6): 50-100 mg
- Rifampicin (R) : 10 mg/kg/d
- Pyrazinamide (Z) : 25-30 mg/kg/d ปรับขนาดยาถ้ามี severe renal insufficiency
- Ethambutol (E) : 15-25 mg/kg/d ปรับขนาดยาถ้ามี renal insufficiency
- Streptomycin (S) : 15 mg/kg/d ปรับขนาดยาถ้ามี renal insufficiency
หรือ ช่วง 2 เดือนแรกอาจใช้ Rifafour (ยา combination H+R+Z+E)
Bw(kg) Dose rifafour
< 40 2 tab PO hs + INH 1 tab hs
40-50 3 tab PO hs + INH ½ tab hs
>50 4 tab PO hs
2. ติดตามอาการผู้ป่วยและอาการข้างเคียงจากการใช้ยาอย่างใกล้ชิดในช่วงแรก
3. Follow up liver enzyme หลังเริ่มการรักษา 2 สัปดาห์
4. ติดตาม chest X-ray เมื่อสิ้นสุดการรักษา หรือก่อนหน้านั้นหากมีอาการเปลี่ยนแปลงโดยเฉพาะกรณียังไม่ได้ definite
diagnosis ของ TB ก่อนเริ่มการรักษา
Treatment failure
SputumAFB ยัง ที่ 5 เดือนหลังรักษา หรือเดิม sputum ถ้า clinical ไม่ตอบสนองต่อการรักษาให้เริ่มยารักษาแบบ MDR-TB
Start 2IRZE/4IR
2 months
Sputum AFB+ Sputum AFB-
Continue intensive
phase for 1 more
month then start
continuation phase 4
months (3IRZE/4IR)
start continuation
phase 4 months
(2IRZE/4IR)
5 months
Sputum
AFB-
Sputum
AFB+
Cured
Treatment
failure
Sputum C/S for drug
sensitivity, continue
anti-TB drug
Choose 3 sensitive drugs (has not been
used before), stop Rx when sputum AFB
– for at least 1 year
complete Rx
course
Sputum
AFB -
Start 2IRZE/4IR
2 months
Sputum AFB+ Sputum AFB-
Continue intensive
phase for 1 more
month then start
continuation phase 4
months (3IRZE/4IR)
start continuation
phase 4 months
(2IRZE/4IR)
5 months
Sputum
AFB-
Sputum
AFB+
Cured
Treatment
failure
Sputum C/S for drug
sensitivity, continue
anti-TB drug
Choose 3 sensitive drugs (has not been
used before), stop Rx when sputum AFB
– for at least 1 year
complete Rx
course
Sputum
AFB -
Start 2IRZE/4IR
2 months
Sputum AFB+ Sputum AFB-
Continue intensive
phase for 1 more
month then start
continuation phase 4
months (3IRZE/4IR)
start continuation
phase 4 months
(2IRZE/4IR)
5 months
Sputum
AFB-
Sputum
AFB+
Cured
Treatment
failure
Sputum C/S for drug
sensitivity, continue
anti-TB drug
Choose 3 sensitive drugs (has not been
used before), stop Rx when sputum AFB
– for at least 1 year
complete Rx
course
Sputum
AFB -
Things to follow
•Symptoms: fever, weight
•Side effects: liver
function, skin lesion
•Sputum AFB (เก็บหลังตื่นนอน 1
sample, เก็บที่ ร พ 1 sample)
•Smear negative patients:
ต้องตรวจ sputum ที่ 2 เดือนเพื่อ
ป้ องกกันการตรวจผิดพลาดในครั้งแรก
ถ้า negative อีกให้ F/U ด้วย
clinical ไม่ต้องตรวจ sputum
อีกแล้ว
•CXR ก่อนเริ่มรักษา และหลังจบ Rx
course
Medicine: Chest, 124
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Management
1. Admission : consult chest physician
2. ET intubation + ventilator : keep O2 sat > 90%
3. Mechanical ventilation and apply PEEP
4. Appropriate fluid management
5. Treat underlying causes eg. infection
6. Prevent complications : barotruama, volutrauma (pneumothorax) จากการใช้เครื่องช่วยหายใจ โดยควรตั้งเครื่องช่วย
หายใจให้ tidal volume ประมาณ 6 ml/kg, ได้ plateau pressure ไม่เกิน 30 cmH2O และตั้งค่า PEEP ที่เหมาะสม
ข้อควรรู้ : การตรวจร่างกายผู้ป่วย ARDS
1. ผลการตรวจร่างกายไม่มีลักษณะจาเพาะ
2. ผู้ป่วย ARDS ส่วนใหญ่ได้รับการใส่ท่อช่วยหายใจร่วมกับเครื่องช่วยหายใจ การตรวจพบว่าเสียงหายใจข้างใดข้างหนึ่งลดลงอาจเกิดจากปลายท่อ
ช่วยหายใจอยู่ลึกเกินไปใน main bronchus โดยเฉพาะด้านขวา หรืออาจเกิดจาก pneumothorax, atelectasis ที่ปอดข้างนั้นก็ได้
3. พยายามตรวจหาสาเหตุของภาวะ sepsis โดยเฉพาะภาวะติดเชื้อ เช่น acute abdomen, phlebitis, บาดแผลกดทับ, UTI,
pneumonia เป็นต้น เพราะเป็นสาเหตุของภาวะ ARDSที่พบได้บ่อย
4. ควรแยกภาวะ cardiogenic pulmonary edema ออกจากภาวะ ARDS โดยตรวจหาข้อมูลสนับสนุน เช่น volume overload,
distended neck vein, edema, hepatomegaly, ECG, PCWP เป็นต้น
Mass in chest
Mass in chest
Lung nodule
(size < 3 cm)
Mediastinal mass
Solitary
pulmonary nodule
Multiple
pulmonary nodule
Lung mass
(size > 3 cm)
ARDS
A : acute
R : ratio (PaO2/FiO2) < 200
D : diffused lung infiltrates
S : Swan-Ganz pressure < 18 mmHg
125.
Medicine: Chest, 125
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Solitary Pulmonary Nodule (SPN)
Benign or Malignant SPN
Factors favor a benign diseases Factors favor a malignant diseases
Age < 50
Nonsmoker
Size < 2 cm
No growth over 2-year period
Circular and regular shaped, ขอบชัด
Central lamination calcification
Age > 50
Smoker or previous smoker
Size > 3 cm
Steady growth over serial CXRs
Grossly irregular or speculated margin
Stippled or eccentric calcification
Solitary pulmonary nodule (size < 3 cm)
Previous CXR
yesno
Nodule changed
in size for 2 years
New nodule Not available
Follow up yearly CT chest with thin section
(HRCT)
Tissue diagnosis
Resection
Initially, follow up
every 3 months
Solitary Pulmonary Nodule ex.
1. Bronchogenic CA
2. Hamartoma
3. Histoplasmoma
4. TB granuloma
5. Bronchial adenoma
6. Solitary met
7. Round pneumonia
8. Rounded atelectasis
126.
Medicine: Chest, 126
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Multiple Pulmonary Nodule (MPN)
Cause
1.malignancy ( greater than 1 cm in diameter -- are more likely to be malignant)
2.benign (<5 mm, juxtaposed to visceral pleura or interlobar fissure, are more likely to be benign lesions)
Benign Tumors - Such as hamartomas. Hamartomas
Autoimmune - such as Wegeners granulomatosis, sarcoidosis, eosinophilic granules, and rheumatoid
nodules
Infections
- Bacterial infections – septic nodules, tuberculosis, nocardiosis
- Fungal infections – aspergillosis, histoplasmosis, coccidiomycosis, cryptococcosis
Lung Cancer
Pathologic type Location Specific features
NSCLC
Squamous cell CA Usually central May find cavitary lesions on imaging
Adenocarcinoma Often peripheral
- Pleural involvement in 20% of cases
- Less closely associated with smoking than other
types
- Can be associated with pulmonary scar /
fibrosis (scar tumor)
Large cell CA Usually peripheral
SCLC Central
- Highly correlated with smoking
- Tend to narrow bronchi by extrinsic
compression
- Wide spread metastasis are common
- Neuroendocrine origin : paraneoplasic
syndrome เช่น SIADH, Cushing syndrome
Medicine: GI, 128
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
GI
Upper Gastrointestinal Bleeding
UGIB
Hematemesis
Blood or coffee ground in NG tube
Melena
Hematochezia with hemodynamic instability
Resuscitation :
- Oxygen cannula (ETT if needed)
- 2 large-bore (≥ 18 G) IV catheters
- Obtain blood for blood typing, CBC, PT, aPTT, BUN, Cr,
Electrolyte, Blood sugar, LFT
- 0.9% NSS IV --> normalize V/S
(if shock --> load 100-200 cc in 15 min)
**no dextrose; no RLS in liver disease**
- Monitor V/S, I/O closely
- Crossmatch blood component
- Discontinue anticoagulant, antiplatelet, thrombolytics
if possible
Blood component replacement :
- PRC or whole blood
- Keep Hct. 25-30%
(depending on comorbidities)
- Keep Hb ~ 8 in variceal bleeding
- Vit.K and FFP to normalize PT
- Platelet transfusion if < 50000
* Clinical risk factor for poor
outcome
- age > 60 years
- severe comorbidity
- active or recurrent bleeding
- vital signs instability
- PRC transfusion ≥ 6 units in 24 hr.
-Iinpatient status at time of
bleeding
- severe coagulopathy
** Rockall scoring system
Score < 2 low risk, Score > 6 : high risk
Severity assessment : Hemodynamic status
Tachycardia --> mild (~10% loss)
Orthostatic hypotension --> moderate (~20% loss)
Shock --> severe (>30 % loss)
Patient assessment :
- Hx, PE
- NPO
- NG tube w/ gastric lavage
- Risk stratification
(Clinical risk factor for poor
outcome*, Rockall scoring
system**)
Variceal bleeding
- Hx of varices/variceal bleeding
- Hx of liver disease/cirrhosis
- Painless bleeding (usually hematemesis)
- >90% has hemodynamic change or Hct<30%
- Signs of portal HT/chronic liver disease: spider
nevi, caput medusa, ascites, splenomegaly.
hepatic encephalopathy
Non variceal bleeding
- Hx of peptic ulcers, H.pylori, NSAID/aspirin use
- Painless/painful bleeding (hematemesis/coffee
ground/melena)
- vary hemodynamic status
- No signs of portal HT/chronic liver disease
Low risk
High risk
Oral PPI double dose
- Omeprazole (40mg) P.O. bid
- Elective EGD
EGD w/in 24-48 hr
129.
Medicine: GI, 129
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Upper Gastrointestinal Bleeding :Variceal bleeding
- Admit
- NPO, IV fluid
- Oxygen therapy
- Record V/S, I/O, observe bleeding
- If continuous bleeding: Sengstaken-Blakemore
tube(SB);อย่าลืม ETTก่อน
Pharmacological therapy
Vasoactive drug therapy
- Somatostatin 250 mcg IV bolus
then IV infusion 250mcg/hr OR
- Octreotide 50 mcg IV bolus
then IV infusion 50 mcg/hr
ATB prophylaxis*
EGD w/in 24-48 hr
- Esophageal variceal band ligation
- Injection sclerotherapy
Success Fail
Rebleed
- SB tube 24-48 hr
- Re-endoscopy
Fail or Rebleed
Poor candidate
TIPS
Good candidate
Shunt surgery
*Antibiotic prophylaxis in cirrhotic pt. w/ UGIB
- Norfloxacin (400mg) PO bid x 7days OR
- Bactrim DS PO bid x 7days OR
- Ceftriaxone 1gm IV OD
in centers with a high prevalence of quinolone-
resistant organisms.
Prevention of recurrent variceal hemorrhage(by
5 days after bleeding is controlled)
- non selective beta-blocker eg. Propranolol
(20mg) P.O. bid (goal 25%HR)
- Nitrates
- Band ligation
-Combination
- TIPS or Surgery if rebleed
Continued pharmacological therapy
(up to 5 days)
Vasoactivedrug therapy
- Somatostatin IV infusion 250mcg/hr OR
- Octreotide IV infusion 50 mcg/hr
ATB prophylaxis
Variceal bleeding
130.
Medicine: GI, 130
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
-Omeprazole (20) 1 cap PO OD ac
-Lansoprazole(30) 1 cap PO OD ac
-Esomeprazole(20) 1 tab PO OD ac
-Pantoprazole (40) 1 tab PO OD ac
-Ranitidine (150) 1 tab PO bid
-Famotidine (40) 1 tab PO od
Upper Gastrointestinal Bleeding : non - variceal bleeding
- Admit
- NPO, IV fluid
- Oxygen therapy
- Record V/S, I/O, observe bleeding
Pharmacological therapy
- Pantoprazole 80mg IV bolus then IV infusion 8mg/hr
OR
- Omeprazole/Pantoprazole 40 mg IV push q12 hr OR
- Oral PPI double dose eg. Omeprazole 40 mg P.O.
bid
EGD w/in 24-48 hr
High risk Low risk
Endoscopic finding
Antisecretory
therapy
Endoscopic intervention
Success Fail
Continued pharmacological therapy (x3days)
- Pantoprazole 80mg IV bolus then IV infusion
8mg/hr OR
- Omeprazole/Pantoprazole 40 mg IV push
q12 hr OR
-Oral PPI double dose eg. Omeprazole 40 mg
P.O. bid
Rebleed
Consult Sx
Re-endoscopy
and hemostasis
Fail
OR
Then
- Omeprazole/Pantoprazole 20mg PO OD x 8wks
- Adherent clot
- Non-bleeding
visible vessel
- Active bleeding
- Clean base
- Spot
Indication for Surgery
1. Continued active bleeding and unable to perform endoscopy
2. Require blood transfusion > 6units
3. Failure of endoscopic treatment
4. Rebleeding after successful endoscopic treatment
If unavailable
Non-variceal bleeding
131.
Medicine: GI, 131
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Peptic Ulcer Disease
Clinical presentation
Symptoms: epigastric pain, DU usually night pain, relieved by food, GU usually worsened by food
Causes: H.pylori, NSAIDs, ASA, gastrinoma, carcinoid, malignancy, stress ulcers, CMV
Investigations: 1. H.pylori : urea breath test , serology , fecal antigen test, rapid urease test (CLO test)
2. EGD ±biopsy
3. UGI series เพื่อหา ulcer
4. EKG โดยเฉพาะในคนสูงอายหรือผู้ที่เสี่ยงต่อโรคหัวใจ
Gastric biopsy for H.pylori surveillance when :
- GU or DU (regardless ulcer activity)
- Atrophic gastritis
- Hemorrhagic/erosive gastritis
- MALToma
- Long term ASA and risk for PUD
- Long term ASA and Hx. UGIH or PUP
- Long term NSIADs
- Family history of Ca stomach
- After gastric cancer resection
Managements : Life style modifications, Discontinue NSAIDs and ASA ถ้าจาเป็นต้องใช้ควรให้ PPI ร่วมด้วย
ถ้าไม่พบเชื้อ H.pylori ให้ H2-blocker or PPI + antacid or sucralfate 6 -8 wksโดย F/U หลังให้ยา 2-4 wk
Drug dose Ranitidine (150) 1 tab po.bid. pc.; Famotidine (40) 1 tab po.od. hs.;Omeprazole (20) 1 cap po.od.ac.
; Lansoprazole(15) 1 FDT po. od. ac.; Esomeprazole(20) 1 tab po. od. ac
H.pylori eradication มีหลายสูตร ณ ที่นี้เป็น PPI-based triple therapy ให้ยา 7-14 วัน
โดยทั่วไปหลังรักษาด้วยการกาจัดเชื้อแล้ว ไม่
มีความจาเป็นต้องให้ยา anti-secretory
ต่ออีก ยกเว้นกรณี เป็น complicated
ulcer และมี comorbid condition
ผู้ป่วยเหล่านี้แนะนาให้ยา anti-secretory
ต่อประมาณ 4-8 สัปดาห์ แต่ในผู้ป่วยที่ต้อง
รับประทาน aspirinหรือ NSAIDsระยะยาวต้องได้รับ PPI คู่กันไปตลอด
การติดตามผลการรักษา
ใช้การติดตามดูอาการเป็นสาคัญ ไม่มีความจาเป็นต้องส่องกล้องตรวจหรือตรวจยืนยันว่ากาจัดเชื้อได้แล้วซ้าอีก ยกเว้นในกรณีต่อไปนี้
1. เป็น complicated ulcer เช่น มี bleeding หรือ previous perforation
2. มี intractable pain หรือ recurrent symptom
3. High risk gastric cancer (กรณีนี้ต้อง biopsy ซ้าเสมอ)
4. Patient’s wishes
132.
Medicine: GI, 132
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Dyspepsia
ประวัติ typical biliary colic มีลักษณะ ดังนี้
1. Typically epigastric or RUQ
2. Characteristically radiating to the back or through to the region of the
right scapula or right shoulder blade.
3. Usually sudden in its onset, reaching its maximum intensity in 15-60
minutes and invariable constant once it reaching its intensity.
4. The attack possibly lasting many hours before subsiding.
5. The pain usually assumes a characteristic pattern for each individual.
Rome III Criteria for the diagnosis of IBS
Irritable Bowel Syndrome can be
diagnosed based on at least 12 weeks
(which need not be consecutive) in the
preceding 12 months, of abdominal
discomfort or pain that has two out of
three of these features:
1. Relieved with defecation; and/or
2. Onset associated with a change in
frequency of stool; and/or
3. Onset associated with a change in
form (appearance) of stool.
Alarm features
(ควรได้รับการส่องกล้อง)
Age of onset > 55 years
Dysphagia
Persistent vomiting
Unexplained significant weight
loss
Evidence of GI blood loss
Diagnosis of Functional Dyspepsia
Most common cause (60-90%) of dyspepsia in general population
Hx: Young age, Long duration of symptoms, No alarm features
PE: Usually normal
EGD or upper GI study: Normal or only non-erosive gastritis
Mx: placebo effects 30-60%
133.
Medicine: GI, 133
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
อาการปวดลักษณะแบบ Ulcer-like
เลือกใช้ anti-secretory drugs เช่น
-Omeprazole (20) 1 cap po od ac
-Lansoprazole(30) 1 cap po od ac
-Esomeprazole(20) 1 tab po od ac
-Pantoprazole (40) 1 tab po od ac
-Ranitidine (150) 1 tab po bid
-Famotidine (40) 1 tab po od
Life style modifications: ได้แก่ การรับประทานอาหาร ไม่ควรทานจนอิ่มเกินไป ไม่ควรนอน
ทันที หลังทานอาหารอิ่มใหม่ๆ กินอาหารตรงตามเวลาทุกมื้อ หลีกเลี่ยงอาหารรสจัด ของดอง
น้าอัดลม งดสูบบุหรี่ งดดื่มสุรา งดการใช้ยาแก้ข้อและกล้ามเนื้ออักเสบ ระวังอย่าให้ท้องผูก ควร
ออกกาลังกาย ผ่อนคลายความเครียดและพักผ่อนให้เพียงพอ
อาการแบบ reflux-like หรือ dysmotility-like
เลือกใช้ prokinetic drugเช่น
- Domperidone 1tab pot id ac
- Metoclopramide(10) 1tab po tid ac
- Domperidone(100 1-2 tab po tid ac
ยากลุ่มอื่นที่อาจเลือกใช้ Antidepressants
amitriptyline(10-25) 2 tabs po hs -- 4 wks
134.
Medicine: GI, 134
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Chronic Diarrhea
Definition : passage of abnormally liquid or unformed stools at an increased frequency and more than 3 weeks in
duration (some reference ; more than 4 weeks) , but if persistent more than 2 weeks should be investigations.
Approach 1. แยกระหว่าง organicและ functional diarrhea
Organic Functional
ระยะเวลา < 3 เดือน > 3 เดือน
การดาเนินโรค เป็นตลอดเวลาหรือรุนแรงขึ้น เป็นๆหายๆ
ท้องเสียกลางคืน พบได้บ่อย ไม่ควรมี
ถ่ายเป็นเลือด พบได้ ไม่ควรมี
Constitutional symptoms พบได้ ไม่ควรมี
น้าหนักลด พบได้ ไม่ควรมี
ซีด พบได้ ไม่ควรมี
Albumin ต่า พบได้ ไม่ควรมี
2. แยกระหว่าง smallและ large volume diarrhea
Small volume diarrhea Large volume diarrhea
ตาแหน่งรอยโรค ลาไส้ใหญ่ด้านซ้าย ลาไส้เล็กหรือลาไส้ใหญ่ด้านขวา
ปริมาณอุจจาระ น้อย มาก
ความถี่ บ่อย ไม่บ่อย
ลักษณะอุจจาระ เป็นน้า,มูกหรือเลือด เป็นน้า
ปวดเหมือนถ่ายไม่สุด(tenesmus) พบได้ ไม่มี
ปวดมวนท้อง ท้องน้อย,อาจมีปวดลงก้น รอบสะดือ
3. แยกโดยใช้ลักษณะของอุจจาระว่าเป็น inflammatory หรือ non-inflammatory diarrhea ( ซึ่งอาจเป็นได้ทั้ง secretory, osmotic หรือ
fatty diarrhea)
Medicine: GI, 137
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
พยาธิใบไม้ในตับ : รับประทาน 10 mg/Kg เป็นเวลา 7 วัน
3. Thiabendazole พยาธิตัวกลมในลาไส้ชนิดต่างๆ : 25 mg/Kg วันละ 2 ครั้ง เป็นเวลา 2 วัน
4. Pyrantel pamoate พยาธิปากขอ พยาธิไส้เดือน พยาธิเข็มหมุด โดยขนาดที่ใช้ คือ 11 mg/Kg ครั้งเดียว
5. Piperazine พยาธิไส้เดือน และพยาธิเข็มหมุด โดยขนาดที่ใช้ คือ 75 mg/Kg วันละครั้ง ติดต่อกัน 2 วัน
6. Praziquantel
พยาธิใบไม้ : รับประทาน 20 mg/Kg โดยให้ 2-3 ครั้ง ห่างกัน 4 – 6 ชั่วโมง
พยาธิตัวตืด : รับประทาน 10 – 20 mg/Kg ครั้งเดียว
7. Niclosamide พยาธิตัวตืด โดยให้รับประทาน ครั้งเดียวในขนาด 2 กรัม
ยาพยาธิแบบน้า
Mebendazole แบบน้า
สาหรับเด็ก 2-15 ปี 1 tsp x 2
พยาธิตัวกลม ให้ 1 วัน ,พยาธิตัวแบน ให้สามวัน
สาหรับเด็ก 1-2 ปี 1/2 tsp x 2
พยาธิตัวกลม ให้ 1 วัน ,พยาธิตัวแบน ให้สามวัน
Albendazole แบบน้า
สาหรับเด็ก 1-2 ปี Alben 200 mg PO single dose
สาหรับเด็ก 2-15 ปี Alben 400 mg PO single dose
Irritable Bowel Syndrome
Clinical presentation
-Chronic gastrointestinal disorder of unknown cause.
-Common symptoms include abdominal cramping or pain, bloating and gassiness, and altered bowel habits
-Patient has comorbid psychiatric disorders [depression, anxiety]
-The hallmark of IBS is abdominal discomfort or pain. The following symptoms are also common
-The Rome III Criteria : a patient should have suffered abdominal pain or discomfort for 12 weeks or more (not
necessarily consecutive weeks) in the previous 12 months. The pain or discomfort should have two out of the
three following features:
138.
Medicine: GI, 138
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Relief with defecation
Onset associated with a change in the frequency of stool
Onset associated with a change in the form of stool
Differential diagnosis
-clinical diagnosis
-Ix to R/O other GI causes ex. CBC,TSH, Electrolyte, Stool
exam, Abdominal film, Barium enema, GI scope Supporting
symptoms
1) abnormal frequency of stools (more than 3/day or less than
3/week)
2) abnormal stool form (lumpy and hard, or loose and watery)
3) abnormal stool passage (straining, urgency, or feeling of
incomplete evacuation)
4) passage of mucus
5) bloating (feeling of abdominal distention, or enlargement).
Management
-Counseling: reassure Pt. เพื่อคลายความกังวลและให้ Pt มั่นใจว่าไม่ได้เป็นโรคร้ายแรง
-Dietary: fiber supplement [psyllium], avoid food that worsen symptoms eg.fat,bean,cabbage,clauliflower
-Medications:
1. Anti-diarrheal drug-> Loperamide[imodium] 4 mg (2 capsules) as a first dose, followed by 2 mg (1 capsule)
after each unformed stool. The maximum dose is 16 mg/day.
2. Anti-spasmodic drugs->
2.1 dicyclomine (Bemote, Bentyl, Di-Spaz) 20 mg given 2-4 times daily.
S/E:dry mouth, blurred vision, confusion, agitation, increased heart rate, heart palpitations, constipation, difficulty
urinating
2.2 hyoscyamine (Levsin, Levbid, NuLev)May be taken with or without food. The dosage is adjusted to the
individual patient to assure control of symptoms with a minimum of side effects.
S/E:dry eyes, dry mouth and urinary hesitancy and retention. Blurred vision, rapid heart rates, palpitations
3. Psychiatrics drug:
TCA->amitriptyline 10-25 mg po hs in divided doses. S/E:SIDE EFFECTS:fast heart rate, blurred vision, urinary
retention, dry mouth, constipation, weight gain or loss, and low blood pressure
139.
Medicine: GI, 139
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Liver Function Test
Lab Normal range Significance
Total Bilirubin 0.2 – 1.0 mg/dL 1. Prehepatic: IB , IB/TB > 80 – 85 %
2. Hepatic: IB & DB
3. Posthepatic: IB & DB
Direct Bilirubin 0 – 0.2 mg/dL
ALT (SGOT) 0 – 37 IU/L - found in liver
AST (SGPT) 5 – 40 IU/L - found in liver, skeletal m., heart, kidney, brain and RBC
Alk Phos 40 – 117 IU/L - found in liver, bone, gut, placenta
GGT 7 – 50 IU/L - found in canalicular membrane & microsomes
- confirm that Alk Phos is of hepatobiliary tract
- alcohol drinking, drugs
Albumin 3.5 – 5.5 g/dL - half-life 20 days, in chronic liver diseases
Globulin 1.5 – 3.5 g/dL - in cirrhosis
Analysis
1. Hepatocellular damage ALT, AST, Alk Phos, GGT
2. Excretory function TB, DB, Alk Phos
3. Synthetic function Albumin, PT, Cholesteral
Disorder Bilirubin Albumin PT AST, ALT Alk Phos
Hemolysis unconj AST
Acute hepatitis unconj, conj , > 500,
AST : ALT < 1
, < 3X
Chronic hepatitis unconj, conj / , < 300 , < 3X
Alcoholic hepatitis,
Cirrhosis
unconj, conj / , AST : ALT > 2
AST < 300
, < 3X
Cholestasis unconj, conj , , , 5 X 3 X
Infiltration 3 X
In ALT or AST in asymptomatic patient
a. Autoimmune hepatitis
b. HBV
c. HCV
d. Drugs or Toxin
e. Ethanol
f. Fatty liver
g. Growths (tumors)
h. Hemodynamic disorders (e.g., CHF)
i. Iron (hemochromatosis), copper (Wilson’s
disease), or AAT deficiency
References: Step Up to Medicine, Lecture Notes Clinical Pathology
140.
Medicine: GI, 140
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Acute viral hepatitis
Clinical presentation
Symptoms: Asymptomatic, Fatigue, Malaise, Jaundice, Fever
Muscle and joint aches
PE : jaundice tender hepatomegaly
Ix : LFT :( ALT>10 เท่าของUNL , AST>ALT ในช่วง 24-48ชม.แรก+/- direct hyperbilirubinemia)
Serology for Acute Viral Hepatitis
HAV: Anti HAV-IgM
HBV: HBsAg , Anti HBc-IgM (Anti HBs, Anti HBc, HBeAg : no benefit)
HCV: HCV RNA positive and anti HCV negative
Management
-Symptomatic and supportive
F/U LFT q 1-2 weeks
คาแนะนาเรื่องอาหาร -สามารถกินอาหารประเภทไขมันได้ถ้าคลื่นไส้อาเจียนไม่รุนแรง
-หลีกเลี่ยงการกินคาร์โบไฮเดรตที่มากเกินไป (เพราะ Impair free water clearance and
Induce fatty liver)
-Indication for admission
Severely symptomatic: marked nausea-vomiting encephalopathy
Lab -Rising bilirubin>15-20 mg/dL
-Persistence of bilirubin at plateau for 2-3 wks.
-Prolonged PTwith rapidly fall in AST/ALT
-Hypoglycemia
-Hepatocellular failure (drops in albumin, ascites)
HAV Prevention
Pre-exposure prophylaxis **ตัวอย่างชื่อการค้าของวัคซีนที่มีในไทย
อายุ 1-15 yr Havrix 360 (viral Ag >360 ELISA Unit) 0.5 ml IM (Day0,1,6 mo) --3 doses
อายุ 1-18 yr Havrix 720 (viral Ag >720 ELISA Unit) 0.5 ml IM(Day0,6 -12 mo) -- 2 doses
อายุ >19yr Havrix 1440(viral Ag>1,440 ELISA Unit) 1 ml IM (Day0,6 -12 mo) --2 doses
Post-exposure prophylaxis
Indication -household and sexual contacts of infected patients
-contacts in childcare centers during outbreaks
-patient is a food handler, others who work at the same establishment.
HAV Ig 0.02 mL/kg IM single dose (ภายใน 2 สัปดาห์) (80-90% effective)
141.
Medicine: GI, 141
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
HAV vaccine ครบ course
HBV Prevention
Preexposure prophylaxis **ตัวอย่างชื่อการค้าของวัคซีนที่มีในไทย
ENGERIX-B 3 doses (Day 0 , 30 , 180)
อายุ > 20 yr. (20/μg/1 ml) IM
อายุ < 20 yr (10μg/0.5ml) IM
EUVAX B 3 doses (Day 0 , 30 , 180)
อายุ >15 yr (20 μg /1 ml) IM
อายุ <15 yr. (10 μg /0.5 ml) IM
Postexposure prophylaxis
Direct exposure (percutaneous inoculation or transmucosal exposure) to HBsAg-positive body fluid (e.g.,
needlestick injury):
HBV Ig 0.06 mL/kg IM single dose (เร็วที่สุด)
HBV vaccine 3 doses (เริ่ม doseแรก ภายใน 7 days)
Direct exposure following sexual contact with an individual with HBV:
HBV Ig 0.06 mL/kg IM single dose ( ภายใน 14 days)
HBV vaccine 3 doses
แหล่งข้อมูล : Practice Guideline - Management of acute viral hepatitis ; World Gastroenterology Organisation, 2007
Chronic Hepatitis B Infection
Clinical presentation
Diagnostic criteria
HBsAg + > 6 months
การดาเนินโรค Chronic hepatitis Bแบ่งได้ 3 ระยะ
1. Immune tolerance phase พบในช่วงแรก ๆ ผู้ป่วยยังอายุน้อย ระดับ ALT จะเป็นปกติแต่ HBeAg positive และมีปริมาณ HBV
DNA ในเลือดสูง
2. Immune clearance phase เป็นระยะที่มีอาการอักเสบ บางรายอาจกาเริบรุนแรงซึ่งเกิดจากร่างกายพยายามกาจัดเชื้อไวรัสจนบางรายอาจ
เกิด hepatic decompensationได้
3. Residual phase เป็นระยะที่ตามมาโดยเกิดมี HBe seroconversion (HBeAg negative, Anti HBe positive) ร่วมกับการ
ทางานของตับเป็นปกติซึ่งบ่งชี้ถึงการเกิด remission
อย่างไรก็ตามยังมีผู้ป่วยจานวนหนึ่งที่พบการอักเสบของตับอยู่หลังจาก HBe seroconversion เนื่องจาก precore mutationทาให้ไม่
สามารถสร้าง HBeAgแต่ไวรัสยังคงแบ่งตัวตามปกติ ในผู้ป่วยกลุ่มนี้จึงต้องอาศัย HBV DNA Viral load ในการติดตามอาการ
142.
Medicine: GI, 142
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Diagnostic marker of HBV
Acute infection
Early HBs Ag +, anti-HBc +
Window IgM anti-HBc +
Recoverd Anti-HBs +, anti-HBc IgG +
Chronic infect on
Replicative HBsAg +, HBeAg +, HBV-DNA
Non/low replicative HBsAg +, HBe –, HBV-DNA
Precore mutant HBsAg +, HBe-, HBC-DNA
Management
ข้อบ่งชี้ในการรักษาและวิธีการรักษา
HBeAg Status HBV DNA
(IU/ml)
ALT
xULN
Potential first-line therapy
Posit ve >20,000 <= 2 Do not treat (low efficacy of current therapy)
Positive >20,000 >2 Treat with interferon, pegylated interferon,
adefovir(Hepsera), or entecavir (Baraclude), or
lamivudir or telbivudine
Negative >20,000 >2 Treat with interferon, pegylated interferon,
adefovir(Hepsera), or entecavir (Baraclude), or
lamivudir or telbivudine
Negative >20,000 1 to >2 Consider liver biopsy to help in treatment decision
Negative <=20,000 <=1 Observe
Positive or
negative
Approximat
ely >=10 to
100
Cirrhosis
with <= 1 to
>2
If liver function compensated with DNA > 2000 IU/ml,
treat with adefovir or entecavir or lamivudine or
telbivudine, if DNA < 2000 IU.ml, treat if the ALT level
is elevated ; if decompensated, treat with lamivudine
or telbivudine or adefovir. Or entecavir with liver-
transplantation center
Positive or
negative
Approximat
ely <10 to
100
Cirrhosis
with <= 1 to
>2
If compensated, observe; if decompensated, refer for
liver transplantation
แหล่งข้อมูล Guidelines are from the American Association for the Study of Liver Diseases (n engl j med 359;14
www.nejm.org) October 2, 2008
*หมายเหตุ บางสถาบันจะรายงานผลจานวนไวรัสเป็นจานวน copiesซึ่ง1 IU/ml = 5.6 copies/ml
Medicine: GI, 144
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
แนวทางการดูแลผู้ป่วยไวรัสตับอักเสบบี
HBeAg ,ALT
ALT<UNL
HBV<105
HBV>105
ALT<UNL
F/U 3 months
ALT >UNL
ALT < 2 UNL
F/U 6 months
F/U 1-2 months
ALT > 2 UNL
Concern of hepatic
decompensation
Yes
-F/U 3-6 months
-If ALT still > 2 UNL Liver Bx and treatment
-IFN ,Peg IFN, antiviral drug
No
Antiviral drug
monitoring
monitoring
HBeAg(--)
HBsAg(+) (exclude HCV,HDV)
HBeAg(+)
Reference
1. Hepatitis B Virus Infection , Jules L. Dienstag, M.D. ,N Engl J Med 2008;359:1486-500
2. แนวทางการดูแลรักษาผู้ป่วยไวรัสตับอักเสบบีและซีในประเทศไทย ปี 2548 , ชมรมโรคตับแห่งประเทศไทย , สมาคมแพทย์ระบบทางเดินอาหารแห่งประเทศ
ไทย
145.
Medicine: GI, 145
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Pyogenic Liver Abscess
History Clinical Presentation Investigation
Hematogenous spread or local
spread from infection within
peritoneal cavity: appendicitis,
diverticulitis, penetrating trauma. (
เชื้อ : E. coli, Klebsiella, Proteus,
Enterococcus, Anaerobes)
- non specific
- fever
- wt loss
- malaise
- nausea/vomiting
- 50% มี hepatomegaly ,RUQ
tender,janudice
- ALP , +/- abn.LFT
- CBC: Leukocytosis
- Round or oval defects on U/S, CT
scan , MRI
- CXR : อาจพบ new elevation of Rt.
hemidiaphragm,Rt. basilar
infiltration,Rt. pleural effusion
Management
- Empirical ATB: Cefoxitine (2g) IV q 4-6 hr.
- Percutaneous or surgical drainage
- Specific ATB depend on G/S and C/S
Amebic liver abscess
History Clinical Presentation Investigation
- Homosexual men
- ติดต่อทาง Fecal-oral hepatic
portal vein liver abscess
- non specific
- fever
- wt loss
- malaise
- nausea/vomiting
- hepatomegaly, RUQ
tenderness, diarrhea
- CBC : Leukocytosis
- LFT often elevate
- 90% positive serologic tests ( IgG
immunoassay)
- Round or oval defects on U/S , CT
scan , MRI (more commonly single)
- CXR : ~ pyogenic
U/S : Amoebic liver abscesses are usually single but can be multiple. Typical location is in the right lobe of liver
subcapsular close to the diaphragm and posterolateral, though it can be situated in any location. The size of an
abscess may vary from few centimeters to a large size occupying almost entire right lobe of liver
Picture1. Early abscess [1]. Picture2
146.
Medicine: GI, 146
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Sometimes the walls may be thicker and these may be seen as shaggy, ill-defined echogenic areas along the
walls (see Picture2). It is at this stage of the abscess that aspiration may be required. Small amount of air in the
abscess because of secondary infection or following an aspiration is seen as highly reflective dots.
Management
- Metronidazole (400 mg) PO tid for 5-10 days
- Percutaneous or surgical drainage
Cirrhosis
History Clinical Presentation Investigation
- cause :
- alcohol,
- chronic HBV,HCV,HDV
- autoimmune hepatitis, drug (eg.
methotrexate)
- metabolic disease :
hemochromatosis, Wilson’s
disease, alpha1-antitripsin
deficiency
- biliary tract disease
- vascular disease : Budd-Chiari
syndrome, Rt.sided heart failure,
constrictive pericarditis
- NAFLD,NASH
Liver failure : jaundice, spider nevi, palmar
erythema, Dupuytren’s contracture, white nail
line, parotid gland enlargement ,
gynecomastia, testicular atrophy, asterixis,
coagulopathy. encephalopathy
+/- signs of portal hypertension eg.
varices,ascites,splenomegaly, dilated
superficial vein(Caput medusae), epigastric
venous hum
PE : shrunken and nodular liver
- U/S upper abdomen
: liver size,
inhomogenous echo,
R/O HCC, ascites
- abnormal LFT
- Fibroscan
- liver biopsy
- AFP : screening HCC
- W/O หา cause eg.
hepatitis serology
etc.
Management
- Symptomatic treatment
- Treat complication eg.SBP,hepatic encephalopathy
- Liver transplantation ( Child-Pugh class B or C)
Measure 1 point 2 points 3 points Units
Bilirubin (total) <34 (<2) 34-50 (2-3) >50 (>3) µmol/l (mg/dl)
Serum albumin >35 28-35 <28 g/l
147.
Medicine: GI, 147
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
INR <1.7 1.71-2.20 > 2.20 no unit
Ascites None Suppressed with medication Refractory no unit
Hepatic encephalopathy None
Grade I-II (or suppressed with
medication)
Grade III-IV (or
refractory)
no unit
Points Class One year survival Two year survival
5-6 A 100% 85%
7-9 B 81% 57%
10-15 C 45% 35%
Hepatic Encephalopathy
Clinical presentation
A neuropsychiatric abnormalities in patients with liver dysfunction or portal hypertension.
neurotoxic substances (ammonia and manganese) chage morphology astrocytes.
characterized by personality changes, intellectual impairment, and a depressed level of consciousness.
3 types : A - associated with Acute liver failure.
B – associated with portal-systemic Bypass and no intrinsic hepatocellular disease
C – associated with Cirrhosis and portal hypertension or portal-systemic shunts
70% of patients with cirrhosis
Clinical features
Grading symptoms according to the West Haven classification
Grade 0 Minimal changes คนใกล้ชิดเท่านั้นที่detectได้
Grade 1 Reversal of sleep rhythm, psychomotor slowing, attention deficits, untidiness, irritability, สั่น
(asterixis) เล็กน้อย
Grade 2 Drownsiness, lethargy, disorientation, inappropriate behavior, slurred speech, obvious a terixis,
brisk reflexes
Grade 3 Somnolent แต่ปลุกตื่น (arousable), persistent disorientation, pronounced confusion, incoherent
speech, unable to perform mental tasks
Grade 4 Coma with(4a)or without(4b) response to painful stimuli
148.
Medicine: GI, 148
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Investigation เพื่อแยกสาเหตุอื่นออกไป
- Blood glucose
- Urea, BUN, Cr
- Electrolyte
- Avoid LP ยกเว้นคิดว่ามีสาเหตุจาก meningitis etc
Management
- Exclude nonhepatic causes eg. intracranial lesion or infection, hypoglecemia, electrolyte imbalance,
alcohol withdrawal, intoxication
- Correct precipitants metabolic, GI bleed, infection, constipation
- Avoid med that depress CNS esp benzodiazepines
- Severe case (gr 3 or 4) ET intubation ( at risk for aspiration)
Specific management
Restrict protein เริ่มด้วย 0.5-0.8 g/kg/d และค่อยๆเพิ่มทีละน้อย 0.25-0.50 g/kg/d q3-5d จนได้ปริมาณ
โปรตีนที่ต้องการ 1-1.5 g/kg/day
Lactulose เริ่มด้วย 30-45 g/d จนผป.ถ่ายได้เนื้อนิ่มวันละ 2-3 ครั้ง ในคนที่ใช้ lactulose ไม่ได้ผล ควร
พิจารณา short-term ATB ~1-2 wk
o Neomycin 2-4 g/d or
o Metromidazole 400 mg/d
Zinc 600 mg/d เฉพาะในราย chronic hepatic encephalopathy เท่านั้น
Ornithine ( L-ornitine-L-aspertage) 9-18 g/d
ทั้งหมด เป็นการรักษาเพื่อลด แอมโมเนียในร่างกายนะ
Flumazenil IV เฉพาะในรายที่ซึมจากการใช้ยา benzodiazepine
Medicine: GI, 151
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
- acetaminophen toxicity ควรแก้ไขโดย N-acetylcysteine
- mushroom poison แก้ไขโดย activated charcoal และ N-acetylcysteine
- การทา transjugular intrahepatic portosystemic shunt (TIPS) ใน acute Budd-Chiari syndrome
- การให้ acyclovir ใน herpesvirus infection
- Dialysis system ในผู้ป่วย HE ที่เกิดจากพิษของยา
2. การรักษาโดยใช้เครื่องมือต่างๆ เพื่อชะลอหรือหลีกเลี่ยงการผ่าตัดเปลี่ยนตับ เช่น
- Hepatic assist devices
- Axillary liver transplantation
- Liver dialysis system
- Xenotransplantation
3. Orthotropic liver transplantation เป็นวิธีการเดียวที่พิสูจน์ว่าเป็นวิธีการรักษาที่ดีที่สุดใน FHF ให้ผลอัตรารอด 1ปี ถึง80%
ข้อบ่งชี้ผู้ป่วยที่ผ่าตัดเปลี่ยนตับตาม King’s College Hospital
1. Acetaminophen – induced disease
Arterial pH < 7.3 (irrespective of the grade of encephalopathy) OR
Grade III or IV encephalopathy AND
Prothrombin time > 100 seconds AND
Serum creatinine > 3.4 mg/dl (301 μmol/L)
2. All other causes of fulminant hepatic failure
Prothombin time > 100 seconds (irrespective of the grade of encephalopathy)
OR
Any Three of the following variables (irrespective of grade of encephalopathy)
1. Age < 10 years or > 40 years
2. Etiology : non-A, non-B hepatitis, halothane hepatitis, idiosyncratic drug reaction
3. Duration of jaundice before onset of encephalopathy > 7 days
4. Prothombin time > 50 seconds
5. Serum bilirubin > 18 mg/dl (308 μmol/L)
2. การรักษาผลแทรกซ้อนที่เกิดขึ้นดังจะกล่าวต่อไป
Medicine: Nephrology, 170
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Magnesium and Phosphate
Electrolyte disturbance Symptoms and Signs Management
Hyperphosphatemia
PO4 > 4.5 mg /dL
Tetany , neuromuscular
irritability ,metastasic calcification
- low phosphate diet
- Phosphate binders เช่น aluminum hydroxide gel
orally
- In acute, severe case : Acetazolamide 15
mg/kg q4hr แล้วปรึกษาอายุรแพทย์ด่วน
+/- Hemodialysis
Hypophosphatemia
PO4 < 3.0 mg /dL
1. Mild: asymptomatic
2. Severe : Weakness , muscle
tenderness , cardiac and
respiratory failure, CNS
dysfunction
- severe(<1.0-1.5 mg/dl) ให้ Sodium phosphate 2
mg/kg IV over 6hr
- mild to moderate (>1.5 mg/dl) ให้ sodium
phosphate (Fleet’s Phospho-soda) 5 ml tid หรือ
potassium phosphate (K-Phos) 1-2 tab oral bid
Hypermagnesemia
Mg > 2.1 mEq/L
(Renal failure : most
common caused)
3-5 mEq/L : Nausea , vomiting ,
hypotension
7-10 mEq/L : Hyporeflexia ,
weakness , drowsiness
>12 mEq/L : Coma , bradycardia
, respiratory failure
- 10%calcium gluconate 10 ml over 10-20 min in
50-100 ml of D5W
- หยุดยาที่มีMg ex. MOM , antacid, MgSO4
- ถ้าไม่ดีขึ้นหรือเป็นโรคไตวาย คงต้องปรึกษาอายุรแพทย์ +/-
Dialysis
Hypomagnesemia
Mg < 1.5 mEq/L
Weakness , asterixis , vertigo ,
seizure, arrhythmia (prolonged Q, flat
T wave , Torsade de pointes)
ระวัง… Coexisting with
hypocalcemia and hypokalemia
- Seizure : 2g Magnesium sulfate in D5W IV over
10-20 min แล้วติดต่อผู้เชี่ยวชาญทันที
- ถ้าไม่มีอาการ ให้ Magnesiun oxide 1 g/d PO
171.
Medicine: Nephrology, 171
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Chronic Kidney Disease
Diagnostic criteria: one or more following condition lasting > 3 mo
1. GFR< 60ml/min/1.73 m2
2. Evidence of kidney damage eg. Proteinuria, hematuria, radiographic finding, pathological finding
Common cause: Diabetic nephropathy, Hypertensive nephropathy, GN, Drug-induced, myeloma, urinary tract
obstruction, PKD, acute renal failure, HIV
Hx : U/D (DM, HT), past UTI, Family Hx, fatigue, anorexia, N/V, metallic taste, pruritus, restless leg, bone
pain, impotence, infertility, dyspnea, urine output
PE: pallor, yellow skin pigmentation, brown nails, purpura, bruising, excoriation, hypertension, cardiomegaly,
pericardial rub, pleural effusion, pulmonary or peripheral edema, proximal myopathy Later if
untreated: arrhythmias, encephalopathy, seizures, and coma
Lab : Serum Cr, normochromic normocytic anemia, hyperkalemia, hyperphosphatemia, hypocalcemia,
metabolic acidosis, PTH (20
hyperparathyroidism), ALP (renal osteodystrophy)
U/S : เพื่อ R/O obstruction, ส่วนใหญ่พบไตขนาดเล็ก (< 9 cm) อาจพบไตขนาดปกติหรือใหญ่ขึ้นในโรค DM, ADPKD, amyloidosis,
myeloma, systemic sclerosis, asymmetric renal vascular disease)
Staging of CKD
CKD stage GFR (ml/min/1.73 m2
) Goals
1 ≥ 90 ลด CV risk (BP, LDL, สูบบุหรี่)
2 60-89 ติดตามการดาเนินโรค
3 30-59 ค้นหาและรักษาภาวะแทรกซ้อน (Hb, Ca, PO4,PTH)
4 15-29 เตรียม RRT เช่น เตรียมเส้นเลือด, ปรึกษาแพทย์โรคไต
172.
Medicine: Nephrology, 172
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
5 < 15 Renal replacement therapy (RRT)
Management
1. Lifestyle modification ออกกาลังกาย ไม่ดื่มสุรา ไม่สูบบุหรี่ หลีกเลี่ยง nephrotoxic agents เช่น NSAID,
aminoglycosides, radiocontrast agents, สมุนไพร
2. Diet control : low protein 0.6-0.8 g/kg/day และควรเป็น high biological value protein เช่น เนื้อสัตว์ ไข่ขาว low
salt < 2,300 mg/day เมื่อมี HT, edema low potassium หลีกเลี่ยงผัก ผลไม้ low phosphate หลีกเลี่ยง เมล็ดพืช
นม เนย กาแฟผง
3. Control BP < 130/80 mmHg : ACEI, ARB เป็น 1st
line drugs (ให้หยุดยากลุ่มนี้ถ้า SCr > 30% จาก
baseline หรือ serum K > 5.5 mmol/L) ยาอื่นๆที่สามารถใช้ได้คือ beta blockers, CCB, thiazide (CKD stage 1-
3), diuretics
4. Control plasma glucose HbA1c < 7.0% ควรใช้ insulin หลีกเลี่ยง Metformin เมื่อ SCr > 1.5 ในผู้ชาย > 1.4 ใน
ผู้หญิง Glibenclamide, Acarbose, Miglitol เมื่อ GFR < 30 Glipizide, Gliclazide เมื่อ GFR < 10
5. Control proteinuria ให้ ACEI, ARB ลด proteinuria ให้เหลือน้อยที่สุด
6. Control LDL cholesterol < 100 mg/dL โดยการคุมอาหาร และใช้ยากลุ่ม statins
7. Anemia Hb < 10 g/dL แยกสาเหตุอื่นออกไปก่อน จากนั้นประเมินว่าร่างกายมีปริมาณเหล็กเพียงพอ (serum
ferritin > 100 ng/mL และ TSAT > 20%) แล้วจึงให้ ESA 50-100 IU/kg/wk SC or 120-180 IU/kg/wk IV (goal Hb
11-12 g/dL)
8. Metabolic acidosis ให้ NaHCO3 เมื่อ HCO3 < 22 mmol/L
9. Edema restrict fluid intake, Furosemide 20-1000 mg/day
10.Control phosphate level < 4.6 mg/dL และ Ca x P < 55โดยการคุมอาหาร และให้ phosphate binders : Ca
acetate or CaCO3 (Tab 625 mg 1-2 tabs tid with meal,max 8 tab/day) หรือ Aluminium hydroxide
11.Control PTH level 100 -150 pg/mL in CKD stage III-V โดยให้ calcitriol PO 0.25 mcg/day increase dose by
0.25 mcg/day at 4-8 wk intervals, F/U serum Ca at least twice weekly during titration
12.Vaccine HBV ควรฉีดทุกคนถ้ายังไม่มีภูมิคุ้มกัน Influenza vaccine ควรฉีด CKD stage 4-5 ทุกปี
Consult nephrologists: 1. CKD stage 4 2. CKD stage 3 + GFR >7 ml/min/1.73m2
/year 3. Proteinuria > 1
gm or UPCR > 1000 mg/g เมื่อ control BP ได้ตามเป้ าหมายแล้ว
173.
Medicine: Nephrology, 173
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Nephrotic syndrome
หลักการวินิจฉัย ได้จากประวัติ ตรวจร่างกายและการตรวจทาง
ห้องปฏิบัติการแล้ว ต้องแยกให้ได้ว่าเป็น primary หรือ
secondary nephrotic syndrome ใน
secondary nephrotic syndrome ต้องรักษาต้นเหตุ
ด้วย
Urinary Tract Infection (UTI)
Lower vs Upper tract
Clinical แบ่งเป็น 2 ประเภทคือ
Uncomplicated UTI: ในผู้ป่วยที่ไม่มีความผิดปรกติทั้งโครงสร้างและหน้าที่ของ urinary tract อยู่เดิม
Complicated UTI: ในผู้ป่วยที่มีความผิดปรกติทั้งโครงสร้างและหน้าที่ของ urinary tract อยู่เดิม, มี immunosuppression เช่น DM, ติดเชื้อ
รักษายากเช่น Pseudomonas, Proteus (ESBL+)
Acute cystitis
History Physical Examination Investigation
- dysuria ,urgency, frequency
- suprapubic pain
- change in urine color/odor
- no fever or systemic toxicity
- suprapubic tenderness
- UA : pyuria, bacteriuria,
varying degree of hematuria
Management
Norfloxacin (400) 1x2 PO pc or Ofloxacin (200) 1x2 PO pc or Ciprofloxacin (250-500) 1x2 PO pc or
Co-trimoxazole (400/80) 2x2 PO pc for 3 days or Nitrofurantoin 100 mg PO bid for 5 dyas
Primary nephrotic syndrome
Primary nephrotic urine
Normal BP
Normal GFR
Nephrotic-nephritic urine
Hypertension
Decreased GFR
Age<1, >60 years
Likely steroid responsive
Trial of steroid Rx
Prednisolone 1mg/kg/day
(up to 60mg) for 2 wks
Response No response
Prednisolone 0.75 mg/kg/day
for 4-6 wks
No relapse relapse
Taper prednisolone over
6-12 months
Prednisolone 1 mg/kg/day
Till urine is protein free
Response No response
Frequent relapse steroid
dependence
Consider renal biopsy
12 wks
174.
Medicine: Nephrology, 174
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Acute pyelonephritis
History Physical Examination Investigation
- fever, shaking chills, flank pain
- urgerncy, frequency dysuria
- N/V, diarrhea
- Risk factor : bed ridden, on catheter
- fever, tachycardia
- CVA tenderness
- CBC : leukocytosis, left shift
- UA : pyuria, bacteriuria
- Urine C/S, H/C
Microbiology : E. coli (80%), Klebsiella, Proteus, Pseudomonas, Enterobacter
Management:
Mild (OPD case) : Ofloxacin (200) 2x2 PO pc or Ciprofloxacin (500) 1x2 PO pc for 7-14 days F/U 3 วัน ถ้าอาการไม่ดีขึ้นให้
admit เปลี่ยนเป็น IV ATB
Moderate to severe (high fever, systemic toxicity, unstable V/S, WBC > 15,000/mm3
) : admit, Ceftriaxone 2 gm IV ODor
Ampicillin 1 gm IV q 6 hr + Gentamicin 1 mg/kg IV q 8 hr for 14 days
หลังไข้ลง 24-48 hr ให้เปลี่ยนเป็น oral ATB ต่อจนครบ 14 วัน
ถ้าอาการไม่ดีขึ้นใน 48 hr ให้ตามผล C/S แล้วเปลี่ยน ATB ตาม sensitivity และอาจส่ง imaging (Film KUB, U/S) เพิ่มเติมตามความ
เหมาะสม
Admission order
One day Continue
1. Blood for CBC, BUN, Cr, Electrolyte
2. Urinalysis, MUC
3. NSS 1000 mlIV drip 80ml/hr (MT).
1. Record V/S, I/O q 4 hr
2. Ceftriaxone 2 g IV OD(or Ampicillin1g IV q 6 hr +
Gentamicin 1 mg/kg IV q 8 hr)
175.
Medicine: Neurology, 175
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
NEURO
Alteration of Consciousness
* Gaze preference (ในกรณีที่มี Destructive lesions)
“The eyes look toward a hemispheral lesion and away from a brainstem lesion”
Supratentorial lesion : “ตามองฟ้ อง lesion” (ตามองตรงข้ามกับข้างที่มี paralysis)
Infratentorial lesion : “ตามองตรงข้ามกับ lesion” (ตามองข้างเดียวกันกับ paralysis)
กรณี irritative lesion เช่น Focal encephalitis ตาจะมองตรงข้ามกับ lesion ใน Supratentorial lesion
176.
Medicine: Neurology, 176
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
** Brainstem reflexes ดูว่า Brainstem ระดับต่างๆ ยัง Intact ดีหรือไม่ (รายละเอียดต้องอ่านเพิ่มนะ)
1. Oculocephalic reflex (Doll’s eye): หากเสีย ตาจะไม่กลอกไปด้านตรงข้ามกับทิศที่หันศีรษะ ซึ่งแปลผลว่า Doll’s
eye negative คนปกติจะแปลผลว่า positive
2. Vestibuloocular reflex (Ice water caloric test): ปกติหากทา
caloric testโดยใช้น้าเย็นตาจะมี Nystagmus ที่มี slow phase
มาข้างนั้นและfast phase ไปด้านตรงข้าม หากเสียจะไม่
ตอบสนอง
3. Reflexes อื่นๆ เช่น Corneal reflex, Gag/cough reflex เป็นต้น
- กรณีจะ LP ใน Alteration of consciousnedd ให้ CT ก่อนเสมอ
- ในทางปฏิบัติกรณี BZD overdose จะไม่ให้ Flumazenil เพราะจะมี
ปัญหาหากผู้ป่วยมี Seizure จะไม่มียาใช้หยุดอาการชักได้
Clinical signs of increased intracranial pressure and brain herniation
- Increased ICP: Headache , nausea , vomiting, papilledema ,Cushing's triad (hypertension, bradycardia,
abnormal respiration)
- Uncal herniation: An ipsilateral 3rd
cranial nerve palsy (pupillary dilation) consciousness, hemiparesis
(contralateral first, later ipsilateral = Kernohan phenomenon)
- Central herniation: Progressive consciousness, Cheyne-Stokes then central hyperventilation,
midposition and nonreacitve pupils, decorticate/decerebrate/flaccid posturing
- Foraminal herniation or tonsillar herniation (downward forcing of the cerebellar tonsils into the foramen
magnum), which causes compression of the medulla, respiratory arrest, and death.
** กำรรักษำของ IICP และ brain herniation ดูได้ใน Sx part Neurosurgery
177.
Medicine: Neurology, 177
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Clinical clue ที่อาจช่วยบอกสาเหตุของ Alteration of consciousness
History
The circumstances , rapidity, antecedent symptoms (confusion, weakness, headache, fever, seizures,
dizziness, double vision, or vomiting) and Trauma.
The use of medications, illicit drugs, or alcohol
Chronic liver, kidney, lung, heart, or other medical disease
Breathing pattern
Kussmaul’s breathing: metabolic acidosis e.g. alcoholic ketoacidosis, DKA, lactic acidosis
Pupils
Dilated pupil : Mydriatrics use (atropine), CN III palsy, Transtentorial herniation
midposition & fixed pupils : Midbrain lesion
Small pupil: Opioid, Horner’s syndrome (involving sympathetic tracts), Early central Herniation
Asymmetrical finding : suggestive for structural lesion มากกว่า metabolic causes
Cutaneous petechiae : suggest thrombotic thrombocytopenic purpura, meningococcemia, or a bleeding
diathesis associated with an intracerebral hemorrhage.
Stroke
Acute management of stroke
1. AT Emergency Room
: A-B-C, observe V/S, GCS, pupil size, clinical sign of brain edema/herniation; O2 therapy
- Capillary blood glucose (keep 80-180; if >180 --- short-acting insulin)
- blood for CBC, BUN, Cr, Electrolytes, Coagulogram
178.
Medicine: Neurology, 178
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
- IV fluid = NSS (not hypotonic and without dextrose), Consult neurologist
- Rx ICP if present
2. History and Physical Exam, Esp.neuro exam in 15 min
- แยกภาวะ Stroke-mimicking เช่น hypoglycemia, postictal phase เป็นต้น
- ลักษณะทางคลินิกที่บ่งว่าน่าจะเป็น Hemorrhagic stroke : Intracerebral (consciousness , อาเจียน, ปวด
ศีรษะ, Progressive focal neuro deficit), subarachnoid (severe headache, meningismus)
3. Emergency CT brain without contrast, EKG
Hemorrhagic stroke (High morbidity/mortality)
Intracerebral hemorrhage
Admit ICU/Stroke unit
Control BP
SBP > 230 or DBP > 140 Nitroprusside 0.5 g/kg/min IV drip then dose + observe BP
SBP 180-230 or DBP 105-140
or mABP ≥ 130 mmHg
Labetalol 10–20 mg IV over 1–2 minutes, may repeat *1( not available in
Thailand)
Nicardipine start with 5 mg/hr, can add 2.5 mg/hr every 5 min (max rate: 15
mg/hr)
Enalapril IV 0.625 – 1.25 mg IV q 6 hr
If still uncontrollable, nitroprusside should be consider
SBP < 180 or DBP < 105 No acute treatment
179.
Medicine: Neurology, 179
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
ถ้าวัด ICP ได้ Keep Cerebral perfusion pressure > 70 mmHg
Correct coagulopathy, treatment of ICP
Antiepileptics prophylaxis for large area or lobar hemorrhage
Indications for surgical evacuation (consult NeuroSx)
- Cerebellar hemorrhage > 3 cm with clinical deterioration or brainstem compression
- Lobar clots within 1 cm of the surface
- Structural lesion (aneurysm, AVM)
- Young patients with large lobar hemorrhage and clinically deteriorating
- Ventriculostomy for massive intraventricular hemorrhage and obstructive hydrocephalus
MRI with contrast and MRA at 6 weeks
- To identify source of hemorrhage (esp. uncommon sites of bleeding or suspicious of tumor)
Subarachnoid hemorrhage
Admit ICU/Stroke unit, consult NeuroSx
Pain control, mild sedation (with caution, because GCS must be always observed)
Absolute bed rest
If negative on CT but clinically suspicious, LP to search for xanthochromia
- To identify ruptured aneurysm, CTA should be done
Control BP (as in intracerebral hemorrhage)
180.
Medicine: Neurology, 180
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Correct coagulopathy, treatment of ICP, seizure prophylaxis (phenytoin IV)
Specific treatment: obliteration of the aneurysm
- Surgical clipping
- Coil embolization
Ischemic stroke
Ischemic stroke
Admit ICU/Stroke unit ถ้าไม่พอ Admit เฉพาะ case ที่ให้ Thrombolytic หรือ brain swelling มาก ๆ
Indications for thrombolysis (Adult Stroke : AHA guideline 2010)
Fulfill all of these :
● Diagnosis of ischemic stroke causing measurable neurologic deficit (NIHSS 4 – 20)
● Onset of symptoms <3 or 4.5 hours before beginning treatment
● Age ≥ least 18 years
Absolute contraindications Relative contraindications
● Head trauma or prior stroke in previous 3 months
● Symptoms suggest subarachnoid hemorrhage
● Arterial puncture at noncompressible site in previous 7
days
● History of previous intracranial hemorrhage
● Only minor or rapidly improving stroke
symptoms
(clearing spontaneously)
● Seizure at onset with postictal residual
neurologic impairments
181.
Medicine: Neurology, 181
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
● Elevated blood pressure (systolic >185 mm Hg or
diastolic
>110 mm Hg)
● Evidence of active bleeding on examination
● Acute bleeding diathesis, including but not limited to
–Platelet count <100 000/mm3
–Heparin received within 48 hours, resulting in aPTT
>upper limit of
normal
–Current use of anticoagulant with INR >1.7 or PT >15
seconds
● Blood glucose concentration <50 mg/dL (2.7 mmol/L)
● CT demonstrates multilobar infarction (hypodensity >1/3
cerebral hemisphere)
● Major surgery or serious trauma within
previous 14 days
● Recent gastrointestinal or urinary tract
hemorrhage
(within previous 21 days)
● Recent acute myocardial infarction (within
previous 3 months)
ถ้าจะให้ rt-PA ในช่วง 3-4.5 ชั่วโมง ไม่ควรมีประวัติ อายุมากกว่า 80 ปี หรือ เป็นโรคเบาหวานร่วมกับโรคหลอดเลือดสมอง หรือ
ประวัติรับประทาง anticoagulant ไม่ว่า INR จะเท่าใดก็ตาม
If candidates for Thrombolysis
- Counseling, explain pts and family about risks and benefits
- Two IV peripheral access and Avoid CVP catheterization, except in emergency condition
- t-PA: total dose = 0.9 mg/kg (max 90 mg)
182.
Medicine: Neurology, 182
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
- divided : 10% of total dose --- IV bolus within 2-3 minutes
90% of total dose --- IV drip in 1 hr
- Observe V/S, bleeding and GCS q 15 min during administration
- Avoid urethral catheterization at least 2 hrs.
- Stop!!! when (1) neurological deterioration (2) serious bleeding found (3) difficulty breathing
- In case of bleeding : then Reimage brain emergently
Peripheral bleeding --- direct compression
Internal bleeding --- give cryoprecipitate and/or FFP and/or platelets
- After give t-PA, no antiplatelets or anticoagulants use within 24 hr
- Repeat head CT at 24 hr to R/O ICH
- Keep < 185/110 mmHg for 24 hr วัด BP q 15 min in 2 hrs then q 30 min in 6 hrs then q 1 hr อีก 16 hrs
BP สูงก่อนให้ยาละลายลิ่มเลือด
โดย SBP>185 or DBP>110
Labetalol 10-20mg v in 1-2 min can repeat ได้อีก 1 ครั้ง
Nicardipine v กรณียัง control BP ไม่ได้
BP สูงระหว่างให้ยา
- DBP > 140
- SBP > 180 or DBP 105-
140
Nitroprusside 0.5 mcg/kg/min
อาจให้ labetalol 10-20 mg v in 1-2 hrs ให้ซ้าได้ หือ double dose q 10 min (max
300mg)
หรือ labetalol v drip 2-8 mg/min
หรือ nicardipine 5 mg/hr titrate 2.5 mg/hr q 5 min (max 15 mg/hr)
183.
Medicine: Neurology, 183
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
ถ้าคุมไม่ได้พิจารณา nitroprusside
BP ต่า พบไม่บ่อย ต้องหาสาเหตุเช่น aortic dissection, volume depletion, MI,
Arrhythmia
- General management
If not candidates for Thrombolysis --- general management
General management
- Observe V/S, GCS
- Keep Temp < 37.5 o
C, avoid anti-HT unless BP > 220/120 (no aggressive treatment)
- If BP --- Nitropusside 0.3-10 g/kg/min IV drip or Nicardipine 2-10 g/kg/min IV drip
SBP ≤ 220 or DBP ≤ 120 Observe, Symptomatic treatment (Headache N/V etc)
SBP ≤ 220 or DBP 121 - 140 Labetalol 10 – 20 mg v in 1-2 min repeat or double dose q 10 min (max
300mg)
Nicardipine v 5 mg/hr titrate 2.5 mg/hr q 5 min (max 15 mg/hr)
DBP > 140 Nitroprusside v 0.5 g/kg/min
- Avoid sublingual CCBs, no hypotonic or dextrose IV fluid
- NPO if high risk for aspiration; GI prophylaxis with omeprazole 20-40 mg IV
- Prevent these complications : UTI, decubitus ulcer, contracture, depression, herniation***
- Aspirin 325 mg/day chewing, within 48 hr of onset (caution!! in candidate for thrombolysis) ให้ dose นี้10 – 28
184.
Medicine: Neurology, 184
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
วันแล้วเปลี่ยนเป็น dose ป้ องกัน
- No absolute indication for heparin use, may use in: AF, valve prothesis, Anterior wall MI with LV clots,
EF<20%, etc. --- start heparin 4-7 days after stroke and repeat CT before!!
- Don’t forget rehabilitation!!
Secondary prevention
1. Continue Aspirin 50-325 mg/day with GI prophylaxis
2. Treat vascular risk factors :
1) Hypertension target BP < 120/80 mmHg
- Lifestyle + anti-HT drugs (ACEIs, ARBs may be more beneficial) Start ยาหลังมีอาการแล้วอย่างน้อย 24 ชั่วโมง
2) DM goal : HbA1c < 7%
3) Dyslipidemia target LDL-C <100 mg/dl (<70 mg/dl in multiple risk factors)
- Simvastatin 5-10 mg PO hs (max 20 mg in the elderly, beware of side effects)
4) Weight reduction as possible
3. Stop alcohol, drug abuse and smoking
Stroke in the young
Stroke in the young หมายถึง Stroke ในคนอายุ < 45 ปีมักต้องหาสาเหตุเพิ่มเติมคือ lupus anticoagulant,
anticardiolipin antibody, homocysteine level, factor V Leiden, prothrombin 20210A, protein C, protein S,
antithrombin III, anti HIV, ANA, urine amphetamine เปนต้น
185.
Medicine: Neurology, 185
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
TIA
Transient ischemic attack เกิดจากสมองบางส่วนขาดเลือดไปเลี้ยงชั่วคราว และอาการทางระบบประสาทจะหาย
เป็นปกติ (นิยามเดิมตาม Clinical diagnosis)
AHA/ASA ให้นิยามใหม่ว่า TIA = ขาดเลือดชั่วคราวที่ทาให้สมอง ไขสันหลัง หรือจอประสาทตาทางานผิดปกติ
ชั่วคราวโดยไม่พบพยาธิสภาพจากการขาดเลือด (MRI ต้องปกติ)
Clinical : ระบบ carotid
- amaurosis fugax
- ipsilateral clumsiness
- ipsilateral paresthesia
- aphasia, dysarthria
- contralateral homonymous hemianopia
Clinical : ระบบ vertebrobasilar
- อ่อนแรงหรือใช้งานไม่ถนัดทั้ง 2 ข้าง
- ชาหรือความรู้สึกสัมผัสเพี้ยนทั้ง 2 ข้าง
- ตาบอดครึ่งซีกด้านตรงข้ามหรือทั้ง 2 ข้าง
- ร่วมกับอาการอย่างน้อยดังต่อไปนี้ได้แก่ เวียนหัว เห็น
ภาพซ้อน กลืนลาบาก dysarthria, ataxia
TIA เป็นอาการนาของ Stroke 25-50 % โดยมีการใช้ ABCD2 score ทานายโอกาสเกิด Stroke ตามมาโดย
A: Age ≥ 60 ปี (1 คะแนน) B: BP ≥ 140/90 (1 คะแนน)
C: Clinical (แขนและขาอ่อนแรง 2, Speech impairment โดยไม่อ่อนแรง 1)
D: Duration (≥ 60 min 2,10-59 min 1) D: DM (1 คะแนน)
คะแนนรวม 0-1 2-day risk of stroke 0% คะแนนรวม 2-3,4-5,6-7 ความเสี่ยงจะร้อยละ 1.3, 4.1, และ 8.1 ตามลาดับ
ถ้าคะแนน ≥ 3 ให้ Admit
การรักษา
For patients with TIA or ischemic stroke of atherothrombotic, lacunar (small vessel occlusive), or
cryptogenic type, we recommend treatment with an antiplatelet agent (Grade 1A) ให้หาสาเหตุและ secondary
prevention แบบเดียวกับ ischemic stroke
Medicine: Neurology, 195
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
2. ส่งตรวจ CT scan หากมี indication ดังต่อไปนี้:
Immunocompromised state = HIV, receiving immunosuppressive therapy, or after transplantation
History of CNS disease = Mass lesion, stroke, or focal infection
New onset seizure =Within 1 week of presentation; some authorities would not perform a lumbar
puncture on patients with prolonged seizures or would delay lumbar puncture for 30min in patients
with short, convulsive seizures
Papilledema
Abnormal level of consciousness …
Focal neurologic deficit = dilated nonreactive pupil, abnormalities of ocular motility, abnormal visual
fields, gaze palsy, arm or leg drift
- ถ้ามีลักษณะดังกล่าว ให้ take H/C, start dexamethasone (ดูข้อ 4) and empirical antibiotic แล้วส่งผู้ป่วยไป CT
- หากผล CT ไม่มี mass effect ให้ทา lumbar puncture ได้ (ดูข้อ 3)
3. หากไม่มี indication ดังในข้อ 2 แล้ว
- ให้เจาะเลือดเพื่อส่ง CBC, serum glucose, +/- Hemoculture, etc.
- ทา lumbar puncture, อธิบาย+เตรียมผู้ป่วย; LP วัด open & closed pressure, ดูความขุ่นของ CSF [หาก open
pressure > 25 cmH2O = High-risk for herniation; Start mannitol then consult neurosurgery]
- ส่ง CSF เพื่อตรวจ (1) C/S, G/S (2) glucose, protein (3) cell count & diff (4) เก็บไว้ตรวจ Gram stain เอง (5) หรือ
ตรวจเพิ่มพิเศษทางห้องปฏิบัติการอื่นๆ
- ย้อม Gram stain เอง หากพบเชื้อให้พิจารณาร่วมกับประวัติ ว่านึกถึงเชื้อใดมากที่สุด และให้ specific antibiotic แต่
หากไม่พบเชื้อ ให้ start empirical antibiotic แล้วคอยติดตามผลเพาะเชื้อ
4. การให้ dexamethasone อาจช่วย improve outcome & survival rate โดยเฉพาะใน community-acquired bacterial
meningitis
- Dose: 0.15 mg/kg หรือ 10 mg IV q 6 hr x 4 days ให้ในช่วง 10-20 นาทีก่อนให้ antibiotic หรือพร้อม antibiotic
(เน้นโดยเฉพาะ dose แรก หากให้หลังจากนี้อาจจะไม่มีประโยชน์)
196.
Medicine: Neurology, 196
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
5. Empirical antibiotic พิจารณาตาม Host factor และประวัติ
Clinical scenario Empirical ATB treatment
Normal adults (Ceftriaxone 2 g q 12 h or Cefotaxime 2 g q 6 h)
plus Vancomycin 15-20 mg/kg (1 g) IV drip q 12 h*
Head injury/Post-neuroSx Ceftazidime 2 g IV q 8 h + Vancomycin 1 g IV drip q 12 h
Elderly/Immunocompromised Ceftazidime 2 g IV q 8 h + Vancomycin (adjusted dose) + Ampicillin 2
g IV q 4 h
* Vancomycin ให้ในกรณีที่พบเชื้อ penicillin resistance S.pneumoniae ใน community แถบนั้นมาก
** Postexposure-prophylaxis in close contacts of patient with meningococcemia : Ceftriaxone 250mg IM
single dose or
Rifampicin 600 mg PO bid x 2 days or Ciprofloxacin 500 mg PO single dose
6. Specific ATB (ปรับยาตามผลเพาะเชื้อและความไวด้วย)
Organisms Antimicrobials Dose/Interval
S. pneumoniae PLUS Ceftriaxone
- Cefotaxime
- Cefepime
2 g q 12 h
2 g q 6 h
2 g q 8 h
Vancomycin 15mg/kg q 6-12 h
N. meningitides penicillin sensitive PGS 3-4 mU q 4 h
197.
Medicine: Neurology, 197
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
- Ampicillin 2 g q 4 h
penicillin resistant Ceftriaxone
- Cefotaxime
Gram neg rod, H. influenzae 3rd Gen Cephalosporin
P. aeruginosa Ceftazidime 3 g q 8 h
S. aureus (MSSA) Oxacillin 1.5-2 g q 4 h
S. aureus (MRSA), Staph coagulase negative Vancomycin 1 g q 12 h
L. monocytogenes Ampicillin 2 g q 4 h
Bacteroides, Fusobacterium Metronidazole 0.5 g q 6 h
S. agalaciae PGS, Ampicillin
เชื้อ N. meningitides ให้ ATB 7 วัน H. influenza ให้ 7 วัน S. pneumonia ให้ 10 -14 วัน gram negative 14 – 21 วัน
L.monocytogenes 21 วันขึ้นไป
7. ติดตามผล CSF Profiles เพื่อยืนยันการวินิจฉัยด้วย
Condition Appearance
Pressure
(cm H2O)
WBC
(/mm3
)
Glucose
(mg/dl)
Protein
(mg/dl)
Normal Clear 9-18 0-5 Mononuclear 50-75 15-40
Bacterial Cloudy 18-30 100-10,000 PMN
<45
(<50% of BG)
100-1,000
TB Cloudy 18-30 <500 Mononuclear 100-200
Fungal Cloudy 18-30 <300 Mononuclear 40-300
198.
Medicine: Neurology, 198
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Aseptic (mostly
viral)
Clear 9-18 <300 PMN Mono 50-100 50-100
BG= blood glucose ในขณะที่ทา lumbar puncture
สาหรับ Viral meningitis หากมีอาการไข้ URI symptoms นามาก่อนอาจจะช่วยสนับสนุนการวินิจฉัย และหากพบว่าซึม
มาก มีพฤติกรรมเปลี่ยนแปลง มีอาการชักให้คิดถึง Viral encephalitis และในกรณีที่มีอาการทางคลินิก(มีfocal
neurological deficit, ชัก หรือซึมมาก)หรือมี vesicle ที่เข้าได้กับ herpes infection อาจพิจารณาให้ Acyclovir 10
mg/kg IV drip in 1 hr q 8 hr 14 วันเพื่อรักษา herpes simplex encephalitis
กรณีที่มีอาการอยู่นาน หรือรักษาแบบ bacterial ที่เหมาะสมแล้วยังไม่ดีขึ้น ต้องคิดถึงภาวะ fungal/TB meningitis หรือ
Pathogen อื่นๆ รวมถึง paraminingeal infection เช่น subdural empyema, brain abscess ด้วย
Aseptic Meningitis
Definition Etiologies
Negative bacterial
microbiologic data
Aseptic = less likely to be
bacterial, but can be
infectious or noninfectious
(aseptic meningitis can be
neutrophilic, though less
common)
• Viral: Enteroviruses(most common),HIV, HSV(type2>1), VZV,mumps,
lymphocytic horiomeningitis virus, Encephalitis viruses, adenovirus, polio,
CMV, EBV
• Parameningeal focus of infection (eg, brain abscess, epidural abscess,
septic thrombophlebitis of dural venous sinuses, or subdural empyema)
• TB, fungal, spirochetal (Lyme, syphilis, leptospirosis), Rickettsial, Coxiella,
Ehrlichia
• Partially treated bacterial meningitis
• Medications: TMP/SMX, NSAIDs, IVIg and antilymphocyte globulins,
penicillin, isoniazid
• Systemic illness: SLE, sarcoidosis, Behçet’s, Sjögren’s syndrome,
199.
Medicine: Neurology, 199
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
rheumatoid arthritis
• Neoplasms: intracranial tumors (or cysts), lymphomatous or carcinomatous
meningitis(CSF cytology or flow may be reactive and diagnosis may require
meningeal biopsy)
Management
• No Antibiotics if suspect viral (cell count <500 w/ >50% lymphs, TP <80–100 mg/dL, normal glc, neg Gram
stain, not elderly/immunosupp.)
• Treat underlying cause.
• Microbacterial : Antimycobacterial treatment plus dexamethasone
• Fungal: amphotericin B or lipid formulation, ± 5-fluorouracil
Viral Encephalitis
Definition : Viral infection of the brain parenchyma with evidence of neurologic dysfunction
Clinical manifestations
• Fever, HA, Altered MS,± seizures and focal neurological findings
Investigation
• LP: lymphocytic pleocytosis; PCR for HSV (95% Se & Sp at 2–3 d),VZV,CMV, EBV, HIV, JC,
adeno/enterovirus,
• MRI (CT if MRI unavailable); HSV-1: temporal lobe lesions/edema
• EEG (to R/O seizure; findings in encephalitis are non-specific)
200.
Medicine: Neurology, 200
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
• Dilated retinal exam
• Serologies; vaccine history, ELISA of nasal or respiratory swabs for respiratory viruses
Management
• HSV, VZV: Acyclovir 10 mg/kg IV q8h
• CMV: Ganciclovir ±Foscarnet; supportive care for most other etiologies
Parkinson’s disease
Parkinsonism: The syndrome of parkinsonism, based on clinical features of tremor at rest, bradykinesia,
rigidity, flexed posture, loss of postural, and freezing of gait
2011, Fahn, Jankovic, Hallett classification of parkinsonism
Primary
Secondary: infections, toxins, drugs, tumor, trauma, vascular, metabolic
Parkinsonism-plus syndromes: MSA, PSP, corticobasal degeneration, Parkinsonism with dementia
Heredodegenerative disorder
Benign parkinsonism: dopa-responsive dystonia (DRD)
Parkinson’s disease is a progressive, neurodegenerative disorder that is characterized by severe motor
symptoms, including uncontrollable tremor, postural imbalance, slowness of movement and rigidity.
Clinical features of PD
Cardinal Features Other Motor Features Non motor Features
Bradykinesia
Rest tremor
Micrographia
Masked facies
Anosmia
Sensory disturbances (e.g., pain)
201.
Medicine: Neurology, 201
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Rigidity
Gait disturbance/postural instability
(hypomimia)equalize
Reduced eye blink
Soft voice (hypophonia)
Dysphagia
Freezing
Mood disorders (e.g., depression)
Sleep disturbances
Autonomic disturbances
Orthostatic hypotension
Gastrointestinal disturbances
Genitourinal disturbances
Sexual dysfunction
Cognitive impairment/Dementia
UK PDS Brain Bank Criteria for the diagnosis of PD
Step 1: Diagnosis of a parkinsonian syndrome
Bradykinesia (slowness of initiation of voluntary movement with progressive reduction in speed and
amplitude of repetitive actions) and at least one of the following:
(i) muscular rigidity,
(ii) 4–6 Hz rest tremor
(iii) postural instability not caused by primary visual, vestibular, cerebellar or proprioceptive dysfunction
Step 2: Exclusion criteria for PD
(i) History of repeated strokes with stepwise
Step 3: Supportive criteria for PD (three or
more required for diagnosis of definite PD)
202.
Medicine: Neurology, 202
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
progression of parkinsonian features
(ii) History of repeated head injury
(iii) History of definite encephalitis
(iv) Oculogyric crises
(v) Neuroleptic treatment at the onset of symptoms
(vi) More than one affected relative
(vii) Sustained remission
(viii) Strictly unilateral features after 3 years
(ix) Supranuclear gaze palsy
(x) Cerebellar signs
(xi) Early severe autonomic involvement
(xii) Early severe dementia with disturbances of
memory, language and praxis
(xiii) Babinski’s sign
(xiv) Presence of cerebral tumour or communicating
hydrocephalus on CT scan
(xv) Negative response to large doses of levodopa (if
malabsorption excluded
(i) Unilateral onset
(ii) Rest tremor present
(iii) Progressive disorder
(iv) Persistent asymmetry affecting side of
onset most
(v) Excellent response (70–100%) to
levodopa
(vi) Severe levodopa-induced chorea
(vii) Levodopa response for 5 years or
more
(viii) Clinical course of 10 years or more
Medicine: Neurology, 210
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Abortive
Oxygen 7 LPM for 15 minutes via face mask
Sumatriptan, NSAIDS
Prophylaxis
Verapamil 120 to 160 mg two to three times per day
อาการปวดหัวอย่าลืมดูด้วยว่าเกิดจาการใช้ยาแก้ปวดเกินด้วยหรือไม่ เพราะถ้าใช่การรักษาจะต้องลดและหยุดยา
ไม่ใช่ให้ยาแก้ปวดเพิ่มไปอีก
Approach to Peripheral Neuropathy
Clinical manifestations
• Weakness, fasciculations, numbness, dysesthesias (burning/tingling)
• ± Autonomic dysfunction (orthostasis, bowel/bladder retention/incontinence, impotence)
• Depressed or absent DTRs (may be normal in small fiber neuropathy)
Etiologies
• Mononeuropathy (one nerve): entrapment, compression, trauma, DM, Lyme
• Mononeuropathy multiplex ปัจจุบันจะเรียกว่า multiple mononeuropathy (axonal loss of multiple, separate,
noncontiguous nerves):
DM, vasculitides, sarcoid, , Lyme, Sjögren
• Polyneuropathy (multiple symmetric nerves, generally length dependent)
Demyelinating
211.
Medicine: Neurology, 211
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
acute: acute inflammatory demyelinating polyneuropathy (AIDP) = Guillain-Barré
subacute: meds (paclitaxel), paraneoplastic
chronic: DM, CIDP, hypothyroidism, toxins, paraproteinemia, hereditary
Axonal
acute: porphyria, vasculitis, uremia
subacute: meds (cisplatin, paclitaxel, vincristine, INH), EtOH, sepsis, paraneoplastic
chronic: DM, uremia, lead, arsenic, Lyme, HIV, paraproteinemia, B12 defic
Investigation
• Distal symmetric polyneuropathy: start with glc or HbA1C, B12
• Electrolytes, BUN/Cr, CBC,TSH, LFTs, ANA, ESR, HIV and heavy metal screening as indicated by clinical
history and exam
• EMG & NCS (often no change in first 10–14 d or in small fiber neuropathy)
• Autonomic testing / skin biopsy(polyneuropathy), nerve biopsy (mononeuropathy multiplex)
• MRI if possible radiculopathy or plexopathy
GUILLAIN-BARRÉ Syndrome (GBS)
Definition and epidemiology
• Acute inflammatory demyelinating polyradiculoneuropathy (AIDP)
• Incidence 1–2 per 100,000; most common acute / subacute paralysis
Clinical manifestations Investigation
• Precipitants: viral illness (EBV, CMV, HSV, HIV), URI (Mycoplasma), (ผลตรวจอาจปกติในช่วงวันแรกๆ)
212.
Medicine: Neurology, 212
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
gastroenteritis(Campylobacter), surgery, immunizations 1-3 wk prior.
• Sensory dysesthesias & numbness มักเป็นอาการแรก, back pain ก็
เป็นอาการที่พบบ่อย
• Ascending symmetrical paralysis over hours to days
• Hypoactive then Absent reflexes
• Respiratory failure 30%;autonomic instability & arrhythmias 50%
• Fisher variant: ophthalmoplegia, ataxia, areflexia; associated with
anti-GQ1b antibodies
• LP: albuminocytologic dissociation =
protein without pleocytosis (<20
lymphs)
• EMG & NCS: decrease nerve
conduction velocity and conduction block
• FVC & NIF: to assess for risk of
respiratory failure
Management
• Plasma exchange or IVIg (no additional benefit with both)
Plasmapheresis: Five exchanges (40-50 mL/kg) qod
Risks: Bleeding, infection, hematoma formation, C/I : sepsis, active bleeding, cardiovascular instability.
IVIg: 0.4 /kg/day daily × 5 days. Check IgA level prior to administering IVIg.
ให้ acetaminophen & diphenhydramine ก่อนให้แต่ละครั้ง
Risks: headaches, myalgias, arthralgias, flu-like , fever, & vasomotor reactions. Serious
complications(rare): anaphylaxis in IgA deficient pts, aseptic meningitis, CHF, stroke, MI, renal failure.
C/I: hyperviscosity, CHF, CRF, congenital IgA deficiency.
IVIg และ plasmapheresis ช่วยให้การฟื้นตัวเร็วเท่านั้น ผลความพิการในระยะยาวพบว่าไม่ได้ดีขึ้น
• Supportive care with monitoring in ICU setting if rapid progression or respiratory failure
( Intubate if FVC < 15 cc/kg or 1 L & NIF < 20 or rapid decline. If intubation >2 wk, consider tracheostomy)
213.
Medicine: Neurology, 213
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
• Watch for autonomic dysfunction: labile BP, dysrhythmias (telemetry) and SIADH
ห้ามใช้ steroid รักษา
Myasthenia Gravis
Definition and epidemiology
• Autoimmune disorder with Ab directed against acetylcholine receptor (AChR) in NMJ
• Prevalence: 1 in 7,500; affects all ages, peak incidence 20s–30s (women), 60s–70s (men)
Clinical manifestations Investigation
• Fluctuating weakness with fatigability (อาการแย่ลงเมื่อใช้งาน
ซ้าๆ และดีขึ้นเมื่อพัก)
• Cranial muscles involved early with ocular (ptosis, diplopia)
in 50%; bulbar (difficulty chewing, dysarthria, dysphagia) in
15%. Often later progresses to generalized weakness.
• Limb weakness proximal > distal; DTRs preserved; minimal
/ no atrophy
• Exacerbations triggered by stressors (such as URI,
,stress/surgery/trauma), botox administration, pregnancy or
postpartum, drugs (eg, aminoglycosides,
procainamide,phenytoin) ; prednisone can worsen acutely
• Bedside: ptosis after 30 seconds of
sustained upgaze, improved with ice pack
over eyes
• Neostigmine test: temporary strength;
false positive & negative occur; premedicate
with atropine
• EMG: decrease response with repetitive
nerve stimulation
• Anti-AChR Ab
• CT or MRI of thorax to evaluate thymus
(65% hyperplasia, 10% thymoma)
Management
• Anticholinesterase medications (eg, Pyridostigmine(60mg 180mg controlled release) 30-60 mg q 4-8 hr)
214.
Medicine: Neurology, 214
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
• Thymectomy if thymoma; may lead to improvement in up to 85% Pts without thymoma แนะนาทาใน
Generalized MG โดยเฉพาะผู้ป่วยที่เริ่มมีอาการ < 60 ปีทุกราย
• Immunosuppression: prednisone(start 1-2mg/kg/d จนดีขึ้นแล้วรวบ dose แล้วค่อย ๆ ลด dose ±azathioprine,
cyclophosphamide
• Myasthenic crisis: treat precipitant
Consider hold anticholinesterase if suspect cholinergic crisis if not suspected give Neostigmine 0.5
mg IV push, followed by pyridostigmine 24 mg in 500 mL D5 1/2 NS.
aggressive immunosuppression with glucocorticoids (methylprednisolone 60 mg IV daily) but watch
for initial worsening
IVIg : 2 g/kg infused in divided doses over 2-5 days & repeat the dose 6 h later if necessary
Plasmapheresis remove 2-3 L 3× /wk until improvement, usually five to six exchanges
ICU if rapid or severe (follow FVC, NIF) and Intubate for FVC < 15 mL/kg & NIF < -20 or rapid
respiratorydecline
** Myasthenic crisis = exacerbation with need for respiratory assistance
** Cholinergic crisis = weakness due to overtreatment with anticholinesterase medications;may have
excessive salivation, abdominal cramping, and diarrhea; rare at normal doses
Approach to Muscular diseases
Etiologies
• Hereditary: Duchenne, Becker, limb-girdle, myotonic, metabolic, mitochondrial
• Endocrine: hypothyroidism, hyperparathyroidism, Cushing syndrome
• Toxic: statins, fibrates, glucocorticoids (critical illness myopathy), zidovudine, alcohol,cocaine, antimalarials,
colchicine, penicillamine
215.
Medicine: Neurology, 215
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
• Infectious: HIV, HTLV-1, trichinosis, toxoplasmosis
• Inflammatory : polymyositis, dermatomyositis, inclusion body myositis
Clinical manifestations
• Progressive or episodic weakness (not fatigue)
• Weakness most often symmetric, proximal > distal (stairs, rising from sitting, etc.)
• ± Myalgias (though not prominent or frequent)
• May develop either pseudohypertrophy (dystrophies) or mild muscle atrophy
Investigation
• CK, aldolase, LDH, electrolytes,ALT/AST, PTH,TSH, ESR, HIV
• Autoantibodies (anti-Jo1, antisynthetase, anti-Mi-2, anti-SRP,ANA, RF)
• EMG/NCS: low-amplitude, polyphasic units with early recruitment, ±fibrillation potentials
• Muscle biopsy, molecular genetic testing (where indicated)
Hiccup
ภาวะสะอึกเป็นภาวะที่พบได้บ่อย โดยส่วนใหญ่เกิดแบบชั่วคราว แต่กรณีถ้าเป็นแบบ Persistant (>48 hours) หรือ
Intractable(> 2 months) ซึ่งมีผลต่อการดารงชีวิต นอนไม่หลับ หรือทาให้เกิด Wound dehiscence ได้ จาเป็นต้องได้รับ
การรักษาและหาสาเหตุต่อไป
ภาวะสะอึกเกิดจากการหดตัวของ diaphragm and the inspiratory intercostal muscles ทาให้หยุดชะงักการหายใจเข้า
ทันที และ closure of the glottis
Benign hiccup bout Persistent and intractable hiccups
Gastric distention from overeating, Vagus and phrenic nerve irritation
216.
Medicine: Neurology, 216
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
carbonated beverages, aerophagia,
and gastric insufflation during
endoscopy
Sudden changes in ambient or
gastrointestinal temperature
Excessive alcohol ingestion,smoking
Sudden excitement or other emotional
stress
• มี FB สัมผัสกับ tympanic membrane
• Pharyngitis, laryngitis, or tumors of the neck
• Goiters, tumors, or cysts in the neck, mediastinal masses,
and abnormalities of the diaphragm ( hiatal hernia, GERD,
diaphragmatic eventration)
Central nervous system disorders
Brainstem mass lesions, multiple sclerosis, hydrocephalus,
syringomyelia. Vascular and infectious causes are more
common.
Toxic-metabolic or drug-related disorders uremia, alcohol
intoxication, and general anesthesia.
Psychogenic factor anxiety, stress, excitement, malingering
Evaluation
History : the severity and duration of hiccups,surgical and medical conditions, alcohol and drug use.
PE : the head and neck, chest, abdomen, and neurologic function.
Laboratory: CBC(infection or malignancy), Cr and electrolytes, CXR(mediastinal abnormalities)
±as clinical indication LFT, serum calcium, EKG,MRI head, CT chest, LP, endoscopy, esophageal
manometry, pulmonary function tests, bronchoscopy, and EEG.
Management
Brief hiccup bouts do not require medical intervention
Nonpharmacologic : ให้กระทาบางอย่างซึ่งเป็นการรบกวน vagal afferent limb ของ hiccup reflex arc มีหลายวิธีเช่น
217.
Medicine: Neurology, 217
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Breathing into bag
Drinking from opposite side of glass
Ice water gargles
Biting on a lemon
Valsalva maneuver
Breath holding
Fright
Noxious odors (inhaling am onia)
Medication
Chlorpromazine เป็นยาที่นิยมใช้ใน persistent hiccups ให้ 25-50 mg PO tid-qid x 7-10 วัน
Metoclopramide, เป็น second drug of choice ให้ 10 mg PO tid-qid
Baclofen เป็นอีกยาหนึ่งที่ใช้ใน idiopathic intractable hiccups
Anticonvulsants (eg, phenytoin, valproic acid, gabapentin , and carbamazepine),
Antidepressants (eg, amitriptyline)
Central nervous system stimulants
Antiarrhythmic drugs (eg, quinidine)
Treatment for refractory hiccups
Hypnosis and acupuncture may be tried.
Surgical approaches, including phrenic nerve crushing or blocking with a local anesthetic
Common Pitfall In Neurology
อาการปวดศีรษะ ต้องพิจารณา “ red flags” หรือ ปวดหัวเรื้อรังรักษาไม่หาย ควรระวัง organic cause
อาการเวียนศีรษะ มึน กลืนติดคอที่รักษาไม่หายต้องระวัง Posterior circulation เพราะมักไม่มี weakness ให้เห็น
Dementia, Behavioral change ในระยะเวลาสัปดาห์ – เดือนต้อง rule out organic cause เสมอ
อย่าลืมถามเรื่องการใช้ยาประจาทุกครั้ง โดยเฉพาะคนแก่ที่กินยาหลายตัวเช่น ยากลุ่ม nitrate ทาให้ปวศีรษะได้
รุนแรงเนื่องจากเป็น venodilator, หรือ anticoagulant เป็น risk ของ bleeding
Neurological diseases ที่เกิดในวัย sexual active ในยุคปัจจุบันให้คิดถึง AIDS ไว้เพราะCNS infections คือ
Cryptococcal meningitis และ Cerebral toxoplasmosis abscess ซึ่งทาให้เกิด Increase intracranial pressure
จึงทาให้ปวดหัวมากได้เช่นกัน
218.
Medicine: Endocrinology, 218
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
ONCO – HEMATO
SVC Obstruction
not an emergency unless there is tracheal compression
History Physical examination Investigation
Causes
Malignant tumor
(common) : Lung
cancer, Lymphoma
Nonmalignant (rare)
: Thrombosis, Goiter,
Aortic aneurysm
- Distended neck vein
- Isolated upper limbs edema, periorbital
and facial edema with flushing
- Pulmonary manifestations : dyspnea,
tachypnea, cough, crackles, rales
- More severe symptoms in recumbent
position or after sleeping
- Prominent chest wall collateral vein (in
slow growing tumor)
- Sequelae of increased intracranial
pressure (less common)
- Special test : Pemberton’s test
Lift the arms over the head for >1 min
Observe : elevated JVP, increased facial
cyanosis/plethora, inspiratory stridor
- Investigations :
CXR : Pleural effusion (aspiration :
transudate pleural effusion)mass,
widening mediastinum
CT chest with contrast (Test of choice) or
MRI (if C/I for contrast)
Managements :
Initial management : symptomatic treatment
- ABCs, O2 therapy and head elevation 30 – 45 degree
- Dexamethasone 4 mg/6 hr : for increase ICP and lymphoma/thymoma
- Diuretics and low salt diet
- Treat IICP if presented : hyperventilation, mannitol (loading dose 1mg/kg of 20% manitol solution) with fluid
replacement (input = urine output)
- Caution : no IV fluid or drugs at upper limbs
REFER for specific treatment
- Tissue Dx and specific Rx :
- Radiotherapy : Non-small cell CA lung, metas. solid tumor
- Chemotherapy : Small cell CA lung, lymphoma, germ cell CA
- Balloon venoplasty and SVC stenting
219.
Medicine: Endocrinology, 219
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Tumor lysis syndrome: life-threatening condition
Causes
- Treatment-associated tumor lysis of hematologic malignancies (esp. Burkitt's lymphoma, ALL, and other
high-grade lymphomas, may be seen with chronic leukemias)
- Rapidly proliferating malignancies (less common)
Clinical presentations
History : 1-5 days after antineoplastic therapy (chemotherapy or radiation
Symptoms - Hyperkalemia : arrhythmia, sudden death
- Hyperuricemia : uric acid nephropathy, renal failure
- Hyperphosphatemia : nephropathy, renal failure
- Hypocalcemia (due to hyperphosphatemia) : muscle cramps, tetany, convulsions, confusion, arrhythmia
Managements
Prevention : Prophylactic therapy
- Allopurinol 300 mg bid PO (or IV 200-400 mg/m2
) 12-24 hr. prior to chemotherapy and aggressive hydration
- NaHCO3 6–8 g PO OD or 2-3 amp of NaHCO3 + 1L D5W infusion
- R/O obstructive uropathy (U/S, CT) for abnormal baseline renal function
Emergency treatment :
- NSS (or N/2) 2-4 L/day
- NaHCO3 6–8 g /day keep urine pH = 7.0 (off when pH >> 7.0)
- Allopurinol IV 300 mg/m2
(up to 900-1200 mg/d)
- Consider diuretics to increase urine output
- Treat the others electrolyte abnormalities
Indication for hemodialysis
- serum K > 6.0 meq/L
- serum uric acid > 10 mg/dL
- serum phosphate > 10 mg/dL or increasing
- serum Cr > 10 mg/dL
- Symptomatic hypocalcemia present
Start next chemotherapy : blood chemistry at 24-48 hr. from last chemotherapy
- serum uric acid < 8.0 mg/dL, - serum Cr < 1.6 mg/dL, - Must monitor blood chemistry q 6-12 hr.
Medicine: Endocrinology, 240
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Myxedema Coma
History/Clinial presentation Investigation Management
- elderly
- treated with long-standing of
uncontrolled hypothyroidism
or previously undiagnosed
- Precipitating factors:
congestive heart failure,
myocardial infarction, GI
bleeding, cerebrovascular
accident, sepsis, drug that
impaired respiration ex.
sedatives, anesthetics,
antidepressant
- high TSH,low T3&T4
- TSH may be normal in co-
morbid nonthyroidal illness,
patients who are on
corticosteroids, dopamine,
central hypothyroidism
- CBC: anemia
- Electrolyte: hyponatremia
- Lipid:
hypercholesterolemia
- Serum LDH: high
- CPK: high
- ABG: Hypoxemia,
hypercapnia, acidosis
- loading with thyroxine 500 µg
IV bolus or via NG tube then
continue 50-100 µg/d
- hydrocortisone 50 mg IV q 6 hr
(impaired adrenal reservation in
profound hypothyroidism)
- supportive treatment: correct
metabolic disturbances, treat
precipitating factors with early
use of board-spectrum ATB,
external warming if T<30 c ,
ventilator support, aware of
severe hyponatremia and
hypoglycemia
- clinical features of
hypothyroidism
- decrease level of
consciousness or seizure
Medicine: Endocrinology, 248
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Adapted from: Harrison’s Textbook of Internal Medicine, 18th Edition e
Thyrotoxicosis
Laboratory evaluation
Thyroid function test
TSH T4 Hypothyroidism
TSH , normal T4 Treated hypothyroidism or subclinical hypothyroidism
TSH T4 TSH secreting tumor or thyroid hormone resistance
syndrome
TSH T4 T3 Hyperthyroidism
TSH , normal T4& T3 Subclinical hyperthyroidism
TSH T4 T3 Sick euthyroidism or pituitary disease
Normal TSH, abnormal T4 Consider change in thyroid-binding globulin, assay
interference, amiodarone or pituitary TSH tumor
thyrotoxicosis state of thyroid hormone excess
hyperthyroidism result of excessive thyroid function
TSH, free T4
↓TSH, ↑free T4 ↑ or ↔TSH,
↑free T4
Primary
thyrotoxicosis
Normal
Free T3
Graves’
disease?
T3 toxicosis
TSH-secreting pituitary adenoma or
thyroid hormone resistance syndrome
High
Yes No
Multinodular
goiter or toxic
adenoma
Subclinical
hyperthyroidism
F/U in 6- 12 wks
↓TSH,
↔free T4
Indications to refer to endocrinologist
1. Uncertain Dx of Grave’s disease
2. Grave’s disease with cold nodule
3. Pregnacy/Lactation period
4. Uncontrolled
5. Requires I-131 or Sx
6. Toxic Adenoma, Toxic MNG
7. Opthalmopathy
8. Severe drug allergy
249.
Medicine: Endocrinology, 249
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Causes of Thyrotoxicosis
Primary hyperthyroidism
Graves' disease (60-80%)
Toxic multinodular goiter
Toxic adenoma
Functioning thyroid carcinoma
metastases
Activating mutation of the TSH
receptor
McCune-Albright syndrome
Struma ovarii
Drugs: iodine excess
Thyrotoxicosis without hyperthyroidism
Subacute thyroiditis
Silent thyroiditis
Other causes of thyroid destruction: amiodarone, radiation, infarction of
adenoma
Ingestion of excess thyroid hormone (thyrotoxicosis factitia) or thyroid tissue
Secondary hyperthyroidism
TSH-secreting pituitary adenoma
Thyroid hormone resistance syndrome: occasional patients may have features
of thyrotoxicosis
HCG-secreting tumors, gestational thyrotoxicosis
Signs and Symptoms of Thyrotoxicosis
Symptoms
Hyperactivity, irritability, dysphoria
Heat intolerance and sweating
Palpitations , fatigue and weakness
Weight loss with increased appetite
Diarrhea
Polyuria
Oligomenorrhea, loss of libido
Signs
Tachycardia; atrial fibrillation in the elderly
Tremor
Goiter
Warm, moist skin
Muscle weakness, proximal myopathy
Lid retraction or lag
Gynecomastia
Treatment: (1) Antithyroid Drug(try medical Rx ก่อน) (2) I-131 (3) Surgery
Drugs (ไทยเฉพาะมียา 2 ตัวนี้) Propithiouracil (PTU) Methimazole (MMI)
Dosage 50–100 mg twice daily
Shorter half-life
Severe cases need higher
doses.
10–20 mg once daily
250.
Medicine: Endocrinology, 250
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Drugs Propithiouracil (PTU) Methimazole (MMI)
Follow-up free T4 มักปกติหลังได้ยา 8–12 weeks
F/U โดยตรวจ TFT ทุก 4–6 weeksเมื่อเริ่มยา เพราะอาจเกิดภาวะhypothyroidism
ได้หากไม่มีการปรับ treatment dose (พบ T4ต่า)
treatment failure มักเกิดจาก non-compliance
Specialconsiderations
Pregnancy นิยมใช้ในหญิงตั้งครรภ์ ไม่ใช้เพราะ MMI ทาให้เกิดscalp defect
and aplasia cutis ในทารก
Thyroid storm ใช้ PTU ใน thyroid storm เพราะ
ยับยั้งการเปลี่ยน T4 เป็น T3
(peripheral conversion) ทาให้ T3
ลดลง
ไมนิยมให้
Majorsideeffects
Agranulocytosis Idiosyncracy Dose dependent
Hepatotoxity Hepatitis Cholestasis
ANCA associated vasculitis พบบ่อยกว่า MMI;
มี acute renal function, arthritis,
skin ulcer, rash,sinusitis,
hemoptysis, ANCA+
ไม่ควรใช้ยานี้อีก
พบน้อย
Rash รักษาโดย antihistamine และไม่ต้องหยุดยาเดิม หรืออาจให้ antihistamine พร้อมกับ
เปลี่ยนยาเป็นอีกขนานหนึ่ง
Graves’ disease
Clinical presentations Specific signs of Graves’ disease
- age 20-50 years and elderly, women>>men - thyroid ophthalmopathy(grittiness, eye discomfort,
มักเกิดใน 3 เดือนแรกถึงเป็นปี อาการเจ็บคอ ไข้สูง แนะนาให้หยุดยาและมาพบแพทย์ทันทีเมื่อมีอาการเพื่อ work-up ห้ามให้
antithyroid drug อีกในรายที่เกิด agranulocytosis
มักเกิดใน 3 เดือนแรกหลังเริ่มยา
-Franklyn et.al., Thyrotoxicosis, published online March 5, 2012, Centre for Diabetes, Endocrinology
andMetabolism, University of Birmingham, Birmingham, UK DOI:10.1016/ S0140-6736(11)60782-4
-แนวทางการดูแลรักษาผู้ป่วยไทรอยด์เป็นพิษ, Update in Internal Medicine 2009,
ภ.อายุรศาสตร์ คณะแพทยศาสตร์ศิริราชพยาบาล
(Criteria by Burch & Wartofsky)
251.
Medicine: Endocrinology, 251
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Harrison’s Textbook of Internal Medicine, 18th Edition e
- diffuse enlarged of thyroid gland (firm consistency)
±thrill / bruit
excess tearing, proptosis, diplopia, papilledema)
- thyroid dermopathy: pretibial myxedema
- thyroid acropathy: clubbing of fingers
Signs and symptoms of thyrotoxicosis (Descending order od frequency)
Symptoms Signs
- diarrhea
- polyuria
- palpitations
- fatigue and weakness
- tremor
- goiter
- warm,moist skin
- gynecomastia
- Hyperactivity, irritability, dysphoria
- weight loss with increased appetite
- oligomenorrhea, loss of libido
- heat intolerance and sweating
- tachycardia: atrial fibrillation in elderly
- muscle weakness, proximal myopathy
- lid retraction or lag (***specific for Graves’)
Investigation TSH T3 T4
Radioactive iodine uptake : Increased uptake :Homogeneous แยกจาก Subacute thyroiditis : low uptake
Treatment
Management
การรักษาด้วยยา ( Medical treatment ):ในกรณี
1.ผู้ป่วยคอโตไม่มาก น้าหนักของต่อมไทรอยด์ น้อยกว่า 40 g
2.ระดับของ thyroid hormone ไม่มากเมื่อเริ่มรักษา
3. ผู้ป่วยที่สามารถควบคุมโรคได้เร็วหลังเริ่มรักษา และต่อม thyroid มีการลดขนาดลง
- Anti-thyroid drugs:
@ PTU ขนาด 100-400 mg/day(PTU เม็ดละ 50 mg)โดยแบ่งให้วันละ 2-4 ครั้ง
side effect ที่สาคัญ : agranulocytosis , rash , peripheral neuritis
(ใช้ในหญิงตั้งครรภ์ได้ SE: rash, hepatitis, arthralgia, agranulocytosis)
ที่มาของรูป: Harrison’s Textbook of Internal Medicine, 18th
Edition
252.
Medicine: Endocrinology, 252
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
@ Methimazole 15-20 mg วันละครั้ง(MMI เม็ดละ 5 mg)
(ห้ามใช้ในหญิงตั้งครรภ์/ให้นมบุตร, SE: rash, hepatitis, agranulocytosis)
@ Carbimazole
- β-blockers :
@ Propanolol 5-40 mg วันละ 2-4 ครั้ง, 2 mg/kg/day ในเด็ก
@ Atenolol 25-50 mg วันละครั้ง
- F/U clinical and TFT 3-4 weeks after starting treatment --> titrate dose based on free T4
- mostly achieve euthyroidism in 6-8 weeks
- patient with severe hyperthyroidism and large goiters --> most likely to relapse, should be followed
closely during the first year
การรักษาด้วยสารรังสี ( Radioactive iodine: I 131
) relapsing after antithyroid drugs(ใช้ในเด็กอายุมากกว่า 10 ปี)
การรักษาด้วยการผ่าตัด ( Surgical treatment ) ทาเมื่อ young adult with relapsing after antithyroid drugs, very large
thyroid, มีอาการกดเบียดจากต่อมไทรอยด์, สงสัยว่าเป็น malignant thyroid nodule,รับประทานยาไม่สม่าเสมอ
Hashimoto’s Thyroiditis
Clinical presentation
Insidious onset , greater prevalence in aging and women
Presenting with goiter (small, irregular and firm in consistency) > symptoms of
hypothyroidism*
Rarely associated with pain
* Signs and Symptoms of hypothyroidism (Descending order of frequency)
Symptoms
Tiredness, weakness, Dyspnea
Paresthesia
Feeling cold
Dry skin, Hair loss
Signs
Dry coarse skin; cool peripheral
extremities
Puffy face, hands, and feet
(myxedema)
253.
Medicine: Endocrinology, 253
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Harrison’s Textbook of Internal Medicine, 18th Edition e
Adapted from: Harrison’s Textbook of Internal Medicine, 18th Edition e
Weight gain with poor appetite
Impaired hearing
Hoarse voice
Constipation
Menorrhagia (later oligomenorrhea or
amenorrhea)
Difficulty concentrating and poor memory
Diffuse alopecia
Bradycardia
Peripheral edema (non-pitting)
Delayed tendon reflex relaxation
Carpal tunnel syndrome
Serous cavity effusions
Laboratory evaluation
TSH
Elevated Normal
Free T4
Normal Low
Mild
hypothyroidism
Primary
hypothyroidism
Pituitary disease suspected?
No Yes
No further tests Free T4
Low Normal
No further
tests
Drug effects?
Sick euthyroid syndrome?
Then, ant. Pituitary function
Anti TPO+ Anti TPO-
Autoimmune
Hypothyroidism
Other causes
I131 treatment
Thyroid surgery
Drugs ex. Lithium
Iodine deficiency
Infiltrative disorder
ex. amyloidosis
T3 are not indicated.
254.
Medicine: Endocrinology, 254
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Management
Adult : start thyroxine 50-100 µg/day (1.6 µg/kg)
Elderly with CAD : start thyroxine 12.5-25 µg/day then adjust dosage every 2-3 months
until TSH is normalized (beware of CAD attack, arrhythmia, heart failure)
adjust 12.5-25 µg a time to keep TSH in the lower half of the normal range (F/U TSH every 2
mths if start or adjust dosage) if TSH level is archieved and stable F/U lab annually)
Less absorbed when taken with dietary fibers, drugs ex CaCO3 ,FeSO4, Al(OH)3
Drug interaction: increased clearance when taken with estrogen, rifampicin,
carbamazepine, phenytoin; amiodarone blocks peripheral conversion
Subacute Thyroiditis
Clinical presentation Treatment
- age 30-50, women>men
- history of viral infection ex. URI (several weeks
before)
- fever, painful and enlarged goiter
- NSAIDs for control symptoms
- uncontrolled case : prednisolone 40-
60 mg /day and taper 6-8 weeks if
symptoms are getting better
- thyrotoxic phase: spontaneous
recovery, no role of antithyroid drugs
- hypothyroid phase: thyroxine
replacement maybe needed (low
dose 50-100 µg/d)
255.
Medicine: Endocrinology, 255
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
- complete resolution but permanent hypothyroidism
can occur
- monitor TSH, free T4 every 2-4
weeks
Sick euthyroid syndrome
History
Investigation/management
- severe illness without underlying thyroid
disease 0r abnormal TFTs
- ↓total of free T3, ↔T4 and TSH
(impaired peripheral conversion)
- monitor TFTs during recovery
- thyroid hormone supplement only in historic
or clinical evidence suggestive
hypothyroidism
256.
Medicine: Endocrinology, 256
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Adapted from: Harrison’s Textbook of Internal Medicine, 18th Edition e
Subclinical thyroiditis
History/Clinical presentation Management
- few or no apparent clinical
features of hypothyroidism
- treat : if sustained elevation of TSH > 10 mU/L over 3 months
: start with thyroxine 25-50 µg/d
- not-treat : follow up TFT annually
Approach to thyroid nodule
Repeat U/S
guided FNA
in 3 months
Surgical indication
Total thyroidectomy/
lobectomy
Nondiagnostic
c
Repeat U/S in
6-12months
Benign
Assess and
treat for
thyrotoxicosis
Hot nodule Cold nodule Negative for
malignancy
Malignancy
Ultrasound-guided FNAThyroid scan
↑ or normal↓TSH
TSH
Suspicious
lesion
Malignancy
257.
Medicine: Endocrinology, 257
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Diffused non-toxic goiter (Simple goiter)
History Clinical presentation/Investigation
- diffuse enlargement of thyroid
- no signs of hyperthyroidism
- cause: iodine deficiency
: goitrogens ex. กะหล่าปลี, ดอกกะหล่า
- may cause tracheal and esophageal
compression
- PE: symmetrically enlarged, not tender, soft
gland without palpable nodules
- TSH : normal or slightly increased
- T3 : normal
- total T4 : slightly decreased
Treatment : younger adult thyroxine 100 µg/d, elderly thyroxine 50 µg/d
: increase efficient of treatment in younger and soft goiter
: significant regression within 3-6 months after this time is unlikely to occur
: surgery is rarely indicated except compression symptoms
Multinodular goiter
Non-toxic multinodular goiter Toxic multinodular goiter
- asymptomatic and euthyroid
- can cause compressive symptoms to
trachea, esophagus and neck vein
- sudden pain cause by hemorrhage into
- subclinical hyperthyroidism or mild
thyrotoxicosis
- elderly with atrial fibrillation, tachycardia,
palpitation, nervousness, tremor, weight loss
258.
Medicine: Endocrinology, 258
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
nodule
- normal TFT - low TSH
- normal or minimally increased of T3 and T4
- conservative treatment
- T4 suppression is rarely reduced thyroid size
(start at low dose: 50 µg/d)
- avoid contrast agents or iodine-containing
substances
- antithyroid drugs and beta-blocker for
normalizing thyroid function
- but can stimulate the growth of goiter
Medicine: Rheumatology, 267
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
ข้อขึ้นลงแบบ intermittent ร่วมด้วย
Management
Treat predisposing disease
Osteomyelitis
History Physical examination Investigation
- อาจมีประวัติ trauma, infection อื่นๆ
นามาก่อนไม่เกิน 1 สป.
- neonate: sepsis, toxic
- older infant: เด็กไม่ลงน้าหนัก,ไม่ใช้ข้อ
นั้น(ส่วนมาก proximal tibia, distal
femur)
- sudden onset of fever with joint
pain
- fever,irritability
- sign of inflammation with point
of tenderness over infected
area
- CBC พบ leukocytosis
- CRP&ESR
- Hemoculture (+>50%)
- plain film จะพบ bone destruction and
periosteal elevation 10-14 วันหลัง
infectionจึงไม่จาเป็นต้องส่งทุกราย
- MRI
Management
1 specific treatment
- intravenous antibiotic ซึ่งการให้ยานั้นจะขึ้นกับเชื้อก่อโรค
Age Bacteria empirical ATB
< 3 mo GBS,S.aureus,
E.coli,
Cefotaxime 100-300 mg/kg/day IV q 6hr or Cloxacillin 50-100
mg/kg/day IV q 6 hr + Gentamycin 5-7 mg/kg/day IV q 8-24hr
268.
Medicine: Rheumatology, 268
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
>2 mo-
children
S.aureus,
GrA Strep,
H.influenzae
2nd
-3rd
gen Cephalosporin เช่น
Cefoxitin 80-160 mg/kg/day IV q 6-8hr
Cefotaxime 100-300 mg/kg/day IV q 6hr
หากมีประวัติถูกของตา เชื้อมักเป็น P.aeruginosa ควรให้
Ceftazidime 100- 150 mg/kg/day IV q 8 hr
จะให้ IV ATB ไปจนกว่าไข้จะลด,ข้อลดบวม(ประมาณ 7-10 วัน) หลังจากนั้น
จึง เปลี่ยนเป็น oral ATB เช่น Dicloxacillin 25-50 mg/kg/day PO qid ac จน
ครบ 4-6 wk
- surgical drainage ทาเมื่อพบว่ามี abscess หรือ ไม่ตอบสนองต่อ ATB ใน 48 ชม
2 supportive treatment - correct dehydration - oral analgesic - splint
* osteomyelitis
acute osteomyelitis
Osteoarthritis ( OA )
History Clinical presentation Investigation
- Risk factors : advanced age,
genetic, abnormal joint
structure, previous joint
trauma, obesity, repetitive use
- Most common : knee, hip,
spine, DIP, PIP, 1st
CMC
- Pain , limit ROM
- Morning stiffness < 30 mins
- Worsen c activity& Wt bearing
- Relieve by rest
- Crepitus
- Joint enlargement
- Node (hand)
Heberden’s node --- DIP
- CXR :
Early : joint space narrowing
Late : subchondral sclerosis ,
marginal osteophyte , and
subchondral bone cyst
269.
Medicine: Rheumatology, 269
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Bouchard’s node --- PIP
Management
- Education , Weight reduction, Exercise, Assistive devices
- Physical therapy
- Medication
Paracetamol
NSAIDS
Celecoxib (200) 1 tab oral OD, pc OR
Naproxen (250) 1 tab oral tid, pc OR
Ibuprofen (400) 1 tab oral tid, pc OR
+ Omeprazole (20) 1 tab oral OD, pc
- Surgery : arthroplasty , osteotomy , and prosthetic joint replacement
Seronegative spondyloarthropathy
Ankylosing spondylitis
Def . chronic inflammation disease of the joints of the axial skeleton
history Clinical presentation investigation
-มาด้วยอาการปวด และ มีข้อติดที่กระดูกสัน
หลังอย่างช้าๆ
-จะเริ่มเป็นเมื่อเข้าสู่ วัยรุ่นตอนปลายหรือ
ผู้ใหญ่ตอนต้น
-พบในเพศชาย > เพศหญิง
DDx low back pain
1. Mechanical cause
-bouts of back pain that radiate into
the bucktock
-back pain จะแย่ลงในตอนเช้า และบ่อยครั้งจะมี
ข้อติดนานหลายชั่วโมง
-อาการปวดและข้อติดจะดีขึ้นเมื่อทา activity ซึ่ง
เอาไว้แยกกับ back pain จาก mechanical
cause and degenerative disease ซึ่งจะดี
เมื่อ rest แย่ลงเมื่อทา activity
-ESR
-HLA-B27 +ve
-imaging
SI joint change : erosion and
sclerosis of SI joint bilateral
and symmetrical
-Bamboo spine is late
270.
Medicine: Rheumatology, 270
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
2. Disk disease
3. Degenerative arthritis
radiography
Treatment
A. Basic program : ให้ความสาคัญกับ postural and breathing exercise
B. Drug therapy :
NSAIDs first line treatment และอาจช่วย ชะลอ progression of spinal disease
TNF inhibitors efficacy for NSAIDs resistant
Sulfasalazine 1000 mg oral b.i.d บางครั้งอาจจะมีประโยชน์ ใน peripheral arthritis แต่ไม่สามารถใช้ใน
spinal and SI joint
Cortico-steroid มีประโยชน์น้อยต่อ arthritis โดยเฉพาะอย่างยิ่ง spondylitis และอาจทาให้อาการแย่ลงจาก
osteopenia
Prognosis ; ผู้ป่วยส่วนใหญ่อาการยังคงเป็นอยู่นานหลายปี เป็นโอกาสยากที่คนเป็นโรคนี้จะหายขาดเป็น
เวลานาน ความรุนแรงของโรคมีความแปรผันมาก
Reactive Arthitis (Reiter syndrome)
History Clinical presentation Investigation
- associated with a recent prior or co-existing
extraarticular infection esp enteric and
genitourinary infection
-duration : several days to weeks
-Chlamydia trachomatis, Yersinia,
Salmonella, Shigella and Campylobacter
- asymmetric oligoarthritis, often
affecting the lower extremities
- conjunctivitis, anterior uveitis
- skin or genital rash
-used to confirm prior
infection and to exclude other
causes of arthritis
เช่น joint aspiration , stool culture
271.
Medicine: Rheumatology, 271
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Management
- NSAID: naproxen 500 mg tid # at least 14 days
or indomethacin 50 mg tid # at least 14 days
-Intraarticular injection with corticosteroid ไม่เป็น C/I แม้พบorganismใน joint fluid
-Antibiotics ถ้ามี acute infection อื่นร่วมด้วย
Psoriatic arthritis
Arthritis จะเกิดขึ้น 15-20 % ของผู้ป่วย psoriasis
history Clinical presentation investigation
-A symmetric polyarthritis แต่
involve น้อยกว่า RA
-Psoriasis skin lesion
-DIP joint เป็นข้อแรกที่มีการอักเสบ
และ pitting of the nail and
onycholysis บ่อยครั้งจะมาร่วมกับ
DIP joint involvement
-Arthritis จะเกิดขึ้นหลัง skin psoriasis
-Severe skin disease มีโอกาสเกิด arthritis
มากกว่า mild skin
-ดังนั้นถ้ามีอาการ arthritis ครั้งแรกอย่าลืม
หา cutaneous lesion ด้วย
-Sausage appearance of finger and toes
-x-ray สามารถช่วยแยกโรค
จาก arthritis อื่นๆได้
-marginal erosion of bone
,
Irregular destruction of
joint and bone in phalanx
Treatment
1. NSAIDs ใช้ในกรณีเป็นเล็กน้อย
2. Methotrexate (7.5-20 mg oral once a week) เป็น drug of choice ในกรณีที่ไม่ตอบสนองต่อ NSAIDs และ
Medicine: Infectious, 273
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
INFECTIOUS
Acute Febrile Illness (fever < 2wk.)
แนวทางการวินิจฉัย Acute Febrile Illness ให้ซักประวัติ ตรวจร่างกายหาว่ามี specific organ หรือ system ที่
เกี่ยวข้องชัดเจนหรือไม่ (with specific organ involvement VS without specific organ involvement) ถ้ามีก็ให้การรักษา
ไปตามโรคที่พบนั้น ส่วนในกรณีที่ไม่มี specific organ involvement ชัดเจนนั้นในประเทศไทยมีโรคที่พบบ่อยได้แก่
Dengue
Malaria
Leptospirosis
Melioidosis
Typhoid fever / enteric fever
Rickettsia / Scrub typhus
Dengue Hemorrhagic Fever
Diagnostic criteria Physical examination Investigation
1. fever 2-7 days
2. evidence of hemorrhage
- Tourniquet’s +ve
- bleeding per gum, petechiae, ecchymosis,
GIB, bleeding @ puncture site
3. evidence of plasma leakage
- Hemoconc. > 20% of baseline
- pleu.effusion,ascites,hypoproteinemia
4. thrombocytopenia (Plt. < 100,000)
Dengue shock syndrome
Dehydration, petechiae,
redness, MP rash,
tender hepatomegaly,
non-tender
lymphadenopathy (may
be normal in febrile
phase)
Tourniquet’s test: + (20/ตร.นิ้วPPV
60%)
CBC: WBC(lymphocyte
predominate) then Plt. then
Hct
Blood smear: atypical lymphocyte,
platelet decrease
BUN/Cr & Urine sp gr: evaluate
dehydration
LFT: AST ALT
ESR มักไม่สูงมาก
274.
Medicine: Infectious, 274
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
= 4 criteria
+circulatory failure (HR,PP<20,BP)
Disease progression
3 phases 1. febrile phase (2-7 days)
2. shock phase (Day 4-5)
Initial Warning signs: fever, Plt., Hct.
Early signs = narrow pulse pressure
3. convalescent phase “ABCD”
Appetite, Bradycardia, Convalescent rash, Diuresis
Managements: Febrile phase:
Tepid sponge ด้วยน้าธรรมดา
anti-pyretic: Paracetamol, NSAIDs should be avoided
adequate hydration (ดื่มORS, ถ้าให้IV <50%maintenance)
F/U clinical & CBC
Shock phase or initial warning sign:
monitor V/S & I/O & Hct q 4-6 hr
5% D/NSS or NSS (depend on volume and hydration status and Hct)
1.Hct ไม่shock M + 3-5%def (or 5-7cc/kg/hr)
2.Shock 10-20 cc/kg push in 15 min แล้วค่อยๆลดrate IV
ถ้าcrystaliodไม่ไหว ให้colloid เช่น 10%dextran, FFP (10 cc/kg/hr, <30cc/kg/day)
275.
Medicine: Infectious, 275
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Malaria
History Physical examination Investigation
spike fever with chill, headache
Hx of travel in endemic area
(กาญ,ตาก,แม่ฮ่องสอน,พม่า,
เวียดนาม) incubation period:
14 days(Pf) or 17 days(Pv)
Fever, mild jaundice,
anemia,
hepatosplenomegaly,
NO rash
No lymphadenopathy
CBC; WBC , +thrombocytopenia
Thick/thin film: (ควรทา>3ครั้ง)
Pf: normal size infected RBC, multiple infection, ring
form, banana shape gametocyte
Pv: large size infected RBC, all form
CBC; normal WBC, possible thrombocytopenia
Severe malaria Cerebral malaria, shock, DIC, ARDS, acute RF, acidosis, hyperparasite, severe normocytic
anemia(Hct<15%), macroglobulinemia
Managements:
Uncomplicated Pf
Artesunate (tab 50mg): 4 tab OD * 3 days (total 600mg)
then day2 Mefloquine (250 mg) 3 tab and then day3 2 tab (total 1250mg)
Or Quinine (300mg) 2 tab tid + Doxycycline (100mg) 1 tab bid for 7 days
or (Clindamycin 10mg/kg iv q8h if pregnancy)
Complicated Pf
Artesunate inj 60 mg:
2.4 mg/kg (120 mg) iv stat then at 12 hr at 24 hr then 2.4 mg/kg OD * total course 5 days +
Mefloquine (250 mg) 3 tab and then 2 tab in 6 hr. later (total 1250mg)
or Quinine loading 20 mg/kg drip in 4 hr then 10 mg/kg q 8 hr x 7 d + Tetra/Doxy x 7 d
276.
Medicine: Infectious, 276
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Pv:
Chloroquine (250mg) 4-2-2-2
Day1: 4 tabs then 2 tabs in 6 hr later
Day2&3: 2 tabs/day
+Primaquine(15-22.5mg) 1tab X 14days (G-6PDอาจลดdose primaquine แล้วให้นานขึ้น)
Rickettsia
History Physical examination Investigation
fever 2-3 wk if
left untreated,
headache
systemic involvement MP rash,
conjunctival injection, gen
lymphadenopathy, splenomegaly,
black eschar Scrub typhus (only
30%of case),
pneumonia(no lung hemorrhage)
-CBC: normal
or WBC Plt atypical lymphocyte
-LFT:elevated transminase
-Serology: IgM titer>1:400, IgG titer≥1:1,600 or 4-
fold rising 14 D apart with titer ≥ 1:200
-Weil-Felix test (insensitive & nonspecific)
O. tsutsugamushi scrub typhus (vector:
chigger, rural area)
R. typhi murine typhus (less severe) (vector:
rat flea, urban/ suburban area)
Managements:
Doxycycline (100mg.) PO bid * 7-10 days
277.
Medicine: Infectious, 277
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Or Azithromycin (250) 2 x 2 x 3 days (in pregnancy or doxycycline allergy)
Or Tetracycline (500) 1 x 4 x 7 days
ถ้ารักษา 4-5 วัน ไข้ยังไม่ลง อาจ add chloramphenicol 1g IV q 6 hr (G6PDต้องnormal)
Leptospirosis
History Physical examination Investigation
Incu. period 2-30 d
fever, ตาแดง, เหลือง,
headache, N/V,
myalgia esp.calf/back,
Hx contact of
contaminated water
Transmission skin
contact to urine of
reservoir
Reservoir rodent, dog,
cat, bat, sheep, cow,
buff
Fever, conjunctival suffusion*, possible
jaundice, hepatosplenomegaly(25%),
stiffneck(aseptic meningitis)
NO lymphadenopathy
Severe form (Weil’s disease)
มีmultiorgan involvement
>2 followings
- Jaundice, hepatitis
- renal impairment
- respiratory involvement;
pneumonia, ARDS, lung hemorrhage
- CNS involvement
(- Pericarditis, myocarditis, CHF, arrhythmia,
- DIC, thrombocytopenia
- Rhabdomyolysis, acalculous cholecystitis,
CBC: normal
or WBC with N,+ Plt
Serology(เมื่อไข้>5วัน):
IgM titer>1:800 or
4-fold rising 14 D apart
PCR: from serum, CSF or urine
(expensive)
BUN/Cr & U/A: look for renal
impairment
LFT: bilirubin>>
transaminase
(hepatocellular, cholestasis)
Coagulogram: +prolong
CXR: อาจพบ patchy infil or
278.
Medicine: Infectious, 278
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
pancreatitis ) bilat pul edema (lung hemorrhage)
Managements:
1. Doxycycline 100 mg. PO bid for 7 days รักษาRickettsiaได้ด้วย
2. Penicillin G 1.5-2 mu IV q 4-6 hr for 7 days (SE: Jarish-Herxheimer’s syndrome ไข้สูงจากการให้ครั้งแรก)
3. Ampicillin 1 g IV q 6 hr for 7 days
4. Ceftriaxone 1 g. IV OD for 7 days
5. Ceftazidime 2 g IV q 8 hr for 7 days
6. Azithromycin (250) 2 x 2 pc
7.Chloramphenicol 1 g IV q 6 hr (G6PDต้องnormal)
Melioidosis (Burkholderia pseudomallei)
History Physical examination Investigation
พบมากในฤดูฝน esp.อีสาน
Risk- thalassemia, DM,
renal insufficiency, soil &
water exposure เช่น
ชาวนา, (50%ของผป.ไม่มี
risk)
Transmission respiratory,
direct contact (ดินน้า ทาง
บาดแผล) ไม่ค่อยพบจากคน
clinical
-acute infection
(incubation 2 days–9 wks)
-chronic
Most cases – prolonged fever
1 sepsis without localizing signs
2 organ-specific
CBC: WBC with N or
leukopenia
Pus G/S C/S: Gm –ve rods(safety
pin, bipolar staining)
Serology: Melioid titer cut off >
1:160 in endemic area and 4-
fold rising (sensitivity70%
specificity70%)
CXR: อาจพบ ipsilateral patchy
279.
Medicine: Infectious, 279
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
สู่คน •Pneumonia - crepitation
•Liver/spleen abscess – jaundice,
hepatosplenomegaly
•Osteomyelitis or septic arthritis ( most in
non-weight bearing joints)
•Meningoencephalitis- brain abscess –
alteration of consciousness, weakness etc
•Others : pericardial effusion, parotid
abscess
infiltration
-CT intraabdominal abscess –
honeycomb or swiss cheese
appearance (hypoechoic, multi-
septate, multi-loculate)
Severity แปรผันตาม จานวนเชื้อ, host immune
Managements:
1 Intensive phase 10- 14 days IV : Ceftazidime 2 g IV q 8 hr x +/- bactrim
Alternative drugs : Imipenem 1 g IV q 8 hr , Meropenem 1 g IV q 8 hr,
Sulperazone 1 g IV q 8 hr (Augmentin 1.2 g IV q 4 hr failure rateสูง)
2 Eradication phase : Bactrim + doxycycline (100)1*2 po pc * 12-20 wk ป้ องกันrelapse เชื้อซ่อนตัวใบphagocyte
ของมนุษย์ได้ Dose bactrim <40 kg: bactrim(400/80) 2*2 po pc, 40–60kg: 3*2 po pc, >60 kg: 4*2 po pc
Alternative drugs : -augmentin(625) 2x3 pc, ciprofloxacin 500mg bid + azithromycin 500mg OD
Typhoid fever/enteric fever (ไข้ไทฟอยด์หรือรากสาดน้อย)
History Physical examination Investigation
เกิดจากเชื้อ Salmonella typhi, high fever, bradycardia CBC: ส่วนใหญ่ WBC, Plt
280.
Medicine: Infectious, 280
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Incu. period 7-14 D อาการ
ทั่วไปคือมีไข้สูง หนาวสั่น ปวด
ศีรษะ ปวดตามตัว ปวดท้องทั่วๆ
ผู้ป่วยอาจมีอาการท้องผูกหรือบาง
รายอาจท้องเสียได้ รายที่เป็นนาน
อาจมีซึม สับสน
Transmission Fecal-oral route
(sphygmothermic
dissociation), rose-
colored spots on lower
chest & abdomen,
hepatosplenomegaly
LFT: bilirubin,transaminase2เท่าของปกติ
Coagulogram: อาจมี prolong PT,aPTT เล็กน้อย
Widal test ที่ช่วยบอกว่าเป็น typhoid คือ (1) มี 4-fold
rising ใน 7 - 10 วัน หรือ (2) ระดับ Titer สูงกว่าเกณฑ์
(ซึ่งแตกต่างกันในแต่ละห้อง Lab,ที่ศิริราช Cut off titer:
O antibody 1:160 , H antibody 1:100) <มี false
negative ได้ใน wk แรก>
** การตรวจที่เชื่อถือได้มากที่สุดคือ culture for
salmonella, ส่วน widal test มีทั้ง spec และ sense
ต่า แพทย์หลายคนจึงไม่เชื่อในผลที่ได้หากไม่สอดคล้อง
กับประวัติและตรวจร่างกาย**
Managements:
1. ceftriaxone 1-2 g/day IV หรือ ciprofloxacin tab 250 mg 2x2 โดยทาการรักษานาน 10-14 วัน
2. ยาอื่น เช่น amoxycillin 1-1.5 g รับประทานวันละ 4 ครั้ง, Bactrim 2 tab PO qid เป็นเวลา 14 วัน
281.
Medicine: Infectious, 281
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Tetanus (Clostridium tetani; drum stick)
General data Physical examination Investigation
Locked jaw, dysphagia , Hx. contaminated
wound
Transmission ไม่ติดจากคนสู่คน
Incubation period 3-21 days
Type 1.Local วินิจฉัยยาก
2.Cephalic tetanus เป็นที่ head&neck
3.Generalized tetanus (80%)
Locked jaw, stiffneck,
generalized rigidity of muscle, m spasm,
opisthotonos, Risus sardonicus
with good conscious!
Spatula test: กดposterior pharynx
spasm of masseters
Complication; laryngospasm, HT, PE
no
DDx. Meningitis, peritonsilar abscess, mandible dislocation, Rabies, stroke, encephalitis
Managements:
Supportive & wound management -dark & quiet room -prophylactic intubation
Medication
-TT 1 course + TAT 3,000 – 5,000 U IM once
-PGS 2 mU IV q 4 hr x 10 days or Metronidazole 500 mg oral or IV q 6 hr or Doxycycline
-Diazepam 5-10 mg prn q 4-6 hr
- + Phenobarb, succinylcholine
-Baclofen intrathecal
282.
Medicine: Infectious, 282
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Fever of Unknown Origin or Prolonged fever
- Fever T> 38.3 C, more than 3 wks
- Undiagnosed after investigations 3 days of admission or 3 visits of OPD
Consider Host (compromised or competent) เพราะมีกลุ่มผู้ป่วยที่มีภูมิคุ้มกันบกพร่องมากขึ้น เช่น neutropenia อาจไข้
จาก gram negative sepsis หรือ Graft versus host disease และกลุ่ม HIV ที่อาจเกิดจาก opportunistic infection or IRIS
(immune reconstitution inflammatory syndrome)
History อายุ โรคประจาตัว ยาที่ใช้ ประวัติการเดินทาง โรคระบาดในท้องถิ่น ประวัติเพศสัมพันธ์ อาการตามระบบ
Physical examination ที่ควรมองหา
-oral ulcer for SLE , Behcet’s disease,disseminated histoplasmosis,penicilliosis
-sinus tenderness for sinusitis
-temporal artery nodule or decrease temporal pulsation for temporal arteritis
-eyes Roth’s spot in retina from Infective endocarditis (IE)
-skin & nails Osler’s node , Janeway lesion, splinter hemorrhage for IE or palpable purpura , digital ulceration for
vasculitis
-genitalia & PR for ulcer or abscess
-heart new murmur for IE
-thyroid enlarge & tender for thyroiditis
Medicine: Dermatology, 314
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Managements :
0.3% Lindane Shampoo( 0.3%Gamma benzene hexachloride)
Apply to dry head or pubic hair and surrounding areas; all night x 2day ; repeat next 1wk
5% Permethrin cream SD
Apply topically to affected area; leave 5-10 min, then rinse
ซักและตากแดด เสื้อผ้าและเครื่องนอน อาจโกนขนหากเป็นที่genitalia
Acne
Signs and Symptoms
Severity mild : comedone ส่วนใหญ่ หรือมีสิวอักเสบ(papule,pustule) ไม่เกิน 10 จุด
moderate : papule,pustule ขนาดเล็กมากกว่า 10 จุดและ/หรือnodule
มากกว่า 5 จุด
severe : pustule.papule มากมาย มี nodule หรือcyst จานวนมาก หรือมี
nodule อักเสบอยู่นานและกลับเป็นซ้า
Managements :
Mild ใช้ยาทา 1% Clindamycin solution bid
2-4% Erythromycin gel or solution bid
2.5-5% Benzoyl peroxide bid 10-30 นาทีล้างออก
0.01-0.05% topical retinoids hs
Moderate ใช้ยาทาร่วมกับยารับประทาน Doxycycline 100-200 mg/day หรือ
Tetrecycline 500-1000 mg/day หรือ
Amoxycillind 500-1000 mg/day
2-3 mo
mmm
315.
Medicine: Dermatology, 315
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Severe ใช้ยาทา, ยารับประทาน ร่วมกับ ถ้าไม่มีเพศสัมพันธ์ ให้ Isotretinoin (Roaccutane) 0.5-1 mg/kg/day
(ปากจะแห้งมากถ้าใช้ยาขนาดนี้แล้วจริงๆ เขาให้ dermatologist สั่งยานะครับ)
ระวัง!! ถ้าจะตั้งครรภ์ต้องคุมกาเนิดหลังหยุดยา 2 เดือน กาชับว่าห้ามแบ่งยาให้ผู้อื่น และห้ามบริจาคเลือด ต้อง
เซ็นยินยอมก่อนใช้
ระมัดระวังเรื่องการที่คนไข้แกะ และบีบสิว
Psoriasis
Chronic relapsing disease, อายุที่พบบ่อย 20-30, 50-70 years
The lesions are usually symmetrically distributed and are
characteristically located on the ears, elbows, knees, umbilicus, gluteal
cleft and genitalia. The joints (psoriatic arthritis), nails and scalp may
also be affected.
Physical exam : Skin (&scalp), nails, mucosa, joint (finger, toe, spine)
“Skin”
1. Erythematous papules or plaques
2. well-defined border
3. silvery scales
4. Auspitz sign +ve
5. at pressure areas / traumatic areas
(knee, elbow, shoulder, coccyx, scalp)
“Nail” 50% fingers 35% toes
Pitting* nail, oil spot,
subungual hyperkeratosis,
onycholysis,
onychodystrophy
“Arthralgia & arthritis” Seronegative
1. Asymmetrical oligoarthritis
(finger, toe)
2. Symmetrical oligoarthritis
3. Classical psoriatic arthritis (DIP jt)
4. Arthritis mutilans
5. Ankylosing spondylitis
316.
Medicine: Dermatology, 316
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
20% Koebner phenomenon
ชนิดของสะเก็ดเงิน
Type Clinical features Precipitating
causes
Treatment
Plaque-type
or Psoriasis
vulgaris
(most
common,
stable form)
Red, thick, scaly lesions with
silvery scale
Stress, infection,
alcoholic
beverages, trauma,
medications,
xerosis
Localized:
topical therapy with corticosteroids,
calcipotriene (Dovonex), tars,
anthralin (Anthra-Derm) or
Tacrolimus
Generalized: phototherapy, systemic
agents, combination therapy
Guttate ;
good
prognosis
Tear drop-shaped, pink to salmon,
scaly plaques, 0.5-1.5cm ; usually
on trunk, sparing of palms and
soles
Streptococcal
throat infection
Ultraviolet B phototherapy(narrow
band), natural sunlight
Pustular
(localized)
Erythematous papules or plaques
studded with pustules; usually on
palms or soles
Stress, infection,
steroid withdraw,
preg, drugs
Same as for plaque-type psoriasis
Pustular
(generalized)
“Von
Zombusch
Same as localized with a more
general involvement; may be
associated with systemic
symptoms such as fever, malaise
(chloroquine, Li, b-
blocker, OCP,
terbinafine)
Systemic therapy and/or
hospitalization usually required
Medicine: Dermatology, 319
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Side effect – teratogenic, premature epiphyseal closure ในเด็ก, dyslipidemia, hepatitis (หลังกิน 4 wk)
Neotigason (Acitretin) หยุด 1-2 ปี ก่อนมีบุตร
Etretinate หยุด > 2ปี ก่อนมีบุตร
-Combined RE-PUVA, climatotherapy, biotherapy,…
-ไม่ให้ systemic corticosteroid เพราะผื่นไม่ค่อยยุบ มีผลข้างเคียงสูง และมี remission สั้น
การให้ความรู้เกี่ยวกับโรคแก่ผู้ป่วยและญาติ (Education)
- โรคสะเก็ดเงินเป็นโรคเรื้อรังที่มีอาการเด่นทางผิวหนังอักเสบ ไม่สามารถรักษาหายขาด แต่ควบคุมได้ด้วยยา
ในบางกรณีอาจมีผื่นตลอดชีวิต และโรคอาจมีการกาเริบเป็นช่วงๆ ได้
- เป็นโรคไม่ติดต่อ ไม่มีผลต่ออวัยวะภายใน, สาเหตุไม่ทราบแน่ชัด แต่เชื่อว่าเกี่ยวกับกรรมพันธุ์
- ควรหลีกเลี่ยงปัจจัยกระตุ้นให้โรคกาเริบเช่น การดื่มเหล้า การแกะเกา และรบกวนผิวหนังในลักษณะต่างๆ ผิวไหม้แดงจาก
แสงแดดและ ความเครียด (stress) การติดเชื้อบางชนิด ยาบางชนิด เช่น ยาต้านมาลาเรีย ยาลดความดันโลหิตกลุ่ม beta-
blocker, ยาแก้ปวด NSAIDs, ยา lithium สามารถกระตุ้นให้โรคกาเริบได้ (รวมถึง steroid withdrawal)
Prescribing an Appropriate Topical Corticosteroid Preparation
1. Characteristic of the skin lesion
Thick and chronic plaquehigh to highest potency Acute and thin lesionlow to medium potency
2. Application area
For face, and intertrigenous skin (axillar, groin, area beneath breast), chose low potency topical steroids.
Higher steroid potency can also be used for a limited 2 week period, potent topical corticosteroid may
cause striae that is permanent local side effect.
Trunk and extremities with thin skin are suitable with moderate potency topical corticosteroids
320.
Medicine: Dermatology, 320
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Steroid acne at face, neck, chest, back may develop when used moderate potency more than 2 wk
For palm and sole where the keratin is thick, chose high to highest steroid potency.
In a condition which requires a wide application area, choose low to moderate potency.
3. Consider corticosteroid potency
The potency of any topical steroid may vary considerably depending upon the vehicle (ointment>cream>lotion),
and whether or not an occlusive dressing is used (increase potency up to 10X).
Topical steroids classified according to their potency
Relative Potency Generic Name Brand Name
Low Hydrocortisone 1%*, 2.5%
Iowest potency
Cortate,
Unicort
Cortisporin
Prednisolone 0.5% Prednisil cream
Triamcinolone acetonide 0.02% Simacort 0.02% cream
Aristocort 0.02% cream
Medium Triamcinolone acetonide 0.1% Kenalog
Kela 0.1% cream,lotion
Laver 0.1% lotion
Prednicarbate 0.1% Dermatop
Clobetasone-17-butyrate 0.05% Eumovate
Fluocinonide 0.05% Lidex, Lidemol
Fluocinolone acetonide 0.025% Synalar®, Synamol®,
Supralan cream
Derma-Smooth®1
Momethasone furoate 0.1 Elomet cream, Nasonex nebule
Amcinonide 0.1%
Betamethasone valerate 0.05%, 0.1% Betnovate cream, Celestoderm
321.
Medicine: Dermatology, 321
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
High Desoxymethasone 0.25%Topicorte®, Esperson®
Betamethasone dipropionate 0.025%, 0.05% Propaderm
Diprosone 0.025%
Diprolene Glycol 0.05%
Halcinonide 0.1% Halog®
Triamcinolone acetonide 0.5% Aristocort C®
Highest Clobetasol-17-propionate0.05%**
** most potent
Dermovet® (cream, ointment,
scalp lotion)
Clobasone cream
Clobet cream
Augmented betamethasone dipropionate 0.05% Diprotop cream, ointment
Effects of drug preparation on topical steroid potency
Moderate potency High potency Highest potency
0.1% TA lotion, cream 0.1% TA ointment
0.05% Betamethasone dipropionate
lotion
0.05% Betamethasone dipropionate
cream
0.05% Fluocinonide cream 0.05% Fluocinonide
ointment
4. Preparations
Preparation Usage
Lotion (Water + Powder)
Solution
Area with hair because it can be applied easily over a large area.
Cosmetically acceptable
Contain preservative thus higher chance for allergic reaction
Gel Useful in most condition.
Evaporate quickly thus leave no sticky feeling
322.
Medicine: Dermatology, 322
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Contain alcohol which could irritate the cracked or ulcerated skin
Cream (Water>Oil) Useful in most condition.
Help dry out the lesion area.
Contain preservative thus higher chance for allergic reaction
Ointment (Oil>Water) Suitable with dry skin area
usually contain no preservatives
5. Duration of steroid use
Moderate to high potency steroid should not be continuously used for more than 3 months.
Highest potency steroid should not be used for more than 3 weeks.
6. Prescribing amount
Usually topical steroids are prescribed to apply bid, mometasone furoate (Elomet cream) can prescribe to apply
once daily.
The amount used in a single application is as followed
Amount enough for single
use
Body area
2 g Head, Each arm, Anterior chest, Posterior chest, Abdomen, Lumbar and buttock
4g Each leg
7. Adverse effect
Hypopigmentation หายได้ แต่ใช้เวลา
Atrophic change : striae, telangiectasia, purpura, skin&lipoatrophy (จากintralesional) ไม่หาย
Local infection (tinea incognito)
Steroid acne/acneiform eruption: erythematous monomorphic stage at acne prone area; chest, back,
face, neck.
Hypertrichosis (increase hair growth at the application area)
Allergic contact dermatitis from steroid itself or from preservatives presence in the preparation
Perioral dermatitis หากทาบริเวณปาก
Glaucoma หากทาperiorbital
Tachyphylaxis ทายานานเป็นปี ดื้อ หากเปลี่ยนยาสักพักแล้วจะกลับมาใช้ตัวเดิมได้
Systemic side effect หากทา >10% BSA >7 day
323.
Medicine: Dermatology, 323
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
o Cushing syndrome เช่น moon face, hirsutism, buffalo hump, purplish striae, hyperpigmentation,
truncal obesity
o Proximal muscle weakness
o กด HPA axis
o Glaucoma (จาก increased IOP) blind ได้
o HT
o Hypernatremia
o Hyperglycemia
o Polycythemia
o GI bleeding, coagulopathy
o Immune suppression
o Osteoporosis
o Growth retardation
o Amenorrhea
324.
Medicine: Nutrition ,324
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
NUTRITION (for adult)
Estimation of caloric requirements
Basal Energy Expenditure : Harris-Benedict equation (kcal/d)
Men: 66.4 + [13.7 × weight (kg)] + [5 × height
(cm)] – [6.8 × age (years)]
หรือคิดโดยประมาณโดยใช้สูตร Men: 900 + [10
× weight (kg)]
Women: 655 + [9.6 × weight (kg)] + [1.7 ×
height (cm)] – [4.7 × age (years)]
หรือคิดโดยประมาณโดยใช้สูตร Women: 700 +
[7 × weight (kg)]
เมื่อได้ BEE แล้ว นาไปคูณด้วย Stress factor และ Activity
factor จะได้ค่าพลังงานที่ร่างกายต้องการที่ใกล้เคียงความเป็นจริงมากขึ้น
Estimates of protein requirements
Clinical conditions Protein (g/kg/day)
Healthy, non-stressed 0.8-1.0
Mild metabolic stress (elective hospitalization) 1.0 - 1.1
Moderate metabolic stress (complicated postop. care, infection) 1.2 - 1.4
Activity factor : multiplying by 1.2 for sedentary, 1.4 for moderately active, or
1.8 for very active individuals 0.7-0.9 for case on respirator
325.
Medicine: Nutrition ,325
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Severe metabolic stress (major trauma, pancreatitis, sepsis) 1.5 - 2.5 (not >2.0 in elderly)
Estimate carbohydrate requirement: 56 – 60% of total calories (less than 7 g/kg/d -IV. TPN)
Estimate lipid requirement: 1 g/kg/d (IV TPN)
Recommendation for specialized nutritional support (SNS)
- Severe underweight (BMI <14 kg/m2
): consider admission and SNS
- Significant degree of pre op. malnutrition: SNS 7-14 days pre op.
- Significant malnutrition: unintentional BW loss of >10% (>5% in elderly) during the previous 6
mo. or a weight/height <90% of standard
- Severe malnutrition: BW loss >20% of usual or <80% of standard
- NPO > 7 days: IV fluid and minimum of 100 g glucose/day
- Prolonged hypermetabolic or severely catabolic period eg. post major operation, severe trauma, severe
burn, etc.
- Systemic response to inflammation
- Organ system failure
Design of individual regimens
- Fluid requirements: maintenance + deficit + concurrent loss
- Energy requirements
- Protein requirements
- Mineral and vitamin requirements for parenteral route (reference: Dietitian's handbook of enteral and
parenteral nutrition โดย Annalynn Skipper)
326.
Medicine: Nutrition ,326
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Na : 2 mEq/kg + replacement
K : 40 – 100 mEq/d + replacement of unusual loss
Cl and acetate : as needed for acid – base balance
Ca : 10 – 20 mEq/d Mg : 8 – 16 mEq/d
P : 20 – 30 mmol
Zn : 2.5 – 4 mg/d plus 10 -15 mg/d per L of stool or ileostomy output
Vitamin A : 3,300 IU Pyridoxine (B6) : 6 mg
Thiamin (B1) : 6 mg Cyanocobalamine (B12) : 5 ug
Riboflavin (B2) : 3.6 mg Biotin : 60 ug
Niacin (B3) : 40 mg Ascorbic acid : 200 mg
Folic acid : 600 ug Vitamin D : 200 IU
Pantothenic acid : 15 mg Vitamin E : 10 IU
327.
Medicine: Nutrition ,327
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Route of administration
1.Enteral nutrition : First choice if no contraindications
- Short term (<6 wk.) : nasogastric or nasoenteric tube
- Long term (>6 wk.) : gastrostomy or jejunostomy tube
Contraindications for enteral feeding
- Persistent/intractable nausea or vomiting
- Mechanical obstruction or severe hypomotility
- Severe malabsorption
- Intolerable postprandial abdominal pain or diarrhea
- Presence of high-output fistulas that do not permit feeding proximal or
distal to the fistula
Enteral feeding products: standard formula usually provided 1 kcal/ml
o Blenderized tube feedings: any food that can be blenderized
o Nutritionally complete formula (standard enteral diet):
- Commercial formulas are convenient, sterile, and inexpensive
- Recommended for patients with minimal metabolic stress and normal gut function
o Chemically defined formula (elemental diets): predigested and readily absorbed form
o Disease specific formulations: use in specific clinical situation eg. organ failure or immune dysfunction
Feeding protocols: start with full-strength formula at a slow rate, stop when oral intake provides 75% of
328.
Medicine: Nutrition ,328
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
the required calories
o Bolus feedings: administration by gravity, not push
- Begin at 50 – 100 mL q 4 hr
- Increased in 50-ml increments until goal intake is reached (usually 240 to 360 mL q 4 hr)
- Elevate pt. head 30 to 45 degrees during feeding and 2 hr. later
- Flush feeding tube: 30 mL of water after each feeding
- If gastric residual volume > 50% of previous bolus, hold the
next feeding
o Continuous infusion: for nasojejunal or jejunostomy tube
- Begin at 20 – 30 mL/hr
- Increased in 10-mL increments q 6 hr until goal intake is reached
- Flush feeding tube: 30 mL of water after feeding
- Hold the feeding or decrease rate if gastric residual volume > 2 times the dripping rate or
abdominal distension/pain developed
o Medications that are not suitable for administration through a feeding tube include the following :
- Enteric-coated medications
- Drugs in gelatinous capsules
- Medications that are designed for sublingual use
- Most sustained-release medications
329.
Medicine: Nutrition ,329
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
2.Parenteral nutrition: consider if in adequate intake (<50% of daily requirement) for more than 7 days and enteral
feeding is not feasible
- Peripheral Parenteral nutrition: limited to 1,000 mOsm (12.5% dextrose solution) to avoid phlebitis
- Total Parenteral nutrition: via central venous catheter
Feeding protocols
- Introduction of TPN should be gradual, increased to the caloric goal
over 1 – 2 days (if no metabolic instability eg. Hyperglycemia)
- Discontinue when oral or enteral intake provides 75% of the required
calories. To prevent rebound hypoglycemia from hyperinsulinemia, the
infusion rate should be halved for 1 hour, halved again the next hour,
and then discontinued.
Monitoring
- Vital signs and serum glucose after 6 hours of initiation of TPN
- BW, fluid intake/output OD
- Serum glucose electrolyte and BUN daily for few days until stable
- Glucose, electrolyte, Ca, Mg, PO4, TG, CBC, PT, liver enzyme and billirubin
Weekly thereafter
330.
Medicine: Nutrition ,330
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Complications
Enteral nutrition
- Metabolic complications : eg. hyperglycemia, hyperosmolarity, hyper/hyponatremia, hyper/hypokalemia
- Clogging : prevent by “flush after use”, avoid mixing every drugs in the same setting
- Tracheobronchial aspiration – Aspiration pneumonia
- High gastric residual
- Diarrhea
Parenteral nutrition
- Catheter-related complications : eg. Infection, thromboembolism
- Metabolic complications : eg. hyperglycemia, hyperosmolarity hyper/hyponatremia, hyper/hypokalemia
- Refeeding syndrome: shift of extracellular ions into the intracellular space, and rapid depletion of ATP
stores resulting in cardiac arrythmias, respiratory failure and sudden cardiac death
- Hepatic dysfunction: for long-term TPN support
- Cholecystitis
การวินิจฉัยภาวะทุพโภชนาการ (Malnutrition)
ในหนังสือ ICD ฉบับที่ 1 กาหนดว่าการกาหนดความรุนแรงของภาวะ Malnutrition นั้น วัดโดยน้าหนักตัว โดยใช้ค่า Mean ของ
ค่าอ้างอิงของประชากร ร่วมกับ Standard deviation ดังนั้น
331.
Medicine: Nutrition ,331
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
1. Severe malnutrition จะมีน้าหนักตัวต่ากว่าค่า mean ของค่าอ้างอิงของประชากรอ้างอิงมากกว่า 3 standard
deviation หรือมากกว่า
2. Moderate malnutrition จะมีน้าหนักตัวต่ากว่าค่า mean ของค่าอ้างอิงของประชากรอ้างอิง 2-2.9 standard
deviation
3. Mild malnutrition จะมีน้าหนักตัวต่ากว่าค่า mean ของประชากรอ้างอิง 1-1.9 standard deviation
อย่างไรก็ตามในประเทศไทยไม่มีค่ามาตรฐานอ้างอิงของประเทศไทย จึงให้ใช้ค่า BMI มาตรฐานตาม WHO (International
classification of adult BMI. Asian & Pacific population. WHO 2004) ดังนี้
ระดับ ค่า BMI ความรุนแรง รหัส
1. BMI 17.00 – 18.49 ระดับ 1 - Mild E44.1
2. BMI 16.00 – 16.99 ระดับ 2 - Moderate E44.0
3. BMI < 16.00 ระดับ 3 - Severe E43
ในกรณีที่มีค่าน้าหนักตัวก่อนหน้านั้น การที่น้าหนักตัวไม่เพิ่มในเด็ก หรือน้าหนักลดในผู้ใหญ่ หรือเด็ก ทาให้นึกถึงภาวะ
Malnutrition โดยใช้ตารางดังนี้
% น้าหนักที่ลดลงในช่วงเวลา เล็กน้อย ปานกลาง รุนแรง
1 สัปดาห์ 1 % 1.1 - 2. % > 2 %
2-3 สัปดาห์ 2 % 2.1 – 3 % > 3 %
1 เดือน 4 % 4.1 – 5 % > 5 %
Medicine: Toxicology, 340
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
- Phentolamine, a nonselective 1-adrenergic receptor antagonist, for severe hypertension due to 1-
adrenergic agonists; Sodium nitropusside can also used 0.3 mcg/kg/min IV
- propranolol, a nonselective blocker, for hypotension and tachycardia due to 2 agonists;
- labetalol, a blocker with blocking activity, or phentolamine with esmolol, metoprolol, or other
cardioselective blocker for hypertension with tachycardia due to nonselective agents ( blockers, if used
alone, can exacerbate hypertension and vasospasm due to unopposed stimulation);
- benzodiazepines:
- diazepam 0.2 mg/kg IV at 2 mg/min; not to exceed 20 mg (as a single dose); may repeat
- lorazepam 0.044 mg/kg (2-4 mg) IV
- midazolam .01-0.05 mg/kg (usually 0.5-4 mg; up to 10 mg) IV slowly over several min; may repeat q10-
15min until adequate response achieved
- propofol.
Treat hyperthermia by mist and fan technique
Sympatolytic Toxidrome
Examples Clinical features Specific treatment
1. 2-Adrenergic agonists
:Clonidine, guanabenz,
tetrahydrozoline and other
imidazoline decongestants,
tizanidine and other imidazoline
muscle relaxants
2. Opiates, opioids
Alteration of
consciousness,
bradypnea,
bradycardia-apnea,
decreased bowel
sounds, miosis,
hypotension.
- Dopamine and norepinephrine for hypotension.
- Atropine for symptomatic bradycardia.
- Naloxone for CNS depression. An initial dose of
0.4 mg to 2 mg.
- it may be repeated at two- to three-minute
intervals
Medicine: Toxicology, 344
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Managements
-ยังไม่มีการรักษาที่ได้ผลดี
-ในรายที่ประเมินแล้วว่ามีความเสี่ยงต่อการฆ่าตัวตายให้admit และให้ยาเหมือนกับMDD
Anticholinergic Poisonings
Agents : Pure anticholinergic – Atropine, Scopolamine, Benztropine
Mixed effect – TCA (cardiac toxic), Antihistamine (Diphenhydramine)
Clinical features
delirium, coma, seizures, tachycardia, hypertension, hyperthermia, peripheral vasodilatation, dry mouth,
mydriasis, urinary retention, decreased bowel sounds
Managements
1. GASTRIC DECONTAMINATION : อาจทาแม้เกิน 1 ชม.เพราะสารพิษทาให้ GI motility ลดลง
ACTIVATED CHARCOAL :
Administer 240 mL water/30 g charcoal
Usual dose 25 to 100 g in adults/adolescents, 25 to 50 g (1 to 12 years)
1 g/kg in infants less than 1 year old
2. ทาECG มองหา QRS widening(QRS>100msec; 2.5mm), prominent R in lead avR (R wave > 3 mm และ/หรือ
r/s sinv r/q . 0.7)และ QT prolongation
3. MONITOR : FLUID, ELECTROLYTES, EKG อย่างใกล้ชิดในรายที่มีอาการ
4. PHYSOSTIGMINE : ระวังใน TCA ingestion เพราะอาจทาให้เกิดการชักและ dysrhythmias
INITIAL DOSE: ADULT: 1 to 2 mg IV over 2 min, may repeat once
345.
Medicine: Toxicology, 345
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
CHILD: 0.02 mg/kg up to 0.5 mg IV over 5 min, may repeat once
5. TACHYCARDIA: ในรายที่มี hemodynamic instability ให้ physostigmine หรือ IV β-blockers
6. VENTRICULAR DYSRHYTHMIAS :
ventricular tachycardia
พิจารณาให้ Lidocaine (Adult: LOADING: 1 to 1.5 mg/kg IV push; for refractory VT/VF may give an
additional bolus of 0.5 to 0.75 mg/kg over 3 to 5 min. Do not exceed 3 mg/kg or 200 to 300 mg over 1hr
INFUSION: 1 to 4 mg/min Pediatric : LOADING : 1 mg/kg ; INFUSION: 20 to 50 mcg/kg/min)
ถ้ามีประวัติtricylic antidepressant หรือมีลักษระECGของ มักตอบสนองต่อ NaHCO3 (starting dose is 1 to 2
mEq/kg IV bolus Repeat as needed)
7. SEIZURES & AGITATION : DIAZEPAM (ADULT: 5 to 10 mg, repeat q 10 to 15 min as needed. CHILD: 0.2
to 0.5 mg/kg, repeat q 5 min as needed)
8. HYPERTENSION : ในรายที่มี severe hypertension ให้ Nitroprusside (0.1 mcg/kg/min and titrate to desired
effect; up to 10 mcg/kg/min may be required)
9. HYPERTHERMIA : external cooling – mist and fan technique
10. RHABDOMYOLYSIS : Hydration keep urine output of 2 to 3 mL/kg/hr. Monitor CK และ renal function
Cannabis Intoxication (กัญชา)
Clinical features
impaired motor coordination, ครื้นเครง, วิตกกังวล, การตัดสินใจบกพร่อง, 2 ชั่วโมงหลังใช้ เจริญอาหาร ตาแดง ปาก
แห้ง ใจสั่น
Managements
ปลอบขวัญ ให้กาลังใจ, ถ้าไม่หาย ให้ diazepam 10-30 mg PO/IV
Medicine: Toxicology, 353
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
- คงยาไว้ 5-10 วัน จากนั้น ลดวันละ 0 2 mg
Organophosphate and Carbamate Poisonings
Clinical features
1. MUSCARINIC EFFECTS : DUMBELS : Diarrhea, Diaphoresis, Urination, Miosis, Bradycardia,
Bronchospasm, Bronchorrhea, Emesis, Lacrimation, Salivation
2. NICOTINIC EFFECTS : fasciculations, weakness, respiratory failure
Autonomic : tachycardia, hypertension, mydriasis
3. CENTRAL EFFECTS : CNS depression, coma, seizures
Managements
1. PERSONNEL PROTECTION :
Decontamination ก่อนเพื่อป้ องกันการได้รับสารพิษทั้งจากทางผิวหนัง การหายใจ
2. AIRWAY PROTECTION :
ให้นอนตะแคงซ้ายและดูดสารคัดหลั่งในปากป้ องกันการสาลัก ในรายที่ไม่รู้สึกตัวพิจารณาการใส่ท่อช่วยหายใจ ถ้าผู้ป่วย
ชักให้การักษาด้วย DIAZEPAM (ADULT: 5 to 10 mg, repeat every 10 to 15 min as needed. CHILD: 0.2 to 0.5
mg/kg, repeat every 5 min as needed)
3. ACTIVATED CHARCOAL :
Administer 240 mL water/30 g charcoal
Usual dose 25 to 100 g in adults/adolescents, 25 to 50 g in children (1 to 12 years)
1 g/kg in infants less than 1 year old
354.
Medicine: Toxicology, 354
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
4. GASTRIC LAVAGE :
แนะนาให้ทาเร็วที่สุดโดยจะได้ประโยชน์เมื่อผู้ป่วยได้รับสารพิษมาไม่เกิน 1 ชั่วโมง
5. ATROPINE THERAPY :
รายที่มีอาการโดยให้ทางหลอดเลือดจนมี Atropinization (พิจารณา secretion ลดลงเป็นหลัก)
Usual dose Adult - 2 to 5 mg, Child - 0.05 mg/kg
If inadequate response, double the dose and repeat it every 10 to 20 minutes as needed
Indications: Bradycardia, Bronchospasm, Bronchorrhea ให้atropine จนอาการเหล่านี้หายไป
6. PRALIDOXIME (Protopam, 2-PAM) :
ใช้ในรายที่มีอาการปานกลางหรือรุนแรง (fasciculations, coma, weakness, respiratory depression, seizures) จะได้
ประโยชน์สูงสุดภายใน 48 ชั่วโมงแรกและให้ติดต่อจน Cholinergic symptoms หายไปแล้ว 24 ชั่วโมง
WHO currently recommends an initial bolus of at least 30 mg/kg followed by an infusion of more than 8
mg/kg/hr
*Carbamate : มี Spontaneous degradation ใน 24-48 ชั่วโมง
Paraquat poisoning
เป็นสารเคมีกาจัดวัชพืชในกลุ่ม dipyridil ชี่อทางการค้ามักจะลงท้ายด้วย -xone เช่น Gramoxone paraquat
Clinical features หลังจากที่ได้รับสารมักมีอาการอาเจียน ปวดท้อง ท้องเสีย แผลบวมแดงในปาก ในรายที่
เป็นมากอาจจะมีอาการ rupture ของ esophagus ภายใน 1-4 วันผู้ป่วยจะมีอาการ systemic จาก paraquat คือมีไต
วายจาก acute tubular necrosis , เกิด hepatocellular damage ทาให้ SGOT, SGPT สูงขึ้นเป็นพันได้ หลังจากนั้น
ประมาณวันที่ 3-14 อาการทางไตและตับมักจะดีขึ้น แต่คนไข้จะมีอาการของ progressive respiratory failure ในที่สุด
มักจะเสียชีวิตภายใน 3 สัปดาห์ ในรายที่ได้รับสารเคมีนี้มากกว่า 60 ml, onset ของอาการจะเร็วภายในไม่กี่ชั่วโมง
Medicine: Toxicology, 358
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
IV NAC 150 mg/kg in 24hr or oral NAC 70mg/kg q 4hr
ให้ยาจนกว่า encephalopathy ทุเลาหรือ PT<2 เท่าและ AST/ALT เริ่มลดลง
Rumack Matthew Nomogram
จานวนเม็ดยาที่ทาให้เกิดพิษ = 150 mg/l x BW(kg)
500 mg
PCM level(mg/l) = จานวนเม็ดที่กิน x 500 mg
BW(kg)
Toxin-Induced Metabolic Acidosis
เกิดได้จากยาและสารพิษได้หลายชนิดซึ่งจะทาให้เกิด Wide anion gap acidosis
A MUDPILE : Alcoholic ketoacidosis, ASA & Salicylate, Methanol, Metformin, Uremia, DKA, Phenformin, INH,
Lactic acidosis, Ethyleneglycol
อาการและการรักษาขึ้นกับชนิดของสารที่ผู้ป่วยได้รับ ดังนั้นการซักประวัติให้ได้สารต้องสงสัยจึงเป็นเรื่องสาคัญ
สารที่พบบ่อย ได้แก่
ASA
Clinical features
fever, tachycardia, nausea, vomiting, tinnitus, compensatory respiratory alkalosis
Managements
359.
Medicine: Toxicology, 359
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
- Rehydrate with 0.9% NaCl
- Alkalinize urine - Infuse solution of 132 mEq/L NaHCO3/L D5W at 1.5-2 times maintenance to achieve
urine pH>7.5
Acidosis - Administer IV NaHCO3 1-2 mEq/kg starting dose correct pH to 7.40 (even mild acidemia
can facilitate movement of salicylate into the brain)
- Monitor - ABGs.
Hemodialysis – เมื่อ salicylate levels > 100 mg/dL, refractory acidosis, persistent CNS symptoms,
pulmonary edema, renal failure
Methanol
Clinical features
Alcoholics with (wide osmol gap if available) with worsening wide anion gap metabolic acidosis despite
supportive care with fluid and glucose, with no explainable sources of lactic acidosis.
abdominal pain, visual blurring, blindness, headache, dizziness, nausea, vomiting, bradycardia, seizures,
coma
Managements
1. Acidosis - IV NaHCO3 1-2 mEq/kg starting dose if pH < 7.2.
2. If acidosis, visual changes, MeOH > 20 mg/dL. Loading dose 10 mL/kg 10% ETOH in D5W over 20-30 min.
Maintenance: 1-2 mL/kg/hr. Maintain blood ETOH 100-150 mg/dL. Monitor blood glucose and ETOH levels.
3. Fomepizole - Indications as for EtOH. Loading dose 15 mg/kg IV over 30 min.
4. Hemodialysis - If acidosis, visual changes or methanol >20-50 mg/dL. Increase ETOH infusion during
dialysis; and increase fomepizole dosing to every 4 hours during hemodialysis
Psychiatry, 395
Survival forall draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Anorexia Nervosa
Diagnostic criteria (DSM IV)
A. ปฏิเสธที่จะคงน้าหนักให้มาก กว่า 85 % ของ expected weight ซึ่งเกิดจากการพยายามลดน้าหนัก
B. กลัวอย่างรุนแรงว่าจะอ้วนหรือน้าหนักเพิ่มขึ้นทั้งที่น้าหนักน้อย
C. การรับรู้ต่อน้าหนักและรูปร่างตนเองผิดปกติ ปฏิเสธถึงอันตรายของภาวะน้าหนักน้อย
D. ในสตรีที่มีประจาเดือนแล้ว มีการขาดประจาเดือนอย่างน้อย 3 รอบติดต่อกัน
มี 2 subtypes คือ restricting type และ binge eating/ purging type
Other important medical history
- ปัญหาจิตเวชอื่นๆ
- ประวัติอาการตามระบบเพื่อหา medical complications: electrolyte disturbance, dehydration prerenal renal
failure, CVS compromise, abnormal GI motility, hepatitis, pancreatitis, impaired growth and development,
infertility, prolonged amenorrhea (>6 เดือน) irreversible osteopenia and pathological fractures เป็นต้น
Differential diagnosis: anemia, hyperthyroidism, DM, DKA, HIV, metabolic acidosis, inflammatory bowel
disease, malabsorption, alcohol and substance abuse, alcoholic and diabetic ketoacidosis, anxiety
disorders, bowel obstruction, malignancies, chronic infections, brain tumors และ dehydration
Physical examination
Complete PE เพื่อหา medical complications
V/S: hypothermia, hypotension
GA: BWbut active, sunken eyeball, acrocyanosis, edema, เหลืองจาก hypercarotenemia หรือ
jaundice ก็ได้
Skin: ผิวแห้ง ผมร่วง lanugo hair
CVS: bradycardia, cardiomyopathy, mitral valve prolapse
RS: spontaneous pneumothorax and pneumomediastinum ได้
GI: parotid enlargement, abdominal pain
Bone: osteoporosis, pathologic fracture
Teeth: decalcification ในผู้ที่อาเจียน
Endocrine: delayed puberty.
Investigations
Lab findings อำจปกติได้ตรำบที่ยังไม่ถึง semistarvation
CBC: anemia, leukopenia, thrombocytopenia
Electrolyte: Na, K, Cl, Mg, Ca, PO , metabolic alkalosis
BUN, Cr
396.
Psychiatry, 396
Survival forall draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
U/A อาจพบ proteinuria
Fecal occult blood
Ethanol and drug screening
Abnormal blood chemistry: hypoglycemia, liver function test, cholesterol, cortisol, carotene
Thyroid function test: decreased T3 (เป็นปกติได้หลังจากน้าหนักขึ้น ไม่ต้องให้ replacement)
Chest and abdominal x-rays – ตาม Hx, PE
EKG: prolongation of QT interval, decreased QRS amplitude, nonspecific ST segment changes,
and T-wave changes แต่แม้ในผู้ป่วยที่ EKG ปกติ ก็อาจมี sudden death ได้
Brain imaging - Increase in ventricular-brain ratio secondary to starvation
Managements
Stabilize patient from potential lethal conditions, nutritional support, then refer to a mental health
professional with specific expertise in this area.
Bulimia Nervosa
Diagnostic criteria (DSM IV)
A. มีการรับประทานอย่างมากเป็นระยะๆ ซึ่งมีลักษณะ
(1) มีช่วงที่รับประทานอาหารครั้งละมากกว่าที่คนทั่วไปจะบริโภคได้ในเวลาเท่ากัน และในถานการณ์ที่คล้ายคลึง
กัน ใน 2 ชั่วโมง
(2) ควบคุมการรับประทานไม่ได้ในระหว่างนั้น
B. มีการชดเชยป้ องกันน้าหนักขึ้นในลักษณะที่ไม่เหมาะสมเป็นระยะๆ เช่น ทาให้ตนเองอาเจียน ยาระบาย หรือยาอื่น
อย่างไม่เหมาะสม อดอาหาร หรือ ออกกาลังกายอย่างหักโหม
C. ทั้งสองพฤติกรรมเกิดขึ้นเฉลี่ยอย่างน้อยสัปดาห์ละ 2 ครั้งมา 3 เดือน
D. มีความหมกมุ่นไม่พอใจในน้าหนักตัว หรือรูปร่างอย่างมาก
E. ความผิดปกตินี้ไม่ได้เกิดเฉพาะในช่วง ของ Anorexia Nervosa เท่านั้น
Purging Type : มักทาให้ตนเองอาเจียน ใช้ยาระบาย ยาขับปัสสาวะ หรือยาสวนถ่ายเป็นประจา
Nonpurging Type : มีพฤติกรรมชดเชยที่ไม่เหมาะสมอื่นเป็นประจา เช่น อดอาหาร หรือออกกาลังกายอย่างหักโหม
โดยไม่มีพฤติกรรมของ Purging Type
Other important medical history
Medical complications เช่น ปวดท้อง เลือดในอาเจียน ใน upper GI tear, ใจสั่น อ่อนเพลียกล้ามเนื้อกระตุก ใน
electrolyte imbalance, Paresthesias, tetany, seizures or cardiac arrhythmias ใน metabolic complications
เป็นต้น
397.
Psychiatry, 397
Survival forall draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Differential diagnosis
Anorexia, hyperthyroid, DM type1, child/sexual abuses
Consider: Cluster B personality disorder, brain tumors, depression, epileptic seizures, OCD, upper
gastrointestinal disorders, body dysmorphic disorder, psychogenic vomiting, increased intracranial
pressure, anxiety disorder, substance abuse, medications - lithium, tricyclic antidepressants,
neuroleptics, insulin, opiates
Physical examination
GA: พบได้ทั้ง overweight, underweight, หรือ normal body weight ถ้า underweight มากอาจดูคล้าย anorexia
แต่จะมีประวัติน้าหนักขึ้นๆลงๆ
V/S: hypothermia, hypotension
HEENT: dental erosion, palatal trauma, painless enlargement of parotid glands
CVS: bradycardia
GI: diffuse pain upon palpation
Extremities:
- metacarpal phalangeal bruises, calluses, scarring, abrasions (Russell sign)
- edema ถ้ามี laxatives or diuretics abuses
- Proximal muscle weakness, waddling gait ถ้ามี ipecac abuses (เป็น emetic)
Investigations: เลือกตามความเหมาะสม
Electrolyte ถ้ามี dehydration หรือ electrolyte imbalances: K, Mg, Cl , BUN
U/A: dehydration, infection
Drug screen ใน patients with possible drug use.
อาจพบ abnormal endocrine findings: dexamethasone suppression test +, basal serum prolactin
EKG ใน ipecac abuse, hypokalemia, arrhythmia
Gastric motility studies ในรายที่เป็น bulimia มานาน, ท้องผูก, unexplained abdominal pain
ถ้าสงสัย ipecac abuse:
Stool and urine for emetine (byproduct of ipecac)
Cardiac assessment - Muscle enzyme values, lipid levels, Mg, Zn, EKG
Management
Stabilize patient from potential lethal condition then refer to a mental health professional with specific
expertise in this area
Palliative Care, 428
การดูแลผู้ป่วยแบบประคับประคอง (Palliative care)
Palliative care คือ (WHO definition 2010)
ควร
สื่อกับผู้ป่วยว่า “แม้ไม่มีทางรักษาให้หายขาดแต่มีคุณภาพชีวิตที่ดีได้”
แต่ไม่ใช่ รักษาไม่ได้,หมดทางรักษา(ทาให้เกิดการท้อแท้ หมดหวัง)
การประเมินผู้ป่ วยระยะสุดท้าย
1. ประเมินความเข้าใจต่อภาวะความเจ็บป่วยของผู้ป่วยต่อโรคที่เป็น (patient’ s idea)
2. ประเมินความเข้าใจต่อภาวะความเจ็บป่วยของครอบครัวต่อโรคที่ผู้ป่วยเป็น (family’ s idea)
3. ระยะของโรคและอาการที่ผู้ป่วยเป็น
4. ความทุกข์ทรมานของผู้ป่วย
5. ภาระที่ผู้ป่วยยังไม่ได้ทา หรือยังทาไม่สาเร็จ(unfinished business)
6. ภาระของครอบครัวและความลาบากของผู้ดูแล (care giver burden)
7. การวางแผนการดูแลรักษาล่วงหน้า การทาพินับกรรมชีวิต (living will)
a. การรักษาทางกาย
b. การทาพินัยกรรมชีวิต (ถ้าผู้ป่วยหมดสติ จะให้ใครเป็นคนตัดสินใจ)
เป้ าหมายการดูแลผู้ป่ วยแบบประคับประคอง (Palliative care)
เป้ าหมายการดูแล
สาหรับผู้ป่วย : ลดอาการและภาวะแทรกซ้อน, เพิ่มคุณภาพชีวิต, ยอมรับภาวะที่เป็น
สาหรับครอบครัว : ลดความกังวลมีทักษะการรับมือปัญหาการดูแล terminal stage
Supportive care(รักษาตามอาการ)ไม่เท่ากับPalliative careซึ่งเป็น active care คือต้องเริ่มดูแลแต่ต้นที่วินิจฉัย ไม่
จาเป็นต้องรอจนสิ้นสุดการรักษาโรคครอบคลุมทุกด้าน คาดการณ์ไว้ล่วงหน้าก่อนว่าจะเกิดอาการอะไรบ้าง ไม่ใช่
429.
Palliative Care, 429
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
รักษาทีหลัง เฉพาะบุคคลและครอบครัว
ประเด็นสาคัญที่ควรประเมิน (holistic evaluation)
ใช้ตัวย่อช่วยจาว่า : LIFESS
(ไม่จาเป็นต้องซักตามลาดับ หรือได้ครบในครั้งแรก แต่ควรติดตามให้ได้ทั้งหมดในการดูแลระยะยาว)
holistic evaluation “ LIFESS”
Living will
: CPR
CPR+2ท่อ(ET,NG)+3เส้น(ATB,IV,transfusion)
POA, Place of death
Request (unfinish business, 3 wishes)
Individual beliefs
: HOPE
H=hope&resource
of hope
O = organized
religion
P = personal
beliefs
E = expectation
Function ADL, PPS score
Emotion&coping ประเมินตามKubler-Ross 'stage
Suffering & symptom S = social & support
L = living will :ค้นหา goal of careประกอบด้วย 3 ประเด็นหลัก (ตัวย่อช่วยจา : CPR)
C = CPR, 2ท่อ 3เส้น= วิธีการรักษาต่างๆเมื่ออาการแย่ลง อยากให้ดูแลรักษาอย่างไร
โดยเฉพาะที่เกี่ยวกับ: การCPR 2ท่อ= ET & NG tube, 3 เส้น= IV,transfusion,ATB
P = Place of death=สถานที่ที่ต้องการรับการรักษาและเสียชีวิต เช่น บ้านหรือโรงพยาบาล
POA (Power Of Attorney) = คนตัดสินใจแทน, ค้นหาบุคคลที่ผู้ป่วยมอบหมายให้ตัดสินใจ
เรื่องการรักษาพยาบาลแทน เมื่อผู้ป่วยตัดสินใจเองไม่ได้
R = Requests = สิ่งคั่งค้างที่ผู้ป่วยยังไม่ได้ทา (unfinished business) หรืออยากทา (wishes)ใช้เทคนิค 3 wishesก็
ได้
430.
Palliative Care, 430
Survivalfor all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
เทคนิคการขอพร 3 ประการ(3 wish) : สมมติมีพรวิเศษ 3 ข้อ ผู้ป่วยอยากขออะไร แล้วดูคาตอบที่ได้ มัก
ช่วยให้เห็น การรับรู้ต่อระยะโรคของผู้ป่วยช่วยสื่อสารความต้องการ(unfinished business)ช่วยให้ทีมตั้งเป้ าหมายได้
ตรงความต้องการผู้ป่วยมากขึ้น
I = individual beliefsประกอบด้วย
H = hope and resource of hope: มีความหวังอะไรอยู่บ้าง อะไรเป็นกาลังใจสาคัญต่อการมีชีวิต
O = organized religion: ศาสนาที่นับถือและความเชื่อของศาสนาที่มีต่อการเจ็บป่วย
P = personal beliefs: ความเชื่อการรับรู้ของผู้ป่วยที่เกี่ยวกับความเจ็บป่วยความตาย และชีวิตหลังความตาย
E = expectation: มีความคาดหวังอะไรบ้างจากทีมที่ดูแลหรือคนรอบข้าง
F = function = ADLs (activities of daily livings), ระดับความสามารถในกิจวัตรประจาวันหรือ ระดับการดูแลที่ใช้(อาจใช้
เครื่องมือ PPS*ช่วยประเมินและบอก prognosis)
E =emotion and copingของผู้ป่วยและครอบครัวขณะนั้น
ปฏิกิริยาที่เกิดขึ้นเมื่อผู้ป่วยและครอบครัวรับรู้ข่าวร้าย
(Kubler-Ross 'stage) มี 5 ระยะ คือ
ระยะ ลักษณะอารมณ์/พฤติกรรม การ approach
1. ตกใจและปฏิเสธ(shock & denial) “ไม่จริง หมอโกหก”
- ไม่เข้าใจ/ยอมรับกับข้อมูลที่แพทย์
อธิบายให้
-รับฟัง empathy
-ระวังผู้ป่วยอาจยังรับข้อมูลไม่ได้
ทั้งหมด ควรให้เท่าที่จาเป็นก่อน
2. โกรธ (anger) “ทาไมต้องเป็นฉันด้วย”
-รู้สึกโกรธ โทษตัวเองหรือโกรธว่าการ
รักษาล่าช้า
รับฟัง empathy
-ระวังการรู้สึกไม่พอใจผู้ป่วยกลับของ
แพทย์ ควรเข้าใจว่าเป็นปฏิกิริยาต่อ
ข่าวร้าย ไม่ใช่ต่อแพทย์จริงๆ
3. ต่อรอง (bargaining) “มันอาจจะหายถ้าฉัน…”
- พยายามหาวิธีต่างๆมาช่วยรักษา
- หรือสร้างเงื่อนไขในการรักษา
ต่างๆ
-ทาความเข้าใจและยอมรับ ว่าเป็น
ทางเลือกหนึ่งตามความหวังที่มี
-หากไม่สิ้นเปลืองหรือมีผลร้ายต่อ
ผู้ป่วยควรอานวยความสะดวกใน


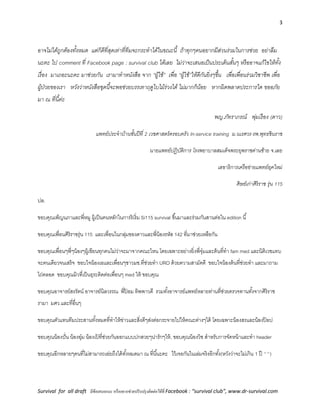


















































































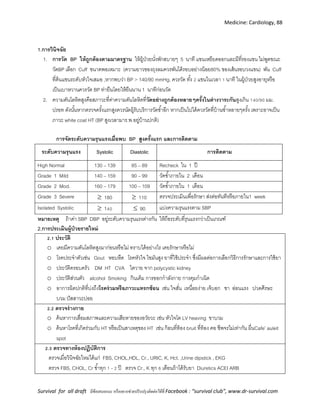





























![Medicine: Chest, 118
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Spirometry
o Obstructive :FEV1 จะลดมากกว่า FVC ค่า FEV1/FVC ratio < 70%
o Reversibility : หลังพ่น bronchodilator ค่า FEV1 เพิ่มขึ้น >200 ml และ >12%
o Restrictive : FEV1 และ FVC ลดลงในสัดส่วนที่ใกล้เคียงกันดังนั้น FEV1/FVC ratio จะปกติ ( 70%) และค่า FVC ≤
80% predicted
Community-acquired pneumonia (CAP)
Symptoms Signs Investigations
- Fever
- Cough
- Dyspnea
- Pleuritic chest pain
- Fine crackles
- Signs of consolidation or pleural
effusion
- CBC: leukocytosis
- Chest x-ray : consolidation,
infiltrates, effusion
- Sputum G/S and Culture
- Hemoculture
การจาแนกความรุนแรง ทาได้หลายวิธี
1. CURB-65 score : confusion, urea (BUN) > 20 mg/dl, RR 30, BP < 90/60, Age 65
(score 0-1 : outpatient, 2 : admit to IPD, 3 : admit to ICU)
2. ATS guideline (2004) : ICU admission (1 major or 2 minor)
Major : mechanical ventilation, septic shock
Minor : SBP ≤ 90, multilobar disease, SpO2 < 90% or PaO2/FiO2 < 250
3. IDSA guideline (1995) : PSI scoring system
Management
OPD IPD : non-ICU
1. Previously healthy and no ATB in past 3 mo
- Clarithromycin (500 mg) PO bid x 5 days
[or] Azithromycin (500 mg) PO once,
then 250 mg OD x 4 d
[or] Doxycycline (100 mg) PO bid x 7-10 d
2. Comorbidities or ATB in past 3 mth
1.1 Levofloxacin 750 mg PO OD
[or] High-dose amoxicillin 1 g tid
[or] Amoxicillin/clavulanate 2 g bid หรือ
1. Levofloxacin (750 mg) PO or IV OD หรือ
2. Cefotaxime (1–2 g) IV q 8 hr
[or] Ceftriaxone (1–2 g) IV OD
[or] Ampicillin (1–2 g) IV q 4–6 hr
Plus
Clarithromycin (500 mg) PO bid
[or] Azithromycin 500 mg PO once,
then 250 mg OD
[or] Azithromycin 1 g IV once,
then 500 mg OD](https://image.slidesharecdn.com/qjnirmqqkwitowjue5vg-signature-8778b5cc48d093758c78950a2029edcc14e324f73053c732e914a05b6e9f543b-poli-160514181421/85/Survival-new-118-320.jpg)
![Medicine: Chest, 119
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
1.2Ceftriaxone 1–2 g IV OD
[or] Cefpodoxime 200 mg PO bid
[or] Cefuroxime 500 mg PO bid
plus Macrolides
2. สาหรับผู้ป่วย ICU และ special case เช่น
Pseudomonas และ CA-MRSA pneumonia แนะนาให้
ปรึกษาแพทย์ระบบทางเดินหายใจและโรคติดเชื้อร่วม
ประเมินและให้การรักษา
Health care-associated pneumonia (HCAP)
clinical as pneumoniaแบ่งเป็น
- Hospital-acquired pneumonia (HAP) เกิดหลังadmit 48 hr
- Ventilator-associated pneumonia (VAP) เกิดหลัง on ETT 48 hr
- Empiric broad-spectrum ATB in first 3-5 days
- Deescalator ATB ปรับลด spectrum ตาม sputum C/S & sensitivity
Management
ATB selection ( ATS guideline 2005) พิจารณาจาก
1.onset : early HAP in first 4 days
- late HAP admit ≥5 days สัมพันธ์กับการติดเชื้อดื้อยาและ poor prognosis
2.Risk for MDR pathogens
- Antimicrobial therapy in preceding 90 d
- Current hospitalization of 5 d or more
- High frequency of antibiotic resistance in the community or
in the specific hospital unit
- Presence of risk factors for HCAP :
o Hospitalization for 2 d or more in the preceding 90 d
o Residence in a nursing home or extended care facility
o Home infusion therapy (including antibiotics)
o Chronic dialysis within 30 d
o Home wound care
o Family member with multidrug-resistant pathogen
o Immunosuppressive disease and/or therapy
Initial empiric therapy
a. Early onset or low risk MDR : H. influenzae, S. pneumoniae, MSSA, ATB-sensitive gram neg bacilli –E.coli, K.](https://image.slidesharecdn.com/qjnirmqqkwitowjue5vg-signature-8778b5cc48d093758c78950a2029edcc14e324f73053c732e914a05b6e9f543b-poli-160514181421/85/Survival-new-119-320.jpg)

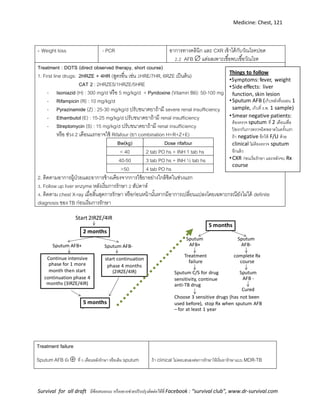






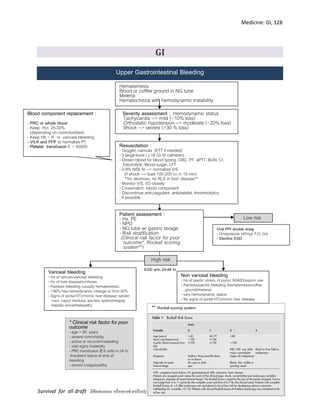








![Medicine: GI, 137
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
พยาธิใบไม้ในตับ : รับประทาน 10 mg/Kg เป็นเวลา 7 วัน
3. Thiabendazole พยาธิตัวกลมในลาไส้ชนิดต่างๆ : 25 mg/Kg วันละ 2 ครั้ง เป็นเวลา 2 วัน
4. Pyrantel pamoate พยาธิปากขอ พยาธิไส้เดือน พยาธิเข็มหมุด โดยขนาดที่ใช้ คือ 11 mg/Kg ครั้งเดียว
5. Piperazine พยาธิไส้เดือน และพยาธิเข็มหมุด โดยขนาดที่ใช้ คือ 75 mg/Kg วันละครั้ง ติดต่อกัน 2 วัน
6. Praziquantel
พยาธิใบไม้ : รับประทาน 20 mg/Kg โดยให้ 2-3 ครั้ง ห่างกัน 4 – 6 ชั่วโมง
พยาธิตัวตืด : รับประทาน 10 – 20 mg/Kg ครั้งเดียว
7. Niclosamide พยาธิตัวตืด โดยให้รับประทาน ครั้งเดียวในขนาด 2 กรัม
ยาพยาธิแบบน้า
Mebendazole แบบน้า
สาหรับเด็ก 2-15 ปี 1 tsp x 2
พยาธิตัวกลม ให้ 1 วัน ,พยาธิตัวแบน ให้สามวัน
สาหรับเด็ก 1-2 ปี 1/2 tsp x 2
พยาธิตัวกลม ให้ 1 วัน ,พยาธิตัวแบน ให้สามวัน
Albendazole แบบน้า
สาหรับเด็ก 1-2 ปี Alben 200 mg PO single dose
สาหรับเด็ก 2-15 ปี Alben 400 mg PO single dose
Irritable Bowel Syndrome
Clinical presentation
-Chronic gastrointestinal disorder of unknown cause.
-Common symptoms include abdominal cramping or pain, bloating and gassiness, and altered bowel habits
-Patient has comorbid psychiatric disorders [depression, anxiety]
-The hallmark of IBS is abdominal discomfort or pain. The following symptoms are also common
-The Rome III Criteria : a patient should have suffered abdominal pain or discomfort for 12 weeks or more (not
necessarily consecutive weeks) in the previous 12 months. The pain or discomfort should have two out of the
three following features:](https://image.slidesharecdn.com/qjnirmqqkwitowjue5vg-signature-8778b5cc48d093758c78950a2029edcc14e324f73053c732e914a05b6e9f543b-poli-160514181421/85/Survival-new-137-320.jpg)
![Medicine: GI, 138
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Relief with defecation
Onset associated with a change in the frequency of stool
Onset associated with a change in the form of stool
Differential diagnosis
-clinical diagnosis
-Ix to R/O other GI causes ex. CBC,TSH, Electrolyte, Stool
exam, Abdominal film, Barium enema, GI scope Supporting
symptoms
1) abnormal frequency of stools (more than 3/day or less than
3/week)
2) abnormal stool form (lumpy and hard, or loose and watery)
3) abnormal stool passage (straining, urgency, or feeling of
incomplete evacuation)
4) passage of mucus
5) bloating (feeling of abdominal distention, or enlargement).
Management
-Counseling: reassure Pt. เพื่อคลายความกังวลและให้ Pt มั่นใจว่าไม่ได้เป็นโรคร้ายแรง
-Dietary: fiber supplement [psyllium], avoid food that worsen symptoms eg.fat,bean,cabbage,clauliflower
-Medications:
1. Anti-diarrheal drug-> Loperamide[imodium] 4 mg (2 capsules) as a first dose, followed by 2 mg (1 capsule)
after each unformed stool. The maximum dose is 16 mg/day.
2. Anti-spasmodic drugs->
2.1 dicyclomine (Bemote, Bentyl, Di-Spaz) 20 mg given 2-4 times daily.
S/E:dry mouth, blurred vision, confusion, agitation, increased heart rate, heart palpitations, constipation, difficulty
urinating
2.2 hyoscyamine (Levsin, Levbid, NuLev)May be taken with or without food. The dosage is adjusted to the
individual patient to assure control of symptoms with a minimum of side effects.
S/E:dry eyes, dry mouth and urinary hesitancy and retention. Blurred vision, rapid heart rates, palpitations
3. Psychiatrics drug:
TCA->amitriptyline 10-25 mg po hs in divided doses. S/E:SIDE EFFECTS:fast heart rate, blurred vision, urinary
retention, dry mouth, constipation, weight gain or loss, and low blood pressure](https://image.slidesharecdn.com/qjnirmqqkwitowjue5vg-signature-8778b5cc48d093758c78950a2029edcc14e324f73053c732e914a05b6e9f543b-poli-160514181421/85/Survival-new-138-320.jpg)






![Medicine: GI, 145
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Pyogenic Liver Abscess
History Clinical Presentation Investigation
Hematogenous spread or local
spread from infection within
peritoneal cavity: appendicitis,
diverticulitis, penetrating trauma. (
เชื้อ : E. coli, Klebsiella, Proteus,
Enterococcus, Anaerobes)
- non specific
- fever
- wt loss
- malaise
- nausea/vomiting
- 50% มี hepatomegaly ,RUQ
tender,janudice
- ALP , +/- abn.LFT
- CBC: Leukocytosis
- Round or oval defects on U/S, CT
scan , MRI
- CXR : อาจพบ new elevation of Rt.
hemidiaphragm,Rt. basilar
infiltration,Rt. pleural effusion
Management
- Empirical ATB: Cefoxitine (2g) IV q 4-6 hr.
- Percutaneous or surgical drainage
- Specific ATB depend on G/S and C/S
Amebic liver abscess
History Clinical Presentation Investigation
- Homosexual men
- ติดต่อทาง Fecal-oral hepatic
portal vein liver abscess
- non specific
- fever
- wt loss
- malaise
- nausea/vomiting
- hepatomegaly, RUQ
tenderness, diarrhea
- CBC : Leukocytosis
- LFT often elevate
- 90% positive serologic tests ( IgG
immunoassay)
- Round or oval defects on U/S , CT
scan , MRI (more commonly single)
- CXR : ~ pyogenic
U/S : Amoebic liver abscesses are usually single but can be multiple. Typical location is in the right lobe of liver
subcapsular close to the diaphragm and posterolateral, though it can be situated in any location. The size of an
abscess may vary from few centimeters to a large size occupying almost entire right lobe of liver
Picture1. Early abscess [1]. Picture2](https://image.slidesharecdn.com/qjnirmqqkwitowjue5vg-signature-8778b5cc48d093758c78950a2029edcc14e324f73053c732e914a05b6e9f543b-poli-160514181421/85/Survival-new-145-320.jpg)

















![Medicine: Nephrology, 163
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Hypovolemic ใช้ NSS เพื่อแก้ ECF volume ก่อนในระยะแรกแล้วจึงให้ 0.45% NaCl หรือ 5% dextrose เพื่อแก้ภาวะ
ขาดสารน้า
Euvolemic ให้ดื่มน้าเพิ่มขึ้นทางปากก่อนพิจารณาให้ hypotonic fluid ได้แก่ 5% D/W
Hypervolemic พิจารณาให้ loop diuretic เพื่อเพิ่มการขับ Na ออกทางไต หลังจากนั้นอาจให้ 5%DW ทดแทน ถ้าไตไม่
ทางานอาจจะต้องทา dialysis
สามารถคานวณการเปลี่ยนแปลงของระดับ sodium ในเลือด โดยใช้สูตร
Change in serum [Na] = infusate[Na+K] - serum[Na]
Total body water + 1
หรือ water deficit(L) = total body water x (1 - current plasma[Na])
140
Long term management (cause dependent)
-ให้ปริมาณน้าดื่มเพียงพอในผู้ป่วยที่เสี่ยงต่อการขาดน้า รวมทั้งโปรตีนและเกลือ
-แก้ไขภาวะที่อาจทาให้เกิด transient nephrogenic DI เช่น hypercalcemia, hypokalemia รวมทั้งการงดใช้ยาที่มีผลต่อการขับน้าที่ไต
-พิจารณาให้ยาขับปัสสาวะ thiazide ขนาดต่า ในผู้ป่วย nephrogenic DI
-ให้ฮอร์โมน vasopressin ทดแทนในผู้ป่วย neurogenic DI (ให้การรักษาทางจิตเวช ในผู้ป่วยที่มีปัญหา psychogenic polydipsia ไม่
เกี่ยวกับ hypernatremia แต่มี polyuria ได้)](https://image.slidesharecdn.com/qjnirmqqkwitowjue5vg-signature-8778b5cc48d093758c78950a2029edcc14e324f73053c732e914a05b6e9f543b-poli-160514181421/85/Survival-new-163-320.jpg)




![Medicine: Nephrology, 168
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Hypercalemia
Diagnosis : ได้จากการตรวจพบ Serum Ca > 10 mg /dL โดยค่า Ca ที่ได้จะต้องทาการ correct กับค่าของ albumin ในเลือดเสียก่อน จาก
สูตรต่อไปนี้
Corrected [calcium] (mg/dL) = Measured [calcium] (mg/dL) + 0.8 (4.0 - [albumin] (g/dL))
Cause :
1. Endocrinopathies : Hyperparathyroidism , Paget’s disease of the bone , Addison’ disease
2. Malignancies : Metastatic cacser ( Bone metastasis) , multiple myeloma , tumors that release PTH-like
hormone (lung cancer)
3. Pharmacologic : Vitamin D intoxication , calcum carbonate, milk , drug (thiazide diurtics, lithium
4. Other : Sarcoidosis , familial hypercalciuric hypercalcemia
Sign and symptom
1. Stones : นิ่วในไต
2. Bones : bone pain , osteitis fibrosa cystica ( pathologic fracture)
3. Grunts and groans : muscle weakness , pancreatitis , PU , gout, constipation
4. Psychiatric overtone : depression , fatigue, anorexia, sleep disturbances ,anxiety , lethargy
5. Other : polydipsia, polyuria, HT , weight loss, shortening QT interval in EKG
Treatment
1. Hydration : NSS 4-5 L
2. Increased calcium excretion : loop diuretic (lasix)
3. Inhibit bone resorption
a. Bisphosphonates (pamidronate)
b. Calcitonin
4. Steroid : lymphoma , multiple myeloma
5. Hemodialysis](https://image.slidesharecdn.com/qjnirmqqkwitowjue5vg-signature-8778b5cc48d093758c78950a2029edcc14e324f73053c732e914a05b6e9f543b-poli-160514181421/85/Survival-new-168-320.jpg)





















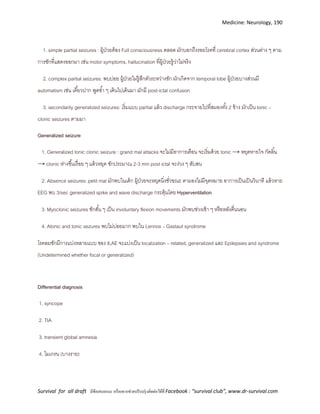




![Medicine: Neurology, 195
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
2. ส่งตรวจ CT scan หากมี indication ดังต่อไปนี้:
Immunocompromised state = HIV, receiving immunosuppressive therapy, or after transplantation
History of CNS disease = Mass lesion, stroke, or focal infection
New onset seizure =Within 1 week of presentation; some authorities would not perform a lumbar
puncture on patients with prolonged seizures or would delay lumbar puncture for 30min in patients
with short, convulsive seizures
Papilledema
Abnormal level of consciousness …
Focal neurologic deficit = dilated nonreactive pupil, abnormalities of ocular motility, abnormal visual
fields, gaze palsy, arm or leg drift
- ถ้ามีลักษณะดังกล่าว ให้ take H/C, start dexamethasone (ดูข้อ 4) and empirical antibiotic แล้วส่งผู้ป่วยไป CT
- หากผล CT ไม่มี mass effect ให้ทา lumbar puncture ได้ (ดูข้อ 3)
3. หากไม่มี indication ดังในข้อ 2 แล้ว
- ให้เจาะเลือดเพื่อส่ง CBC, serum glucose, +/- Hemoculture, etc.
- ทา lumbar puncture, อธิบาย+เตรียมผู้ป่วย; LP วัด open & closed pressure, ดูความขุ่นของ CSF [หาก open
pressure > 25 cmH2O = High-risk for herniation; Start mannitol then consult neurosurgery]
- ส่ง CSF เพื่อตรวจ (1) C/S, G/S (2) glucose, protein (3) cell count & diff (4) เก็บไว้ตรวจ Gram stain เอง (5) หรือ
ตรวจเพิ่มพิเศษทางห้องปฏิบัติการอื่นๆ
- ย้อม Gram stain เอง หากพบเชื้อให้พิจารณาร่วมกับประวัติ ว่านึกถึงเชื้อใดมากที่สุด และให้ specific antibiotic แต่
หากไม่พบเชื้อ ให้ start empirical antibiotic แล้วคอยติดตามผลเพาะเชื้อ
4. การให้ dexamethasone อาจช่วย improve outcome & survival rate โดยเฉพาะใน community-acquired bacterial
meningitis
- Dose: 0.15 mg/kg หรือ 10 mg IV q 6 hr x 4 days ให้ในช่วง 10-20 นาทีก่อนให้ antibiotic หรือพร้อม antibiotic
(เน้นโดยเฉพาะ dose แรก หากให้หลังจากนี้อาจจะไม่มีประโยชน์)](https://image.slidesharecdn.com/qjnirmqqkwitowjue5vg-signature-8778b5cc48d093758c78950a2029edcc14e324f73053c732e914a05b6e9f543b-poli-160514181421/85/Survival-new-195-320.jpg)


































![Medicine: Endocrinology, 230
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
- แก้ไขสาเหตุของ DIC
- supportive treatment : oxygen, IV fluids, maintain BP & renal perfusion
- ให้ FFP (all factors.), platelet, cryoprecipitate (f. VIII, XIII, vWF, fibrinogen, fibronectin)
Keep fibrinogen > 100 mg/dL
- ถ้ามีอาการของ thrombosis รุนแรง อาจให้ heparin ร่วมด้วย (controversial)
2. Hemophilia
แบ่งเป็น Hemophilia A (พบบ่อยกว่า) ขาด factor VIII และ Hemophilia B ขาด factor IX
History Physical examination Investigation
เลือดออกง่าย – หยุด
ยาก, มีประวัติใน
ครอบครัว โดยเฉพาะ
ญาติผู้ชาย (XR)
- anemia จาก bleeding
- hemarthroses, intramuscular hematomas,
hematuria, hemospermia, intracranial
bleeding, retroperitoneal bleeding
- delayed post-traumatic or post-operative
bleeding
- aPTT : prolonged
- factor VIII (hemophilia A) or
factor IX (hemophilia B)
activity level : low (<1% =
severe, 1-5% = moderate, 5-
25% = mild)
Managements :
- สาหรับ hemophilia A : mild – moderate หรือ minor bleeding episode สามารถใช้ DDAVP โดยจะเพิ่ม factor VIII
level ได้ 3-5 เท่าใน 30 นาที [DDAVP : 0.3 mcg/kg SC หรือ dilute in 50–100 ml NSS IV drip in 30 min, repeat q
12 hrs.], DDAVP ไม่ได้ผลใน hemophilia B
- ให้ factor replacement โดยพิจารณาดังนี้
1. ประเมินระดับ factor ที่ต้องการ
- Life-threatening hemorrhage or major surgery เช่น ICH, retropharyngeal, retroperitoneal
hemorrhage, active GI bleeding, ophthalmic trauma or hemorrhageต้องการ 80 – 100 %
- Major bleeding or minor surgery เช่น active oral bleeding, persistent hematuria, tooth extraction
ต้องการ 50 – 80 %
- Mild bleeding or minimally invasive surgery เช่น early hemarthrosis, intramuscular hematoma (ที่ไม่ใช่
iliopsoas m.) ต้องการ 30 – 40 %
2. คานวณปริมาณ factor ที่จะให้
- factor VIII 1 U / kg เพิ่มระดับ factor VIII ได้ 2 %, half-life 12 ชม.
- factor IX 1 U / kg เพิ่มระดับ factor IX ได้ 1 %, half-life 24 ชม.](https://image.slidesharecdn.com/qjnirmqqkwitowjue5vg-signature-8778b5cc48d093758c78950a2029edcc14e324f73053c732e914a05b6e9f543b-poli-160514181421/85/Survival-new-230-320.jpg)



![Medicine: Endocrinology, 234
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
4. Lymphoma
(Non-Hodgkin’s [NHL] พบบ่อยกว่า Hodgkin’s [HL] 2 เท่า)
Clinical presentations
1. ต่อมน้าเหลืองโตเร็ว ไม่เจ็บ
2. อาการของ extranodal involvement เช่น ปวดท้อง, แน่นท้อง, ปวดกระดูก
3. B symptoms (พบใน HL > NHL) : ไข้, เหงื่อออกกลางคืน, น้าหนักลด
4. ถ้ามี bone marrow involvement อาจมาด้วยอาการของ pancytopenia
ผู้ที่มีปัจจัยต่อไปนี้มีความเสี่ยงต่อ lymphoma มากขึ้น (โดยเฉพาะ NHL)
- HIV/AIDS
- immunosuppression
- viral infection บางชนิด เช่น EBV, HTLV-1
- ยา, สารเคมี, รังสี
- primary immunodeficiency
- autoimmune diseases
Physical examination
HL : painless lymphadenopathy ที่ cervical, supraclavicular, axillary, mediastinum
มักกระจายเรียงตาม lymph node ที่ต่อกัน ไม่ข้าม node (contiguous spread)
NHL : painless, firm, mobile lymphadenopathy ที่ supraclavicular, cervical, axillary
มักกระจายไปยัง node ที่ไม่ต่อเนื่องกัน, มี extranodal involvement
Investigation
- lymph node biopsy (ไม่ควร FNA เนื่องจากต้องอาศัยลักษณะโดยรอบของ lymph node) สามารถบอก definite
diagnosis ได้ (HL พบ Reed Sternberg Cell, NHL ไม่พบ)
โดย lymph node ที่มีขนาด > 1 cm นาน 4 สัปดาห์ขึ้นไป ที่ไม่ได้เกิดจาก infection ควรได้รับการ biopsy
- CBC ควรทาก่อนเพื่อช่วยแยก acute leukemia เนื่องจากทาให้ lymph node โตได้เหมือนกัน
- LDH, alkaline phosphatase สูง ทาให้นึกถึง bone or liver involvement
- liver function test หรือ bilirubin ที่สูง ทาให้นึกถึง liver involvement
- CXR อาจพบ hilar หรือ mediastinal lymphadenopathy
- CT scan (chest,abdomen) เพื่อหา lymph node involvement
- electrolytes, calcium, phosphate, uric acid, BUN, creatinine
- bone marrow aspiration / biopsy : จาเป็นสาหรับ NHL ทุกรายเนื่องจากมี BM involvement มาก แต่ HL ควรทาใน
บางระยะของโรคเท่านั้น](https://image.slidesharecdn.com/qjnirmqqkwitowjue5vg-signature-8778b5cc48d093758c78950a2029edcc14e324f73053c732e914a05b6e9f543b-poli-160514181421/85/Survival-new-234-320.jpg)



























































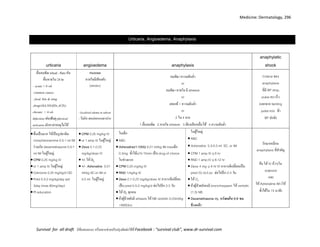



























![Medicine: Nutrition , 324
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
NUTRITION (for adult)
Estimation of caloric requirements
Basal Energy Expenditure : Harris-Benedict equation (kcal/d)
Men: 66.4 + [13.7 × weight (kg)] + [5 × height
(cm)] – [6.8 × age (years)]
หรือคิดโดยประมาณโดยใช้สูตร Men: 900 + [10
× weight (kg)]
Women: 655 + [9.6 × weight (kg)] + [1.7 ×
height (cm)] – [4.7 × age (years)]
หรือคิดโดยประมาณโดยใช้สูตร Women: 700 +
[7 × weight (kg)]
เมื่อได้ BEE แล้ว นาไปคูณด้วย Stress factor และ Activity
factor จะได้ค่าพลังงานที่ร่างกายต้องการที่ใกล้เคียงความเป็นจริงมากขึ้น
Estimates of protein requirements
Clinical conditions Protein (g/kg/day)
Healthy, non-stressed 0.8-1.0
Mild metabolic stress (elective hospitalization) 1.0 - 1.1
Moderate metabolic stress (complicated postop. care, infection) 1.2 - 1.4
Activity factor : multiplying by 1.2 for sedentary, 1.4 for moderately active, or
1.8 for very active individuals 0.7-0.9 for case on respirator](https://image.slidesharecdn.com/qjnirmqqkwitowjue5vg-signature-8778b5cc48d093758c78950a2029edcc14e324f73053c732e914a05b6e9f543b-poli-160514181421/85/Survival-new-324-320.jpg)
































































![Psychiatry, 392
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Attention Deficit Hyperactivity Disorder (ADHD)
Causes
-genetics
-bio: frontal lobe ทางานผิดปกติ
-psychosocial:ไม่ได้ทาให้เป็นโรคแต่ทาให้อาการเด่นชัดรุนแรงขึ้น
Comorbidity พบได้ 2/3 เช่น OCD, conduct d/o, mood d/o, anxiety d/o
Diagnosis
1.inattention ขาดสมาธิ
2.hyperactivity ซน-ไม่อยู่นิ่ง
3.impulsivity หุนหันพลันแล่น
เป็นนานกว่า 6 เดือน, เป็นก่อนอายุ7ปี, ≥2เหตุการณ์, ผลต่อการเข้าสังคม การเรียน การงาน,
R/O โรคระบบประสาท lead poisoning, hyperthyroidism เป็นต้น
Classification
1.combined
2.hyperactive/compulsive
3.inattentive
Managements [multiple-modality approach]
Psycho-social
1.Parent management trainingให้ความรู้ว่าเป็นความผิดปกติของสมอง เด็กคุมตนเองไม่ได้ สอนการจัดการหรือปรับ
พฤติกรรมไม่พึงประสงค์โดยไม่ลดคุณค่าเด็ก เช่น จัดตารางเวลา, หาที่สงบทางาน, นั่งประกบทางาน, ไม่ตวาด, ตั้ง
กฎเกณฑ์, ลงโทษโดยจากัดสิทธิ์, ชมเชยเวลาทาดี
2.School-focused intervention ให้เด็กนั่งหน้าชั้นไกลประตูหน้าต่าง,หากิจกรรมให้ทาเวลาขาดสมาธิเขียนการบ้านให้
ชัดเจน,ลดเวลางานให้สั้นลงถ้าไม่เสร็จ,ไม่ตาหนิให้อาย,ช่วยด้านการเรียน สอนตัวต่อตัว
3.Child-focused intervention ฝึกทักษะทางสังคมให้สังเกตอารมณ์คนอื่น รู้จักรอคอย รับฟัง เอาใจเขามาใส่ใจเรา รู้อะไร
ควรทา
Bio
1.Stimulant drugs[DOC]: Methylphenidate 0.3-1 MKD pc เช้า เที่ยง[max 60 mg/d,T1/2=2-3hr]
เป็น sympathomimetic
SE:เบื่ออาหาร น้าหนักลด อารมณ์เปลี่ยน ปวดหัว ปวดท้อง คลื่นไส้ ใจสั่น
2.Non-stimulant drugs:
TCA 1-5 MKD, Clonidine 3-5ug/kg/d](https://image.slidesharecdn.com/qjnirmqqkwitowjue5vg-signature-8778b5cc48d093758c78950a2029edcc14e324f73053c732e914a05b6e9f543b-poli-160514181421/85/Survival-new-392-320.jpg)
![Psychiatry, 393
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Learning disorder (LD)
Diagnosis
ผลสัมฤทธิ์ด้านการเรียนต่ากว่าชั้นเรียนจริง 2 ชั้น โดยที่ระดับสติปัญญา (IQ) ปกติ การทดสอบเช่น
- Achievement Test
- แบบทดสอบการเขียน การอ่าน การคานวณ (WRAT test)
- KUS-SI (รร.ใช้แบบทดสอบนี้ในการคัดกรอง)
Classification
1. โรคบกพร่องด้านการอ่าน (Reading disorder)
2. โรคบกพร่องด้านการเขียน (Written expression disorder)
3. โรคบกพร่องด้านคณิตศาสตร์ (Mathematics disorder)
4. Learning disorder not otherwise specified
Managements [multiple-modality approach]
การช่วยเหลือทางการแพทย์ เนื่องจาก LD สามารถเกิดรวมกับโรคอื่นๆได้บ่อย เช่น ADHD ดังนั้นแพทย์จึงมีบทบาทใน
การประเมิน วินิจฉัยภาวะต่างๆที่เด็กมี ร่วมถึงให้การรักษาภาวะเหล่านั้น เช่น โรคสมาธิสั้น หากได้รับยาช่วยสมาธิ
อาการของโรคก็จะดีขึ้นมาก
การช่วยเหลือทางการศึกษา โรงเรียนควรจัดทาแผนการเรียนรายบุคคล เน้นการสอนเสริมในทักษะที่บกพร่อง เช่น การ
สะกดคา อ่าน เขียนสอนเป็นกลุ่มย่อยหรือตัวต่อครั้งละ 30-45 นาที สัปดาห์ละ 4-5 วัน การช่วยอ่านบทเรียนให้ฟัง
เพื่อให้เด็กได้เนื้อหา ความรู้ ได้เร็วขึ้นใน reading D/O การให้เวลาในการทาสอบเพิ่มขึ้น เพื่อให้เด็กมีเวลาเพียงพอใน
การ อ่านโจทย์ และเขียนตอบ จะช่วยให้เด็กเรียนได้ดีขึ้น และควรส่งเสริมทักษะด้านอื่นๆ ที่เด็กสนใจ เช่น ดนตรี กีฬา
ศิลปะ เพื่อให้เด็กเกิดความภาคภูมิใจในตนเอง
การช่วยเหลือจากครอบครัว เปลี่ยนพฤติกรรมจากการตาหนิ ลงโทษ เป็นความเข้าใจ และสนับสนุนในการส่งเสริม
ทักษะการเรียนรู้ของเด็ก ชื่นชมเมื่อเด็กทาสาเร็จแม้ในเรื่องเล็กน้อยเพื่อให้เกิดความภาคภูมิใจในตนเอง](https://image.slidesharecdn.com/qjnirmqqkwitowjue5vg-signature-8778b5cc48d093758c78950a2029edcc14e324f73053c732e914a05b6e9f543b-poli-160514181421/85/Survival-new-393-320.jpg)






![Psychiatry, 400
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Tic Disorders
Cause “multifactorial factors”
genetics
brain:basal ganglia[cortico-striato-thalamocortical circuits]
neurotransmitter:dopamine↑
prenatal:LBW,เครียดตอนตั้งครรภ์
immune:B-hemolytic strep. Infection
Comorbidity: ADHD,OCD,impulsivity,distractibility
History :
abrupt/purposeless/recurrent/stereotyped/partial inhibited
ความถี่เปลี่ยนตาม env./ความรุนแรงไม่คงที่ อาจขึ้นหรือลดลงเอง(waxing&waning) ไม่เป็นตอนหลับ รู้ตัวตอน
เป็น รู้ตัวว่าจะมีอาการ
เป็นก่อนอายุ18ปี
ประกอบด้วย motor/vocal tics
R/O drug, huntington, cerebritis
หายได้เอง เป็นชั่วคราว
Differential diagnosis
1. Psychiatric disorder
Transient tic disorder
-อาการนาน 4wk-1yr
-พบบ่อยสุด ไม่รุนแรง ที่หน้าคอแขน
-ตัวกระตุ้นคือ เครียด ตื่นเต้น
Chronic motor/vocal tic disorder
-อาการอย่างใดอย่างหนึ่งนาน>1yr
-ไม่มีช่วงไม่เป็นต่อกันนานเกิน 3
เดือน
Tourette’s disorder
- multiple motor&vocal tics เป็น
ร่วมกัน
- รุนแรงสุด นานเกิน 1yr
-ไม่มีช่วงไม่เป็นต่อกันนานเกิน 3
เดือน
2. Organic disorder: myoclonus, tremor, chorea, athetosis, dystonia
Managements
Psyco-social
-ให้ความรู้พ่อแม่ว่าเป็นความผิดปกติของสมองบางส่วน ไม่ห้ามปราม ปกป้ องการล้อเลียน ให้ความมั่นใจ
-ร่วมมือกับโรงเรียน
-ให้ผู้ป่วยเข้าใจโรคและปัญหา
-พฤติกรรมบาบัด](https://image.slidesharecdn.com/qjnirmqqkwitowjue5vg-signature-8778b5cc48d093758c78950a2029edcc14e324f73053c732e914a05b6e9f543b-poli-160514181421/85/Survival-new-400-320.jpg)
![Psychiatry, 401
Survival for all draft มีข้อเสนอแนะ หรืออยากช่วยปรับปรุงติดต่อได้ที่ Facebook : “survival club”, www.dr-survival.com
Bio [some case] 2ตัวแรกให้ผลดีสุด
-haloperidol 0.25mg hs SE:ง่วง น้าหนักเพิ่มextrapiramidal SE[ให้benztropineแก้]
-pimozide 1mg hs SE:same+QT prolonged
-risperidone
-clonidine 0.025-0.05 mg/dose เช้า
Child abuse
แบ่งออกเป็น 4 ประเภท
1. Physical abuse การทารุณกรรมทางร่างกาย
2. Sexual abuse การทารุณกรรมทางเพศ
3. Physical abuse การทารุณกรรมทางจิตใจ
4. Neglect การทอดทิ้งเด็ก
หลักในการดูแลเด็กลุ่มนี้
1. Identify เด็กที่น่าสงสัยว่าถูกทารุณกรรม
• การบาดเจ็บที่น่าสงสัยการทารุณกรรมทางร่างกาย: คาอธิบายสาเหตุไม่สอดคล้องกับอาการ
บาดเจ็บ ความล่าช้าในการมาพบแพทย์ ประวัติบาดเจ็บซา้้ๆ รอยฟกช้าตามร่างกาย กระดูกหักหลายที่
• อาการที่น่าสงสัยการทารุณกรรมทางเพศ: ตั้งครรภ์ โรคติดต่อทางเพศสัมพันธ์ พฤติกรรม
แสดงออกทางเพศผิดปกติ อาการหวาดกลัวหรือพฤติกรรมเปลี่ยนแปลงโดยไม่ทราบสาเหตุ การบาดเจ็บของอวัยวะ
เพศ
• อาการบ่งชี้ว่าเด็กอาจถูกทารุณกรรม: เด็กหวาดกลัวผู้ปกครอง เด็กแยกตัวหรือเข้ากับคนง่าย
ผิดปกติ การเจริญเติบโตช้าโดยไม่ได้เกิดจากเป็นโรคเรื้อรัง ผู้ปกครองข่มขู่เด็ก ผู้ปกครองมีอาการทางจิต
2. ประเมินทางร่างกายเบื้องต้น
• ซักประวัติ
• ตรวจร่างกายทุกระบบ: ค้นหาร่องรอยการถูกทาร้าย ตรวจอวัยวะเพศพร้อมเก็บหลักฐานทางนิติเวช
• Investigation: bone survey ในเด็ก<2ปี, CT brain ใน head injury, swab เชื้อโรคติดต่อทางเพศสัมพันธ์,
lab พื้นฐานอื่นๆตามที่เกี่ยวข้องกับการทารุณกรรมที่สงสัย
3. รักษาภาวะทางร่างกาย
4. ประเมินความจาเป็นในการรับไว้ในโรงพยาบาล (ข้อบ่งชี้: มีภาวะทางร่างกานที่ต้องรักษาตัว, มีแนวโน้มถูกกระทาซ้า,มี
ความเสี่ยงต่อความไม่ปลอดภัยอื่นๆ)
5. ในกรณีที่เด็กไม่ปลอดภัยหากกลับไปอยู่กับครอบครัว อาจโทรติดต่อศูนย์ประชาบดีสายด่วน1300 เพื่อคุ้มครองเด็กและ
ช่วยเหลือด้านสภาพจิตใจกับจิตแพทย์ต่อ](https://image.slidesharecdn.com/qjnirmqqkwitowjue5vg-signature-8778b5cc48d093758c78950a2029edcc14e324f73053c732e914a05b6e9f543b-poli-160514181421/85/Survival-new-401-320.jpg)