Downloaded 145 times
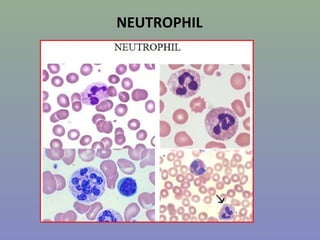
































This document provides information on various types of blood cells. It describes the characteristics of bands, neutrophils, eosinophils, basophils, monocytes, lymphocytes, and their appearances under the microscope. It also discusses some disorders associated with abnormal counts of these cells, such as neutropenia, neutrophilia, eosinophilia, lymphocytopenia, and lymphocytosis.