Downloaded 308 times
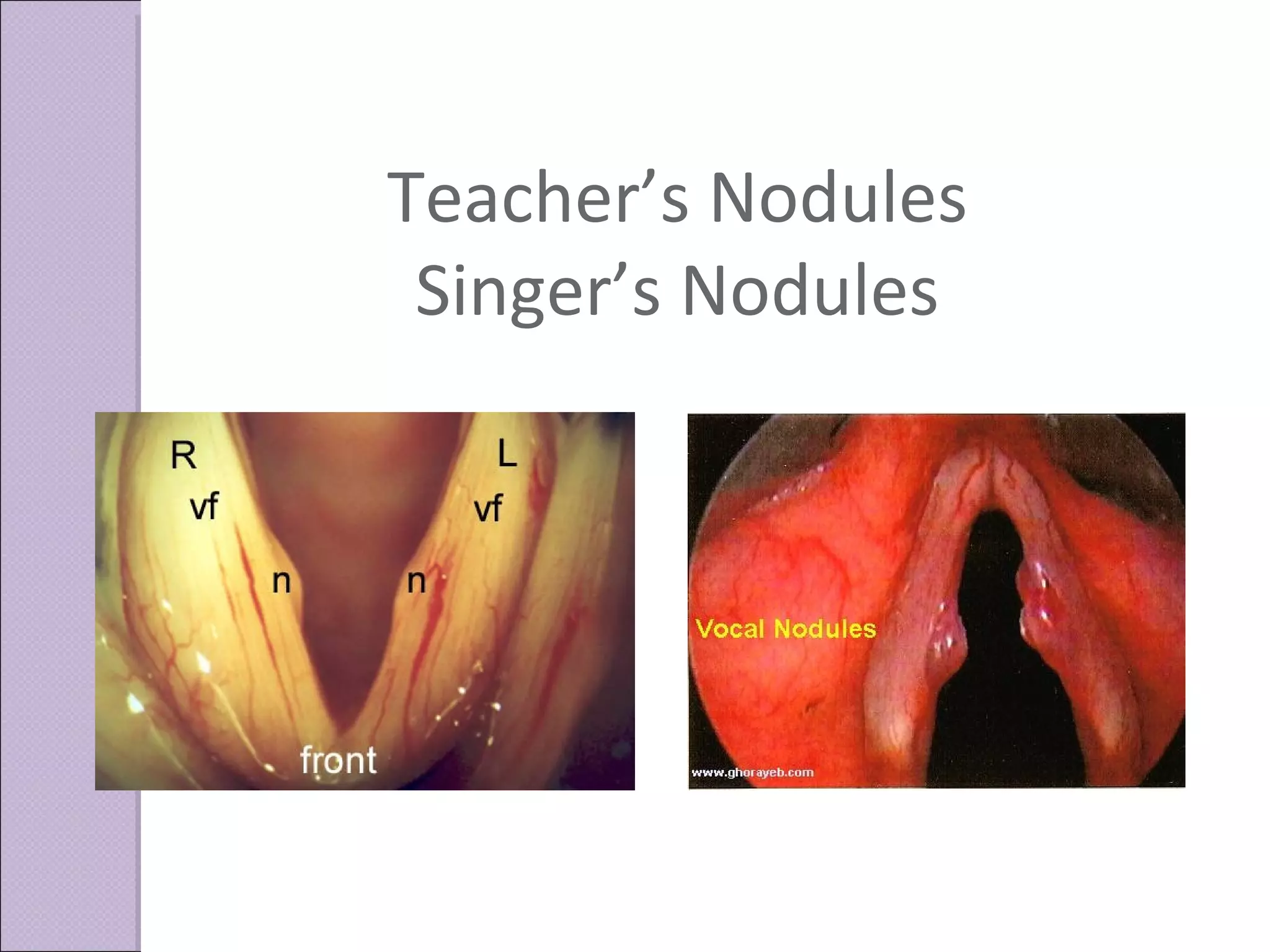

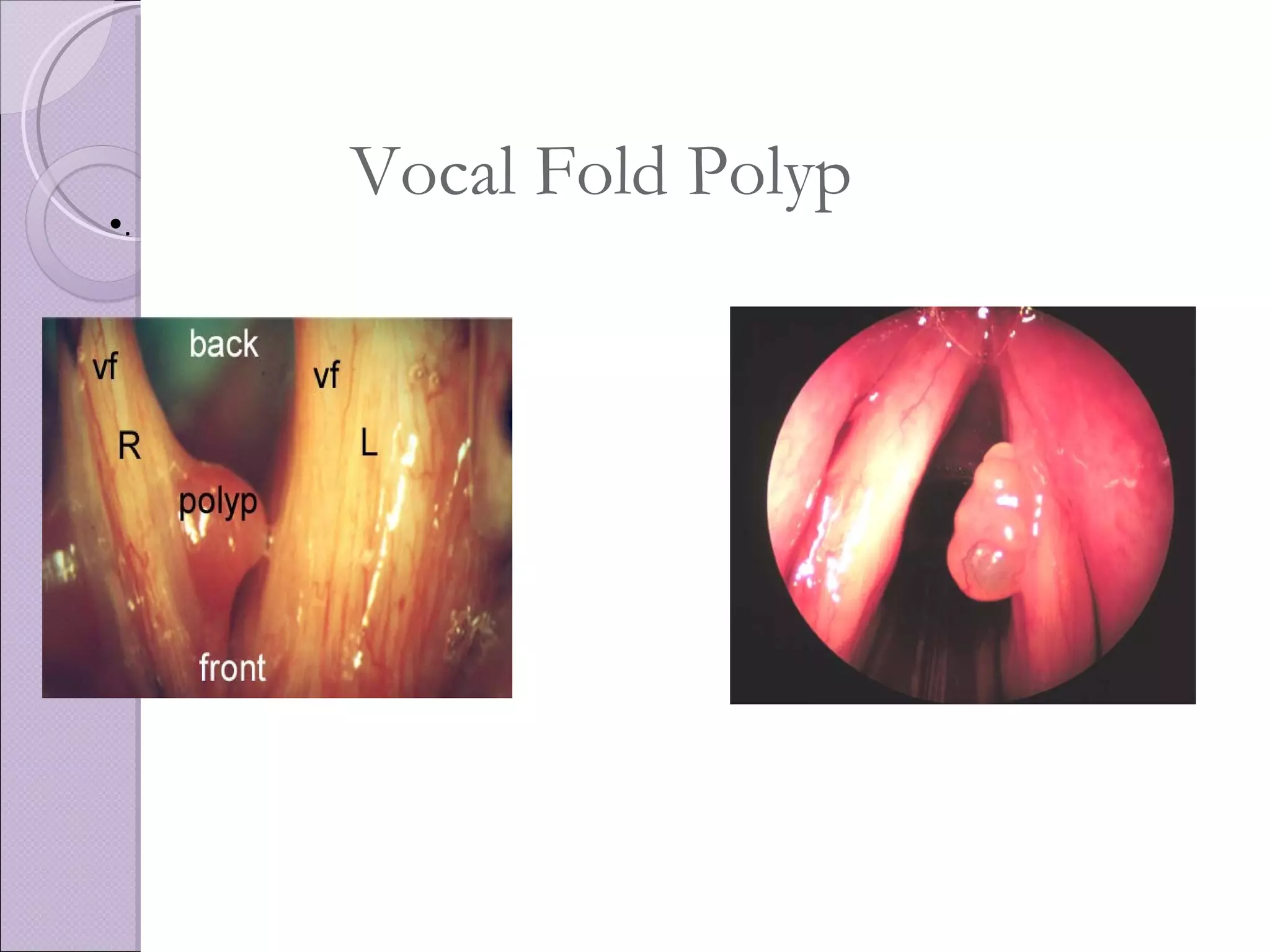

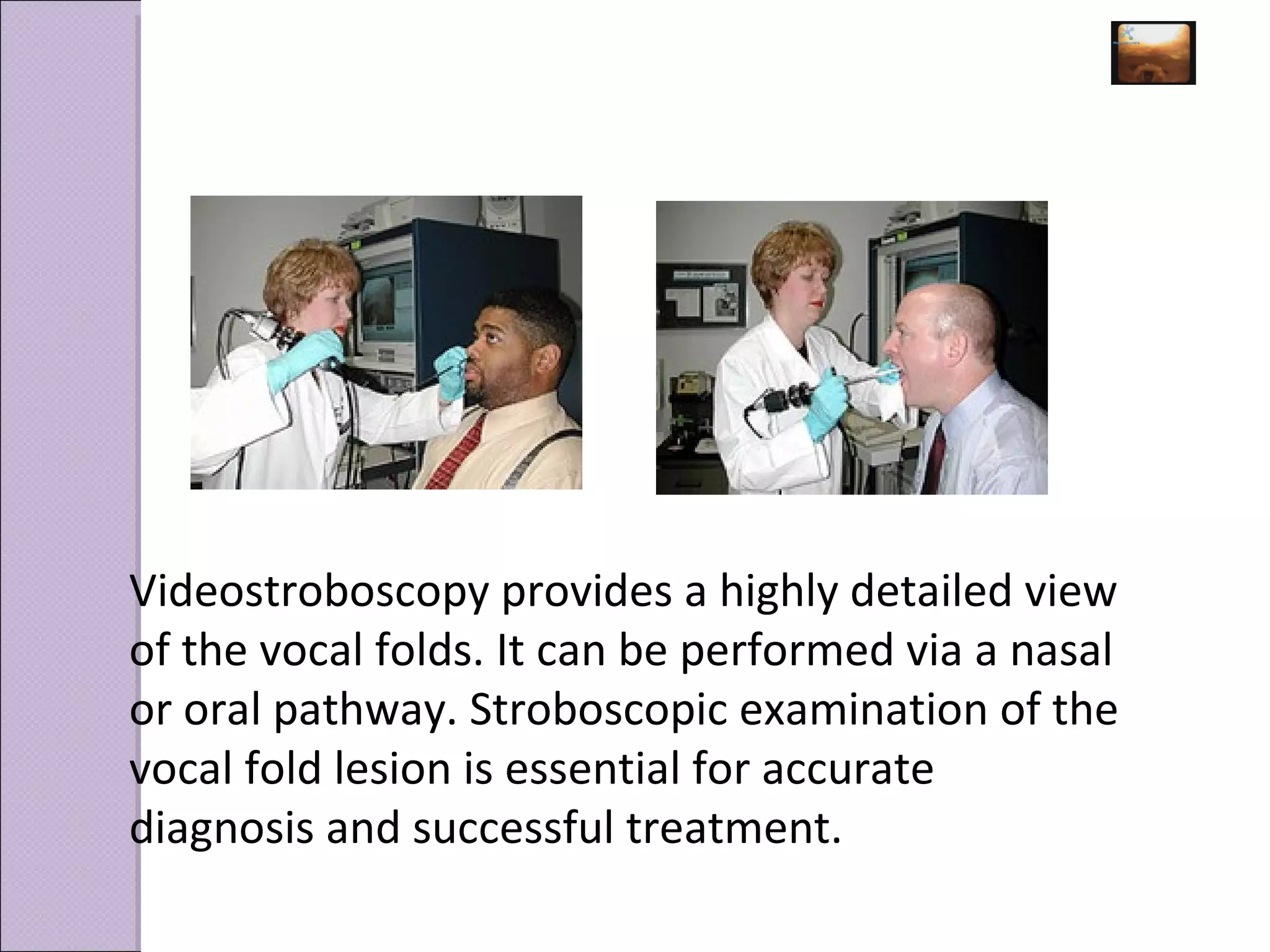
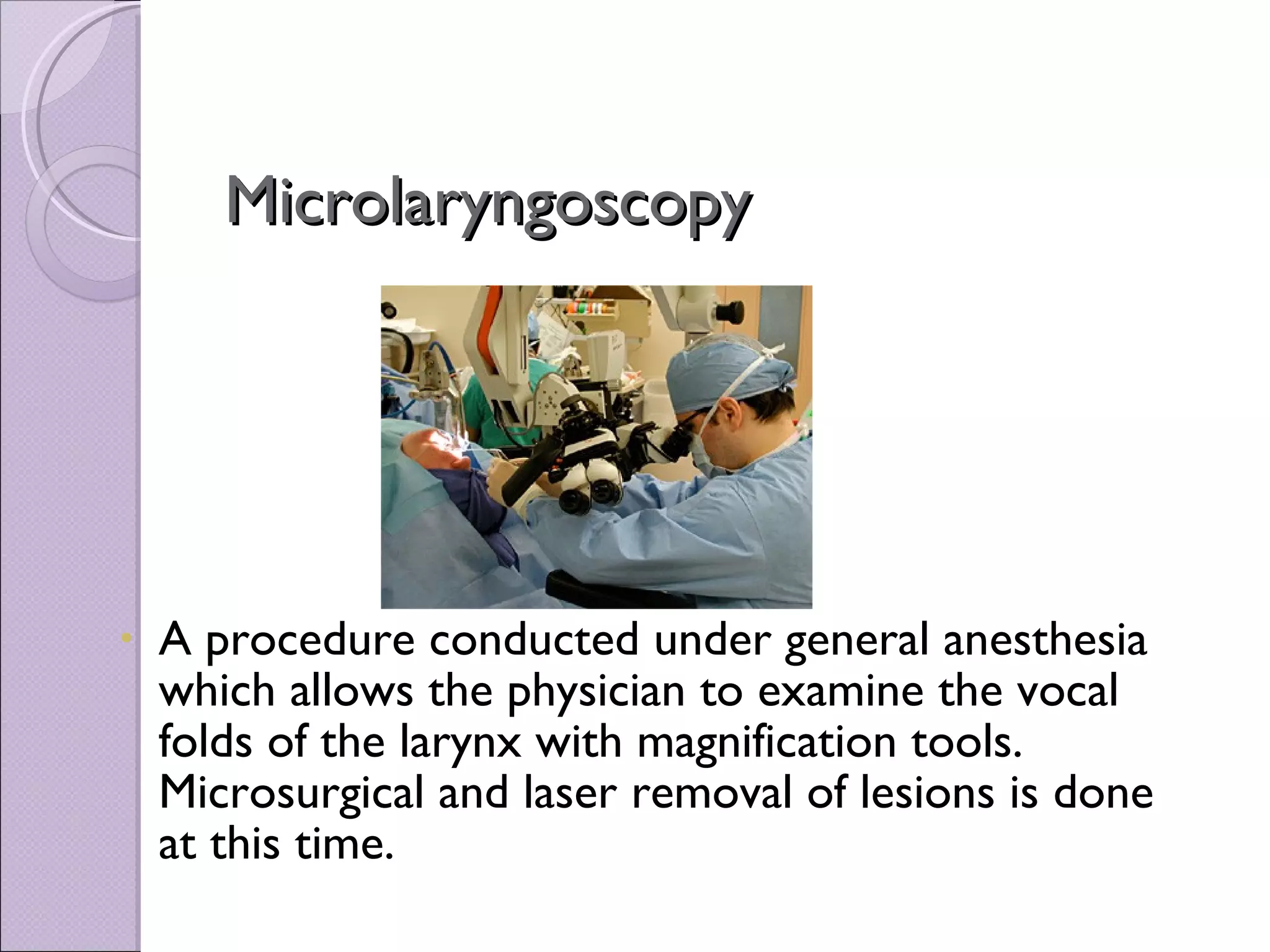

The document discusses vocal nodules and polyps, which are benign growths on the vocal folds caused by vocal abuse or misuse. Vocal nodules are small lesions less than 3mm located at the front of the vocal folds, while polyps are larger lesions. Symptoms include hoarseness, vocal fatigue, and difficulty speaking. Treatment involves voice therapy, medical management, and surgery to remove the growths if they are large or not improving. Surgical complications can include scarring and loss of voice if the layers of the vocal folds are damaged during removal of the nodules or polyps.

















































































