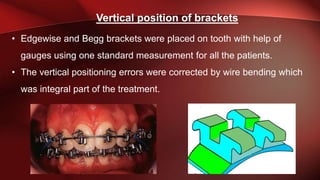
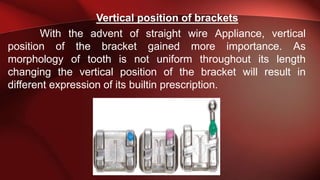
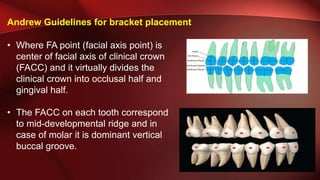
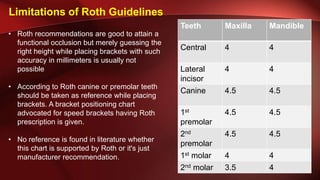
This document discusses different guidelines for determining the vertical position of orthodontic brackets. It begins by outlining Angle's initial proposal to place bands at the center of the tooth surface and discusses subsequent modifications by Edgewise and Begg appliances. It then examines guidelines proposed by Andrew, Roth, Alexander, Bishara, and McLaughlin/MBT. Each approach has limitations in addressing individual tooth variations. The document concludes by describing Kalange's method, which uses marginal ridge lines and measurements from molars and premolars to determine bracket heights aimed at leveling marginal ridges.