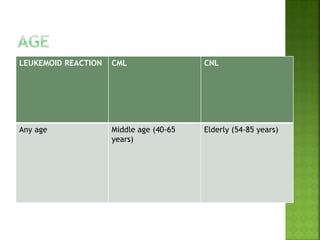
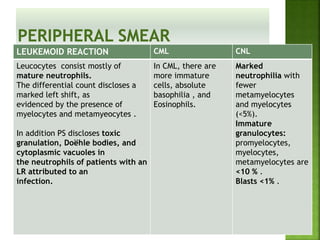
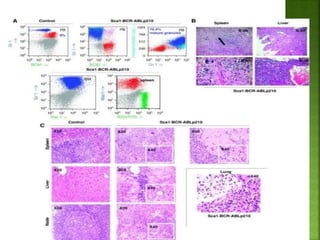
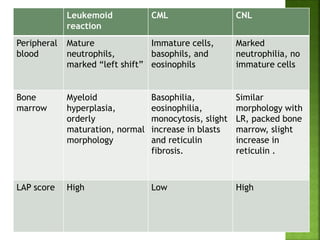
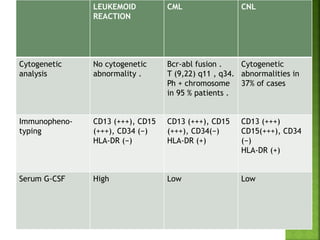
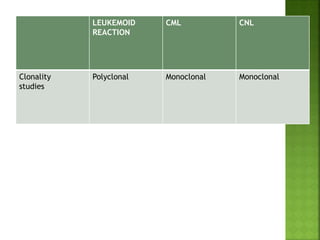
1. The document discusses the differentiation between myeloid leukemoid reaction, chronic myeloid leukemia (CML), and chronic neutrophilic leukemia (CNL).
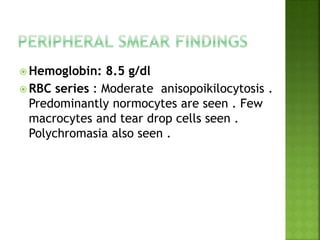
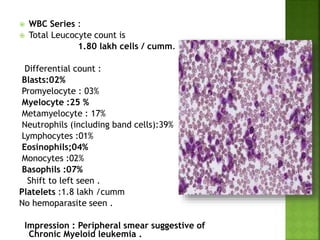
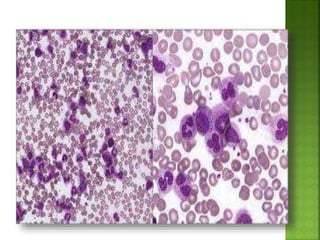
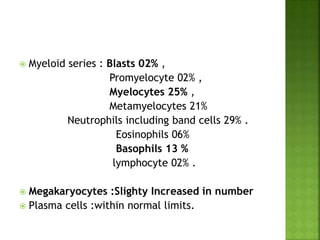
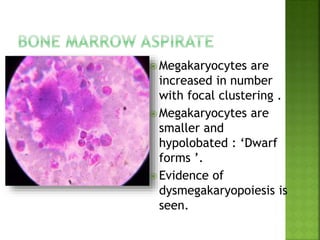
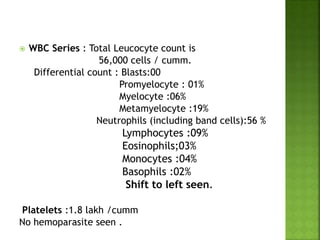
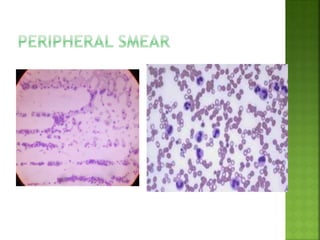
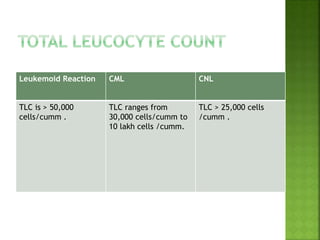
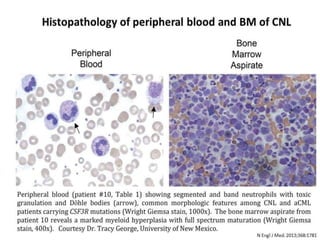
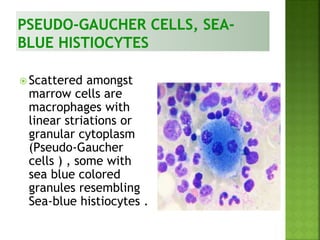
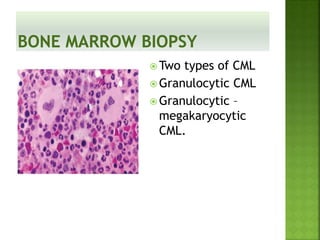
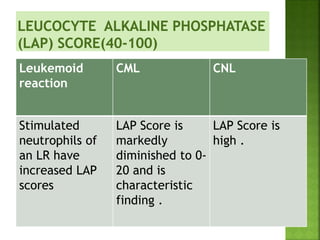
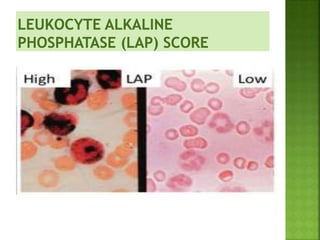
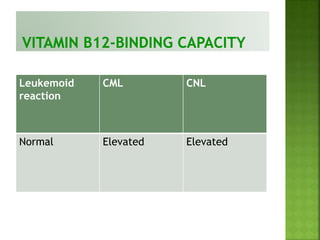
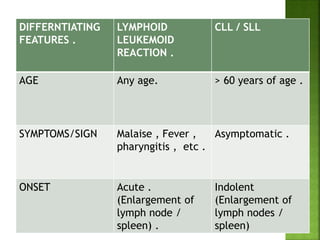
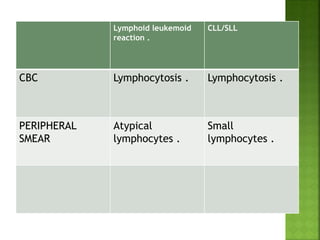
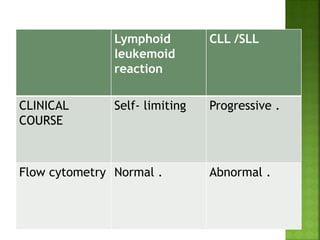
2. Key differences include peripheral smear findings, bone marrow aspirate/biopsy pictures, LAP scores, cytogenetics, and immunophenotyping results.
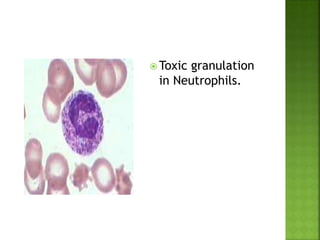
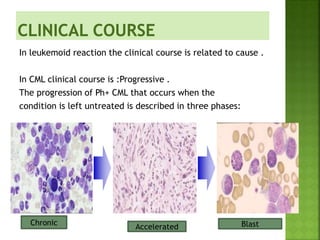
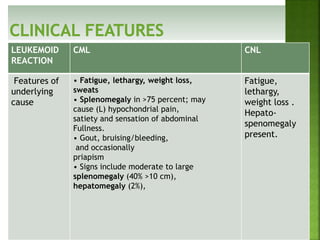
3. A leukemoid reaction is secondary to an underlying cause and shows features of that cause, while CML and CNL are myeloproliferative neoplasms with distinct clinical features, lab findings, and disease progression.
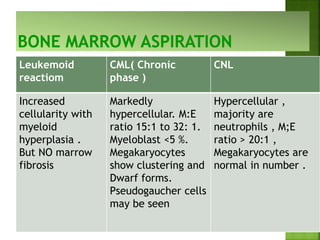
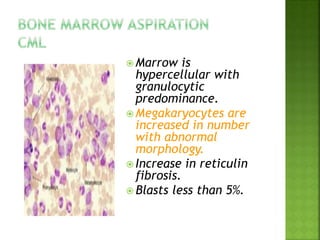





























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




