Acute inflammation is a protective process that helps eliminate harmful stimuli and promote tissue repair. It is characterized by increased blood flow, vascular permeability, and migration of white blood cells. The major signs of acute inflammation are heat, redness, swelling, pain, and loss of function. Key events in acute inflammation include changes in blood vessels that allow fluid and cells to move between blood vessels and tissues. White blood cells like neutrophils are recruited to destroy pathogens and initiate repair.
In this document
Powered by AI
Introduction to inflammation, its role as a protective mechanism against injury and infections.
Inflammation is essential for healing but can cause chronic diseases. Major causes include trauma, toxins, and pathogens.
Differences between acute and chronic inflammation regarding duration and immune cell types.
Key components of acute and chronic inflammation include cells, proteins, and structural proteins.
Cardinal symptoms of inflammation: Heat, redness, swelling, pain, and loss of function.
Tissue-specific terminology for inflammation using the suffix '-itis' (e.g., pancreatitis, arthritis).
Acute inflammation involves vascular changes leading to increased blood flow, permeability, and leukocyte migration.
Process by which leukocytes migrate through blood vessels and tissues during inflammation.
Key adhesion molecules and their roles in facilitating leukocyte migration during inflammation.
Leukocyte activation mechanisms during inflammation, including chemotaxis and signaling pathways.
Neutrophil functions in pathogen clearance via phagocytosis and reactive metabolites.
steps involved in phagocytosis, including particle recognition, engulfment, and destruction.
Acute phase response effects, such as fever, leukocytosis, increased acute phase proteins.
Clinical examples of leukocyte-induced injury and acute inflammatory diseases including infections.
Immunodeficiencies and specific syndromes affecting leukocyte function leading to increased infections.
Potential developments from acute inflammation include resolution, healing, or chronic inflammation.
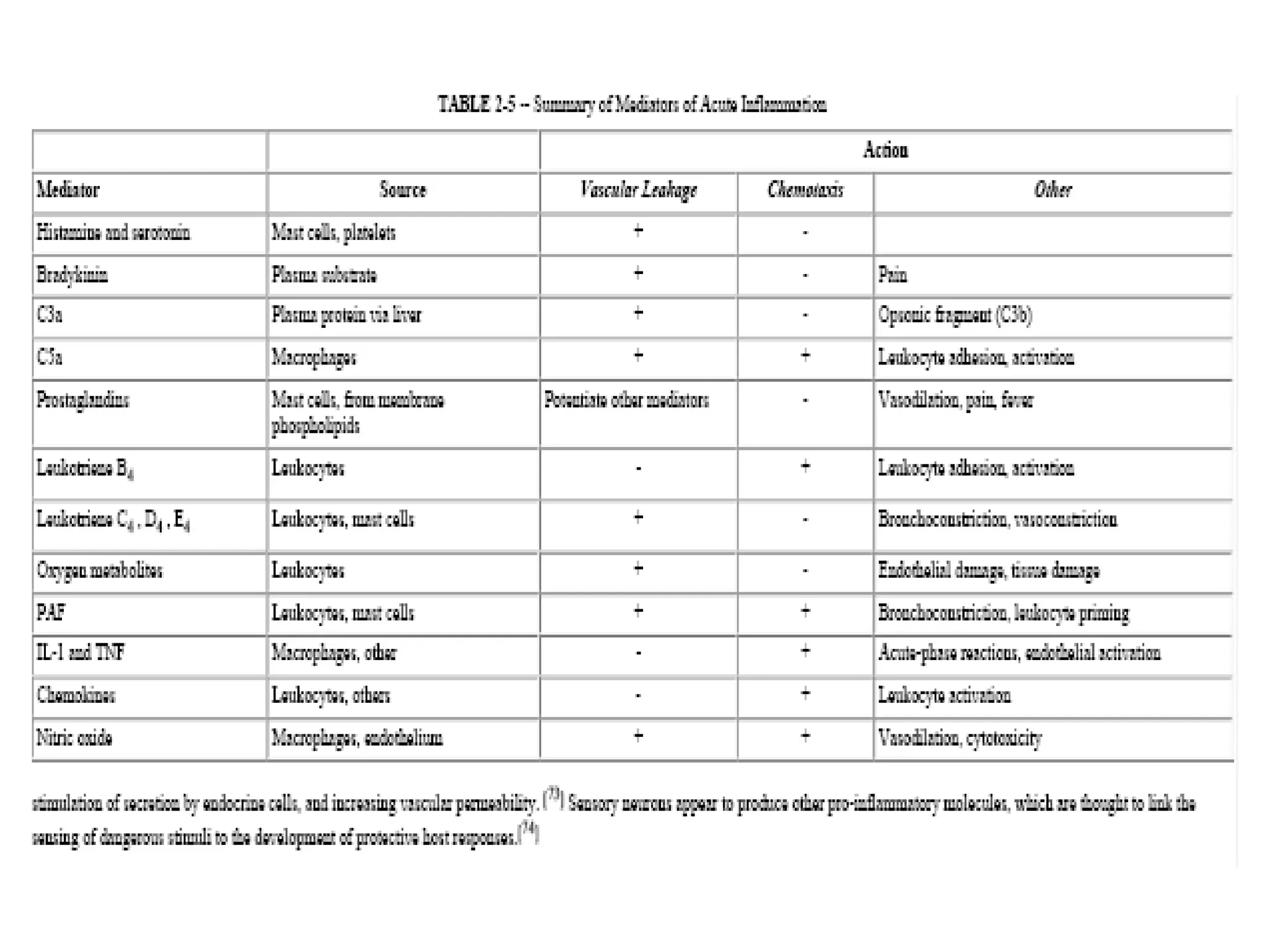
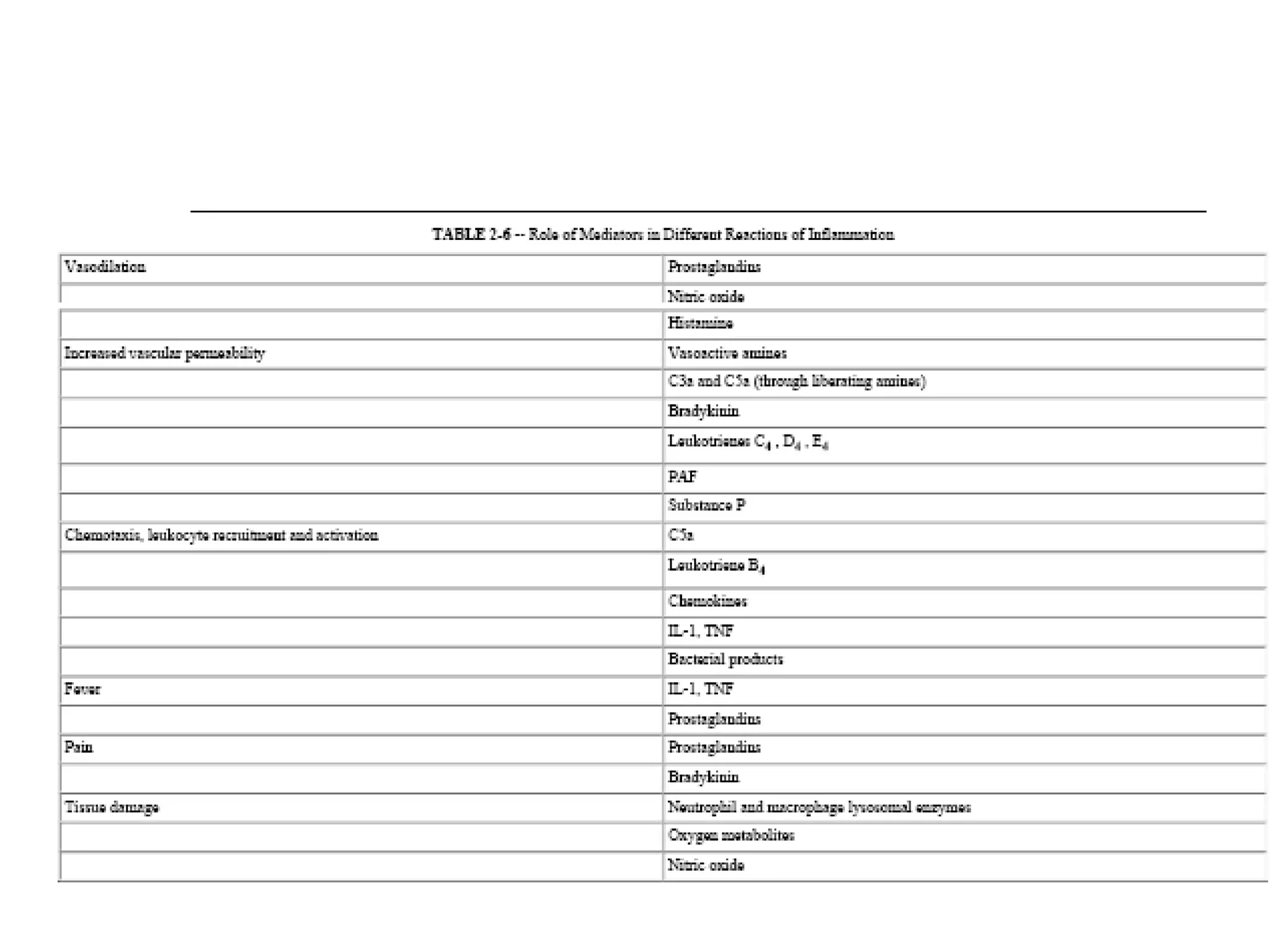
Biological activities and roles of various preformed and newly synthesized chemical mediators in inflammation.
Discussion of the complement system and bradykinin actions in the context of inflammatory response.
Major functions of interleukin-1 and tumor necrosis factor, plus nitric oxide roles in vascular biology.
End of the presentation, expressing gratitude to the audience.
Acute inflammation andchemical mediators of inflammation Pooja Sharma Moderator: Dr Biman saikia
2.
INFLAMMATION Is fundamentallya protective mechanism designed to rid the organism of both the initial cause of cell injury (microbes, toxins) and the consequences of such injury (necrotic cells, tissues). Without inflammation infections would go unchecked wounds would never heal injured organs might remain permanent festering sores.
3.
Inflammation… Inflammation andrepair may be potentially harmful , however. Life-threatening hypersensitivity reactions to insect bites, drugs and toxins Chronic diseases- rheumatoid arthritis, atherosclerosis and lung fibrosis. The major causes of inflammation are: Trauma ( sprain, strain, contusion, etc.) Chemical agents ( poisons, stings, etc.) Thermal extremes of heat or cold (burns) Pathogenic organisms ( infections )
4.
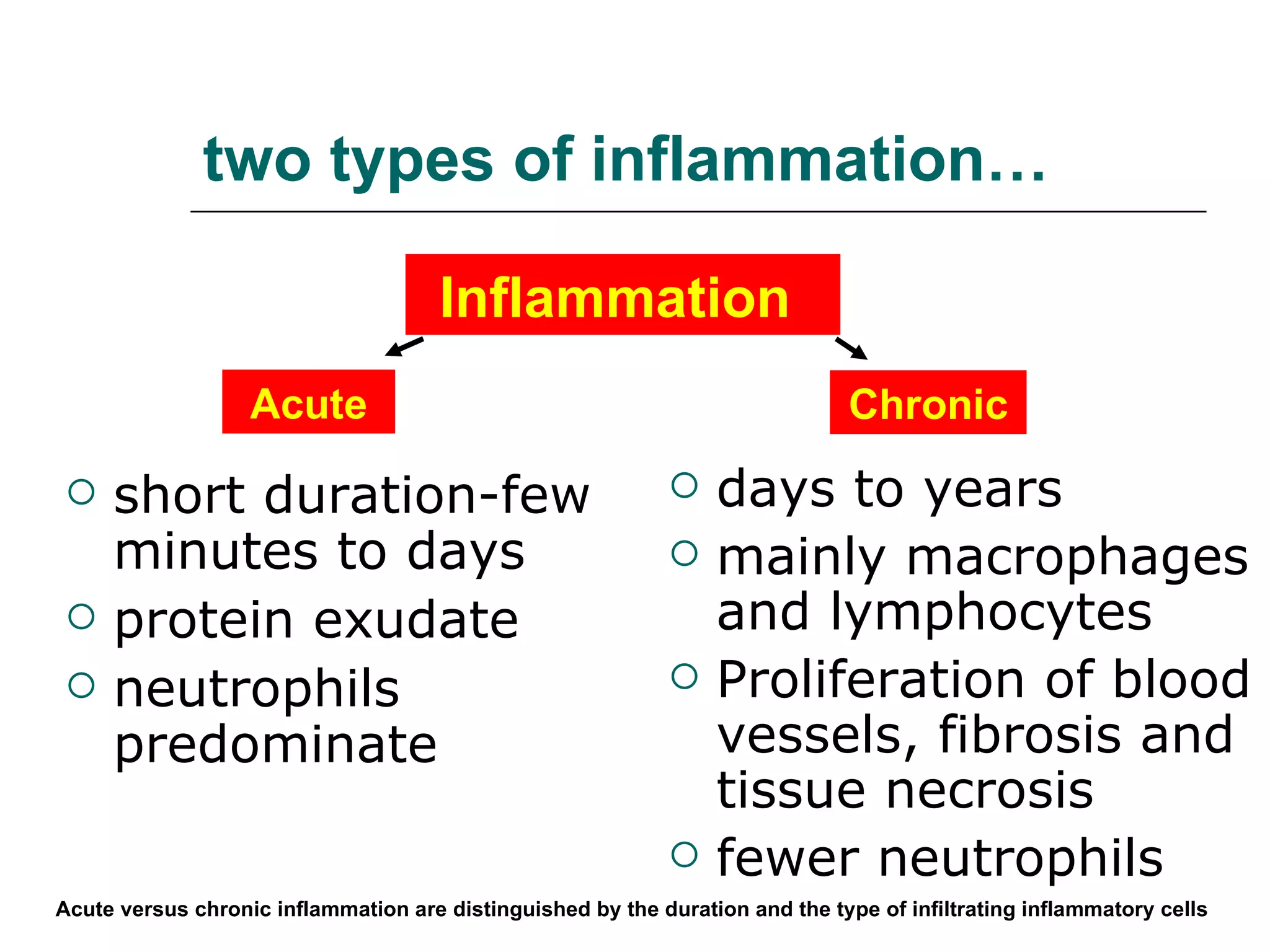
two types ofinflammation… short duration-few minutes to days protein exudate neutrophils predominate days to years mainly macrophages and lymphocytes Proliferation of blood vessels, fibrosis and tissue necrosis fewer neutrophils Acute versus chronic inflammation are distinguished by the duration and the type of infiltrating inflammatory cells Inflammation Acute Chronic
5.
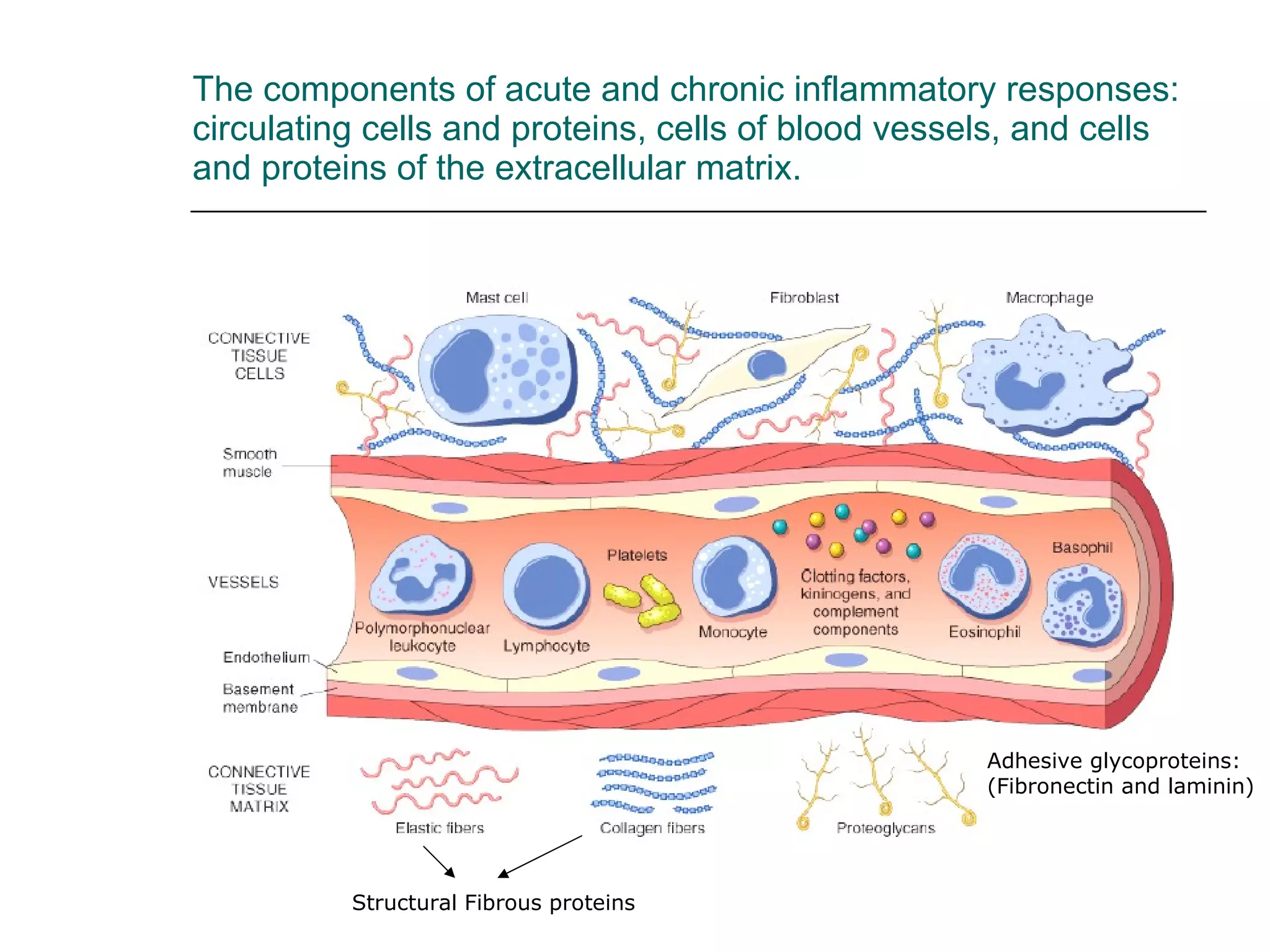
The components ofacute and chronic inflammatory responses: circulating cells and proteins, cells of blood vessels, and cells and proteins of the extracellular matrix. Structural Fibrous proteins Adhesive glycoproteins: (Fibronectin and laminin)
6.
SIGNS AND SYMPTOMSOF INFLAMMATION HEAT REDNESS SWELLING PAIN LOSS OF FUNCTION Calor Rubor Tumor Dolor Functio laesa The inflammatory response can be either acute or chronic, but the local reactions are described as the cardinal signs and symptoms of inflammation:
7.
The nomenclature usedto describe inflammation in different tissues employs the tissue name and the suffix “- itis ” e.g pancreatitis meningitis pericarditis arthritis
8.
Acute inflammation involves:alteration of vascular caliber (vasodilation leads to increased blood flow) changes of microvasculature (increased permeability for plasma proteins and cells) emigration of leukocytes from microcirculation (leukocyte activation leads to elimination of offending agent)
9.
Vascular changes playan important role during acute inflammation (begin early after injury and depends upon the severity of the injury) Vasodilation , leads to increased blood flow causing redness and warmth (rubor and calor) Increased Permeability , leads to exudation of protein rich fluid into the extravascular space causing swelling (tumor) Loss of fluid from the vessels leads to Concentration of red cells resulting in decreased velocity and stasis of the blood flow Leukocyte rolling, adhesion and migration leads to the accumulation of inflammatory cells
10.
Increased vascular permeabilityand edema: a hallmark of acute inflammation loss of protein from plasma leads to edema due to reduced osmotic pressure in the vasculature and increased osmotic pressure in the interstitium Leakage is restricted to venules of 20-60 m in diameter caused by endothelial gaps usually an immediate and transient response (30 min.) Gaps occur due to contraction of e.g. myosin and shortening of the individual endothelial cell Normal fluid exchange and vascular permeability depends upon intact endothelium Proposed mechanisms for how the endothelium becomes leaky?
11.
direct endothelial injury causing necrotic cell death will result in leakage from all levels of microcirculation (venules, capillaries and arterioles) reaction is immediate and sustained Delayed prolonged leakage begins after 2-12 hours and can last several days occur due to thermal-, x-ray or ultraviolet radiation (sunburn) and involves venules and capillaries Transcytosis occurs across channels consisting of interconnected, uncoated vesicles and vacuoles called vesiculovacuolar organelle. Certain factors like VEGF increases number and size of these channels. during tissue repair - new blood vessels ( angiogenesis) – remain leaky until intercellular junctions are formed. All these described mechanisms may occur in one wound (e.g burns) and can be life threatening
12.
A critical functionof the vascular inflammatory response (stasis and vascular permeability) is to deliver leukocytes to the site of injury in order to clear injurious agents Neutrophils are commonly the first inflammatory cells (first 6-24 hours) recruited to a site of inflammation. Extravasation of leukocytes is a coordinated event of: margination rolling, adhesion, transmigration (diapedesis) migration.
13.
In normal flowingblood erythrocytes are confined to a central axial column , displacing leukocytes towards the wall of vessel. As blood flow slows in inflammation more white cells assumes peripheral position along the endothelial surface. This process of leukocyte accumulation is called margination Laminar blood flow maintains the leukocytes against the venular wall
14.
The multistep processof leukocyte migration through blood vessels. Slowly move along the endothelium and adhere transiently (process called rolling) finally they come to rest at some point - adhere firmly. After adhesion they insert there pseudopods into endothelial cell junction and squeeze through this layer into the extarvascular space. The process of adhesion and transmigration is determined by binding of adhesion molecules on leukocytes and endothelial cells.
15.
Four families ofadhesion molecules are involved in leukocyte migration Selectins E-selectin (endothelium) P-selectin (endothelium & platelets) L-selectin (leukocytes) Ligands are sialylated glycoproteins (e.g Sialylated Lewis X) which are linked to mucin-like glycoproteins:PSGL-1,GlyCAM-1 , ESL-1, CD34 Immunoglobulin family ICAM-1 (intercellular adhesion molecule 1) VCAM-1 (vascular adhesion molecule 1) Are expressed on activated endothelium Ligands are integrins on leukocytes Integrins ( + chain) Heterodimeric molecules VLA-4 ( 1 integrin) binds to VCAM-1 LFA1 and MAC1 (CD11/CD18) = 2 integrin bind to ICAM Expressed on leukocytes Mucin-like glycoproteins Heparan sulfate (endothelium) Ligands for CD44 on leukocytes
16.
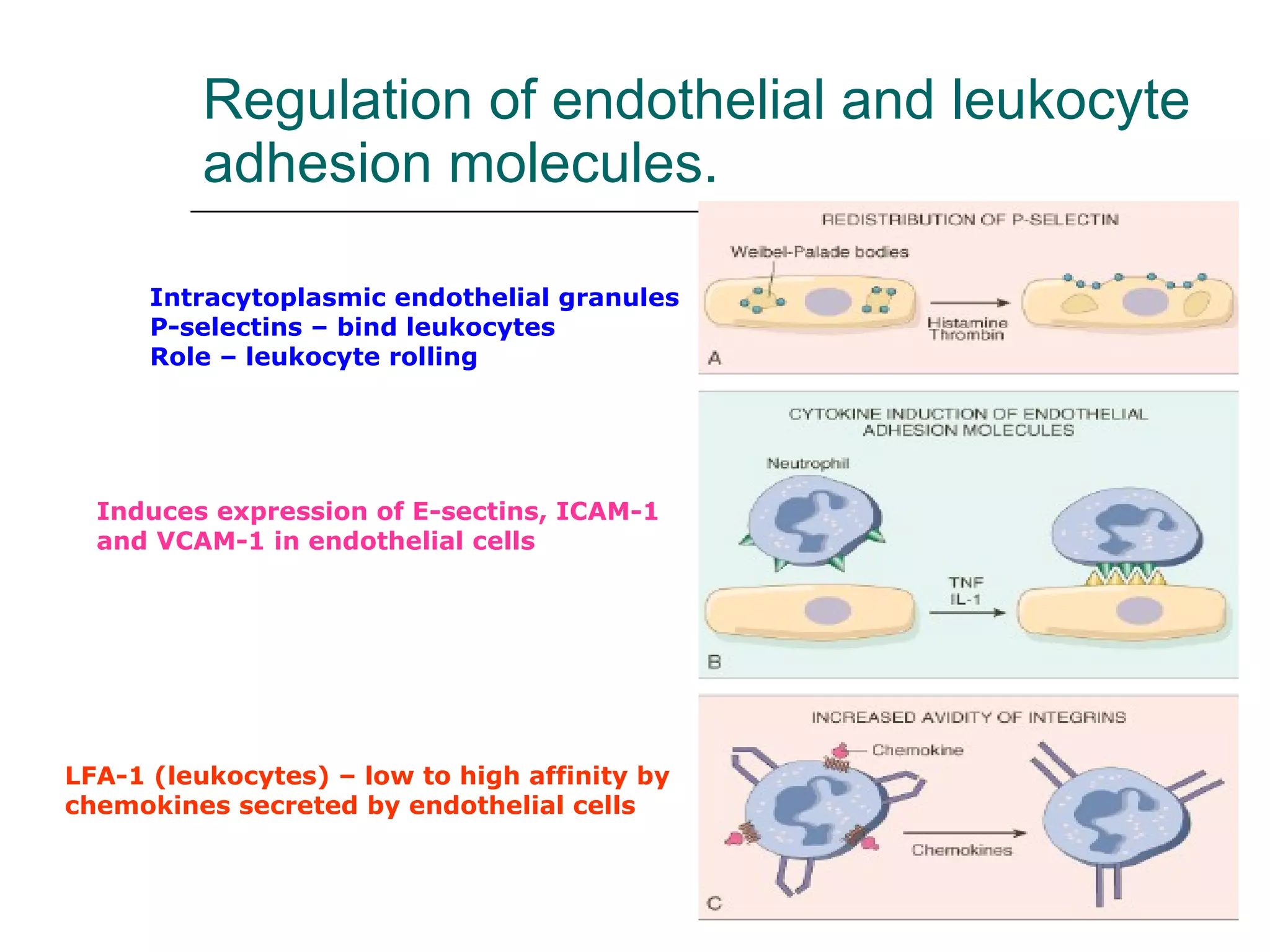
Regulation of endothelialand leukocyte adhesion molecules. Intracytoplasmic endothelial granules P-selectins – bind leukocytes Role – leukocyte rolling Induces expression of E-sectins, ICAM-1 and VCAM-1 in endothelial cells LFA-1 (leukocytes) – low to high affinity by chemokines secreted by endothelial cells
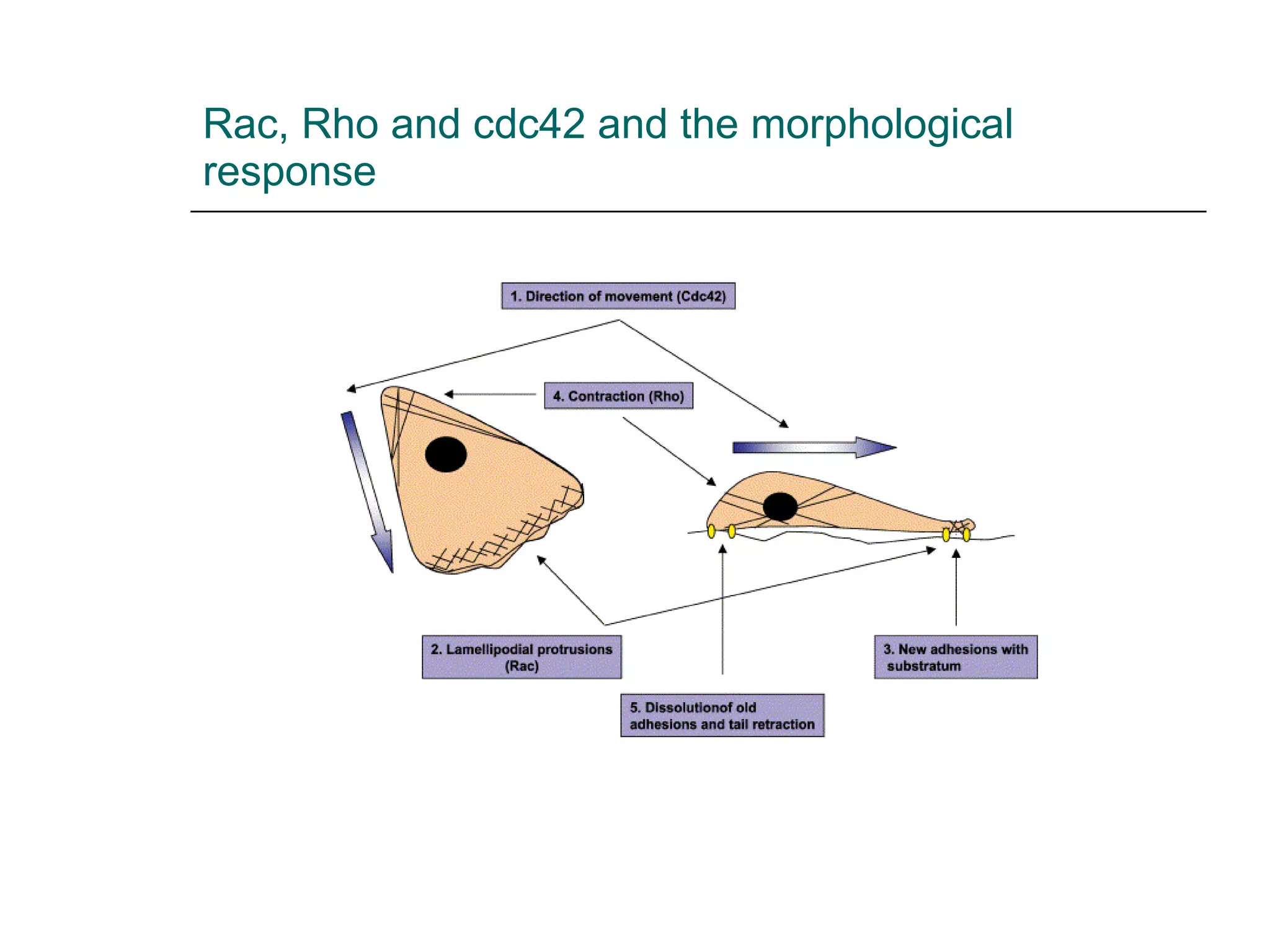
Leukocytes follow towardsthe site of injury in the tissue along a chemical gradient of chemo-attractants in a process called chemotaxis. Exogenous and endogenous stimuli can act as chemoattractants Exogenous: bacterial product (e.g N- formyl-methionyl peptides Endogenous: anaphylatoxins (C5a), leukotrienes (LTB4), chemokines (e.g IL-8) Most chemotactic agents signal via G-protein-coupled 7 transmembrane receptors leading to the activation of phospholipase C resulting in intracellular Ca2+ release and activation of small GTPases (Rac,Rho, cdc42) . This leads to actin/myosin polymerization and a morphological response with directional filopodia formation
While signaling of chemo-attractants induces a morphological response and locomotion of neutrophils, pattern recognition receptors or opsonin receptors induce neutrophil and macrophage effector functions Pattern recognition receptors recognize CD14 LPS Toll-like receptor endotoxins, CpG, dsRNA, bacterial proteoglycans Mannose receptor bacterial carbohydrates Scavenger receptors lipids Opsonin-receptors recognize CR1 complement product C3b Fc receptor IgG coated pathogens
21.
Neutrophil and macrophageeffector functions serve to eliminate pathogens and noxious substances Phagocytosis of pathogens and noxious agents Release of bactericidal and cytoxic molecules
22.
Phagocytosis and itsoutcome involves three distinct steps Recognition and attachment Engulfment and fusion of phagosome and lysosome Killing and degradation mainly through the generation of oxygen radicals and their halogenation
23.
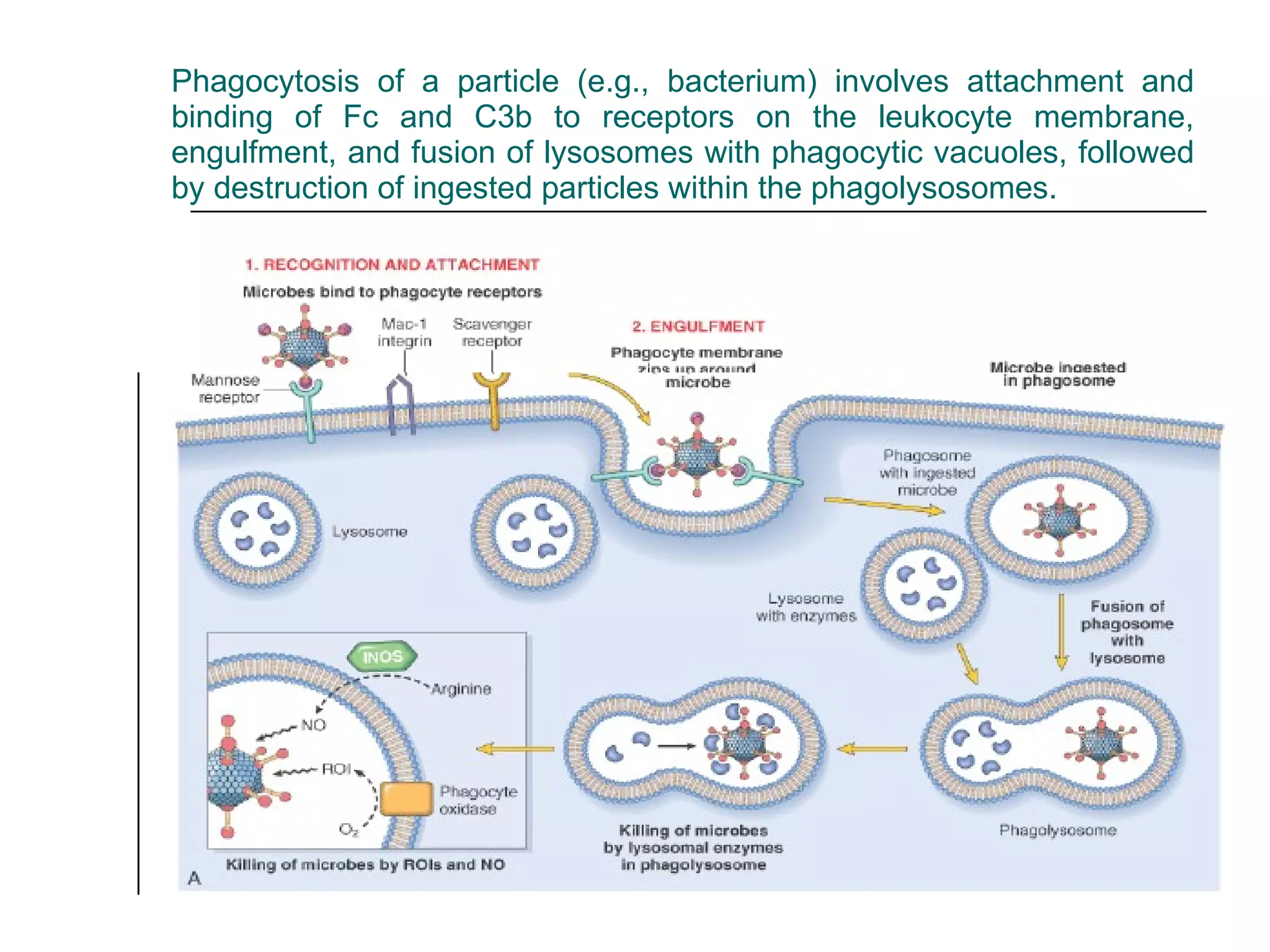
Phagocytosis of aparticle (e.g., bacterium) involves attachment and binding of Fc and C3b to receptors on the leukocyte membrane, engulfment, and fusion of lysosomes with phagocytic vacuoles, followed by destruction of ingested particles within the phagolysosomes.
24.
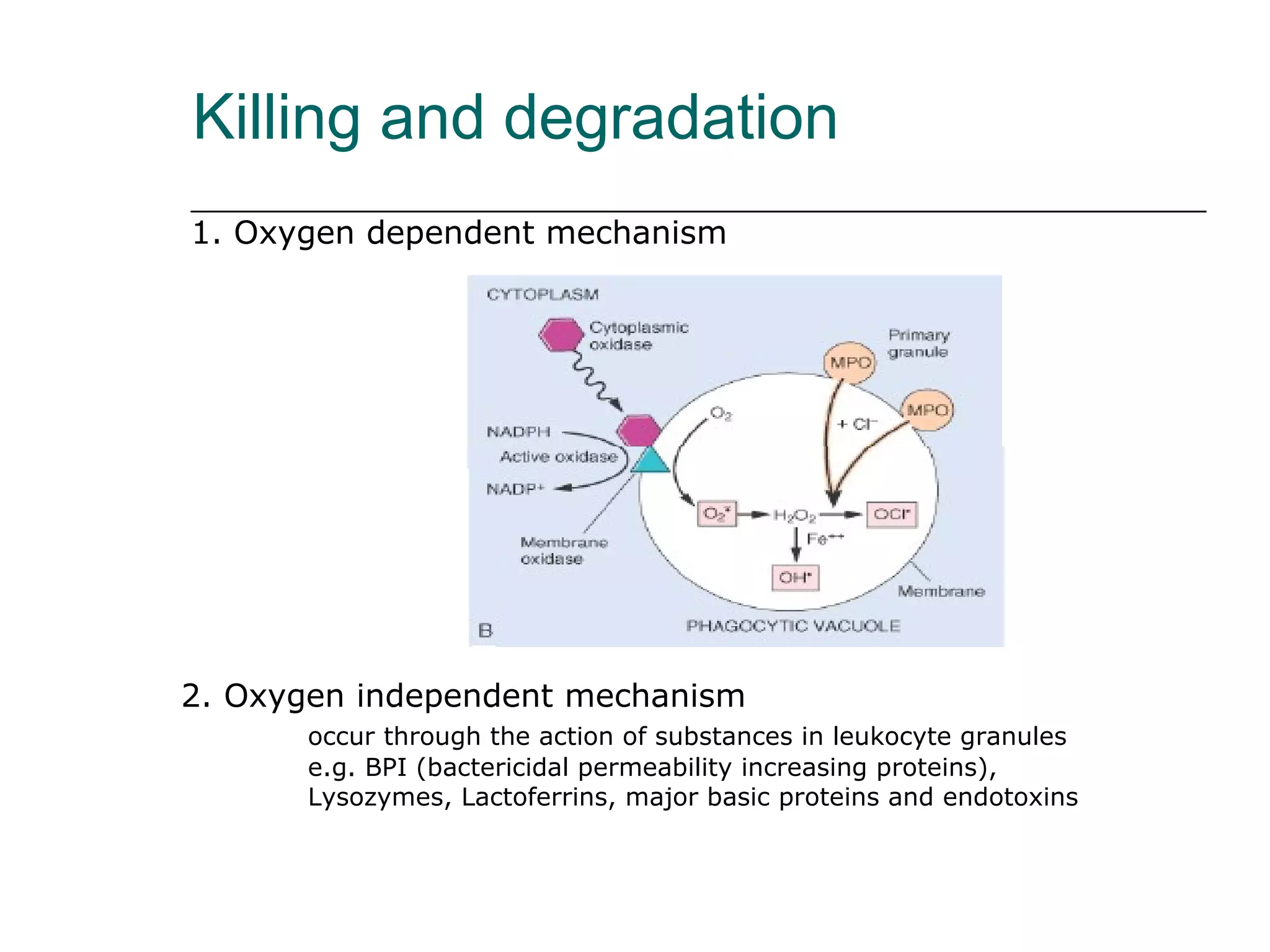
Killing and degradation1. Oxygen dependent mechanism 2. Oxygen independent mechanism occur through the action of substances in leukocyte granules e.g. BPI (bactericidal permeability increasing proteins), Lysozymes, Lactoferrins, major basic proteins and endotoxins
25.
Systemic effects ofacute inflammation acute phase response Fever (temperature > 37.8 o C or >100 F) Increased pulse, blood pressure Chills Anorexia Leukocytosis neutrophilia and left shift of neutrophils points to bacterial infection Lymphocytosis points to viral infection Eosinophilia point to allergy or parasitic infection Acute phase protein production in liver fibrinogen, CRP,SAA leads to increased ESR
26.
Increased ErythrocyteSedimentation Rate as a result of the presence of acute phase reactants ESR = rate at which erythrocytes settle out of unclotted blood in one hour Normally, Erythrocytes are very buoyant and settle slowly Erythrocytes are negatively charged and repel each other (no aggregation occurs) In presence of acute phase reactants (fibrinogen) erythrocytes aggregate due to loss of their negative charge resulting in increased sedimentation ESR is a widely performed test to detect occult processes and monitor inflammatory conditions
27.
Granulocytosis with “leftshift” of neutrophil population are a good indicator for a severe bacterial infection Leukocyte release result from a direct effect of IL-1 and IL-6 on bone marrow neutrophil stores. Exaggeration of this can result in a “ Leukemoid reaction ” release of very immature precursors and cell counts >25-30 x 10 6 / l
28.
Termination of acuteinflammation Eradication of an offending agent should lead to discontinuation of the inflammatory response Neutrophils have only a short life span (few hours -1 day) Most mediators are very short lived and are degraded immediately Anti-inflammatory cytokines ( TGF-beta , and IL-10 ) can inhibit the production of pro-inflammatory cytokines (TNF) In Arachidonic acid metabolism, lipoxin and resolvins are generated that have anti-inflammatory activity
Peptic ulcer Anulcer is a local defect of mucosal lining produced by shedding of necrotic tissue Peptic ulcers are produced by an imbalance between gastro-duodenal defense mechanisms and the damaging force 70% of all ulcers are due to H. pyolri infection which initiates a strong inflammatory response
34.
Septicemia with disseminatedintravascular coagulation due to Meningococca l Infection Invasion of the bloodstream by Neisseria meningitides leads to widespread vascular injury with endothelial necrosis, thrombosis and peri-vascular hemorrhage. Hemorrhage as it is seen in the skin can occur in all organs
Immunodeficiency Diseases causedby deficiencies or defects in phagocytes (neutrophils and macrophages) Lack of neutrophil/macrophage numbers or defect of their function can lead to live threatening infectious diseases, particularly with bacterial and fungal pathogens Clinically most common: bone marrow suppression with decreased cell numbers (leukopenia) due to tumor infiltrate or chemotherapy resulting in myelosuppression (>500 neutrophils / l is considered very severe) However, inherited defects of adhesion, phago-lysosome- and microbicidal functions have been found
37.
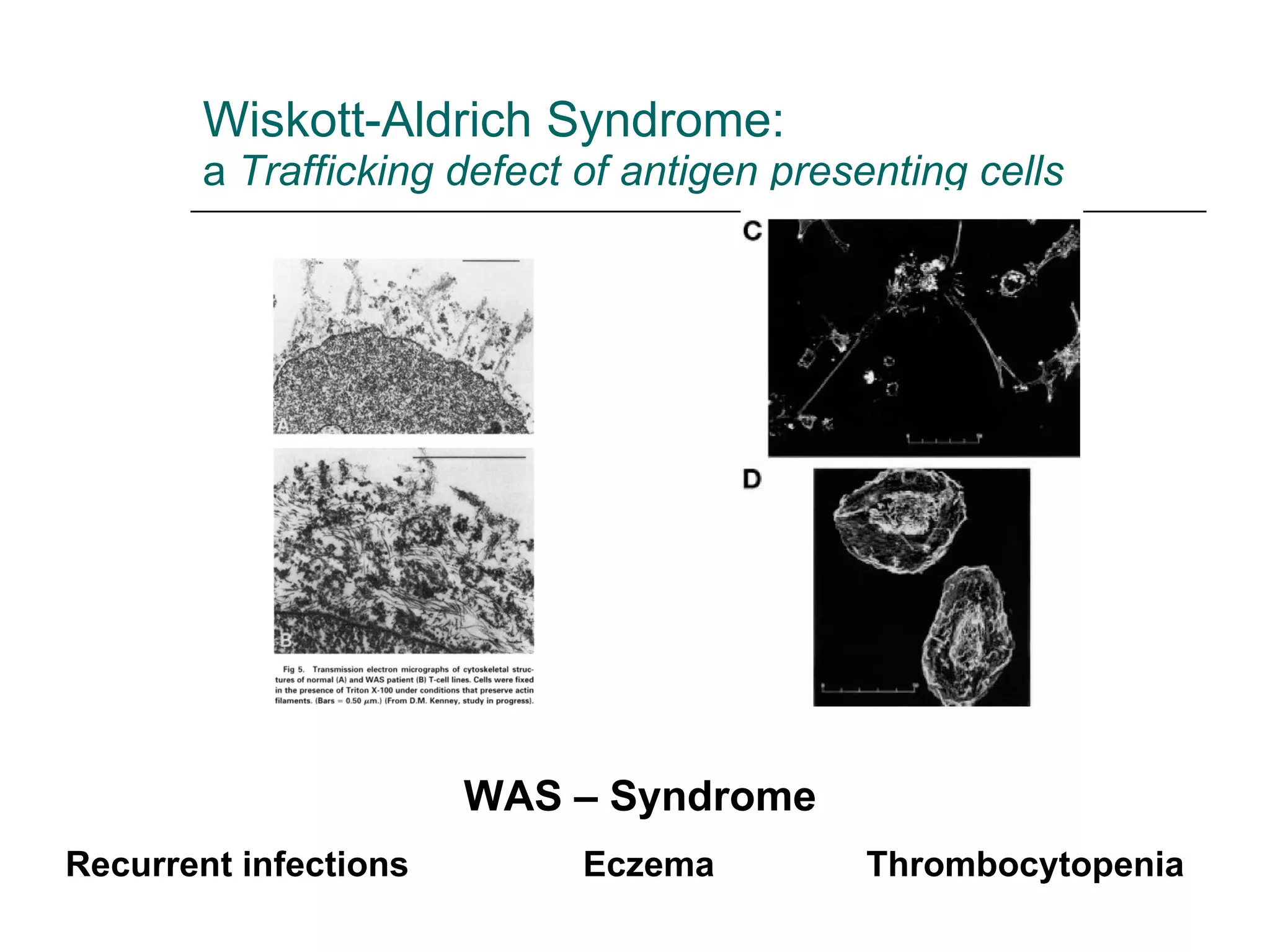
Wiskott-Aldrich Syndrome: a Trafficking defect of antigen presenting cells WAS – Syndrome Recurrent infections Eczema Thrombocytopenia
38.
Leukocyte adhesion deficiency1 and 2 (LAD1/2) LAD 1 is a result of a lack of 2 intergrin expression due to defect of CD18 (LFA-1 and MAC-1). Interaction with ICAM and VCAM on endothelium is impaired LAD 2 results from a lack of sialyl LewisX (defect of carbohydrate fucosylation). Interaction with endothelial E-and P-selectins is impaired
39.
Leukocyte adhesion deficiencies(LAD 1 and 2) Neutrophils unable to aggregate Leukocytes unable to leave the circulatory system Neutrophil counts are commonly twice the normal level even without an ongoing infection (Leukocytosis) Clinical findings: History of delayed separation of umbilical cord Severe peridontitis Recurrent bacterial and fungal infections of oral and genital mucosa (enteric bacteria, staph, candida, aspergillus) Infected foci contain few neutrophils (no pus) and heal poorly LAD 2 immunodeficiency is less severe , however the defect is associated with growth retardation, dysmorphy and neurological deficits NEJM: Vol. 343: No 23, pp1703-1714
40.
Chronic granulomatous disease (a defect of NADPH oxidase system and therefore inability to undergo oxidative burst and production of hydrogen peroxide) CGD is a heterogeneous disorder caused by defects of any of the four subunits of NADPH oxidase. 70% are due to X-linked defect of gp91 phox (more severe form) Second most due to autosomal recessive defect of p47 phox NEJM: Vol. 343: No 23, pp1703-1714
41.
Chronic granulomatous disease= defect of NADPH oxidase system Clinical findings: Recurrent infections with catalse-positve microorganisms ( S. aureus, Burgholderia cepacia, aspergillus spec., nocardia spec., and Serratia marrcescens ) Recurrent infections of lungs, soft tissue and other organs (typical is infection of nares, and gingivitis) Appearance of fever and clinical signs of infection may be delayed Excessive formation of granuloma in all tissues NEJM: Vol. 343: No 23, pp1703-1714
42.
Chediak-HigashiSyndrome Defect of the formation and function of neutrophil granules CHS is an autosomal recessive disorder of all lysosomal granule containing cells with clinical features involving the hematological and neurological system All cells containing lysosomes have giant granules . In neutrophils large granules result from abnormal fusion of azurophilic and specific granules and delayed fusion with phagosomes. Neutrophils of CHS patients fail to orient themselves during chemotaxis resulting in delayed diapedesis Mutated gene: LYST = protein involved in vacuolar formation and transport of proteins
43.
Defect of theformation and function of neutrophil granules Chediak-Higashi Syndrome Clinical features: recurrent bacterial infections with S. aureus and beta hemolytic streptoc.; Peripheral nerve defects (nystagmus and neuropathy) Mild mental retardation and partial ocular and cutaneous albinism Platelet dysfunction and severe peridonatal disease Mild neutropenia and normal immunoglobulins NEJM: Vol. 343: No 23, pp1703-1714 Normal PMN Abnormal PMN
44.
Myeloperoxidase deficiency Mostcommon inherited disorder of neutrophils Catalyzes the generation of hypochlorous acid (HOCL) A deficiency is not generally associated with disease(!!!!) Except in patients with diabetes mellitus, who are susceptible to disseminated Candidiasis
45.
Outcomes of acuteinflammation: resolution, healing by fibrosis, or chronic inflammation
46.
Chemical mediators ofinflammation Perform biological activity by binding to specific receptors on target cells Some have direct enzymatic activity (lysosomal proteases) or mediate oxidative damage (oxygen metabolites). Once activated and released from cell, most of these are short lived- quickly decay, inactivated or inhibited.
47.
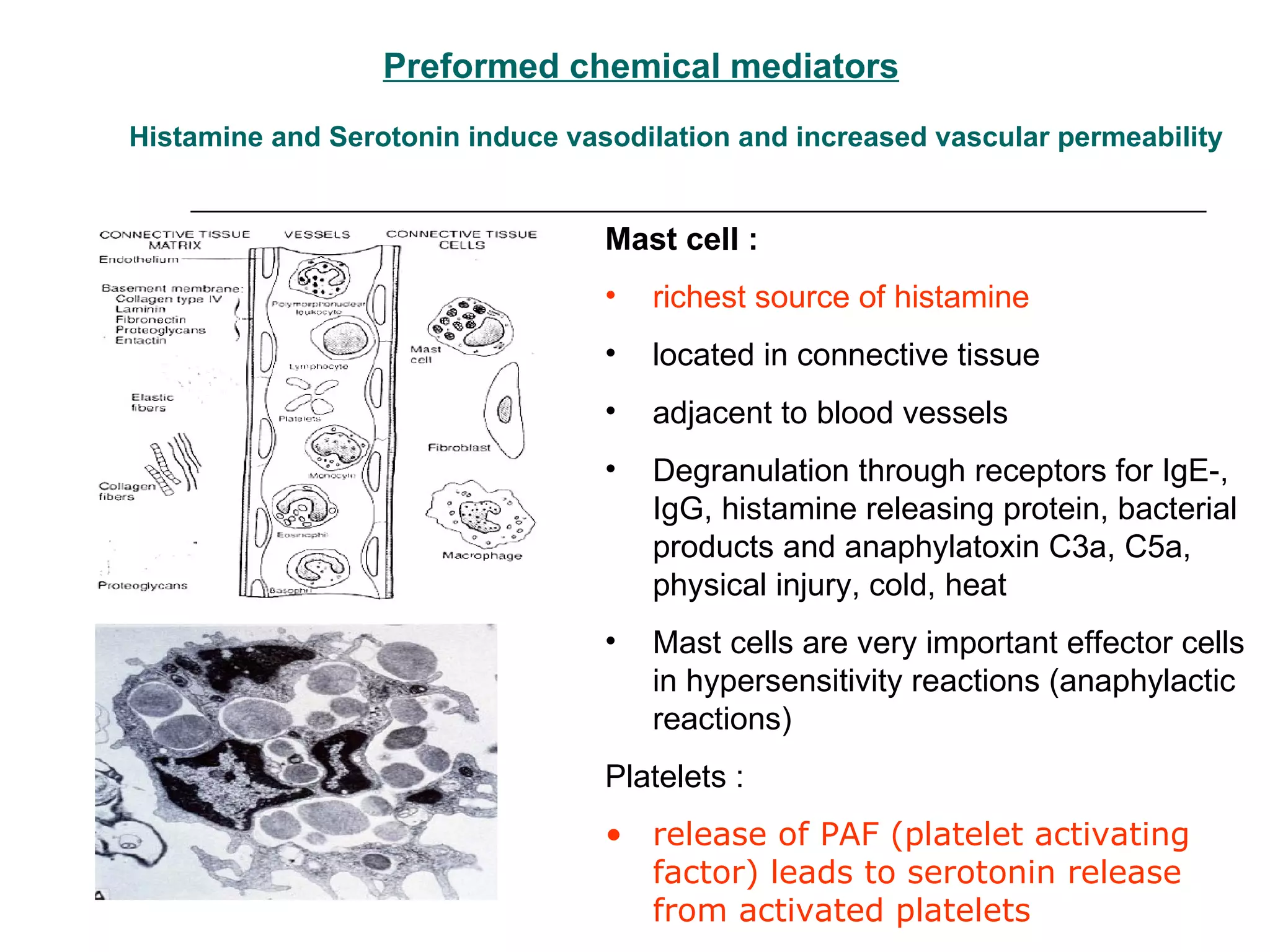
Preformed chemical mediatorsHistamine and Serotonin induce vasodilation and increased vascular permeability Mast cell : richest source of histamine located in connective tissue adjacent to blood vessels Degranulation through receptors for IgE-, IgG, histamine releasing protein, bacterial products and anaphylatoxin C3a, C5a, physical injury, cold, heat Mast cells are very important effector cells in hypersensitivity reactions (anaphylactic reactions) Platelets : release of PAF (platelet activating factor) leads to serotonin release from activated platelets
48.
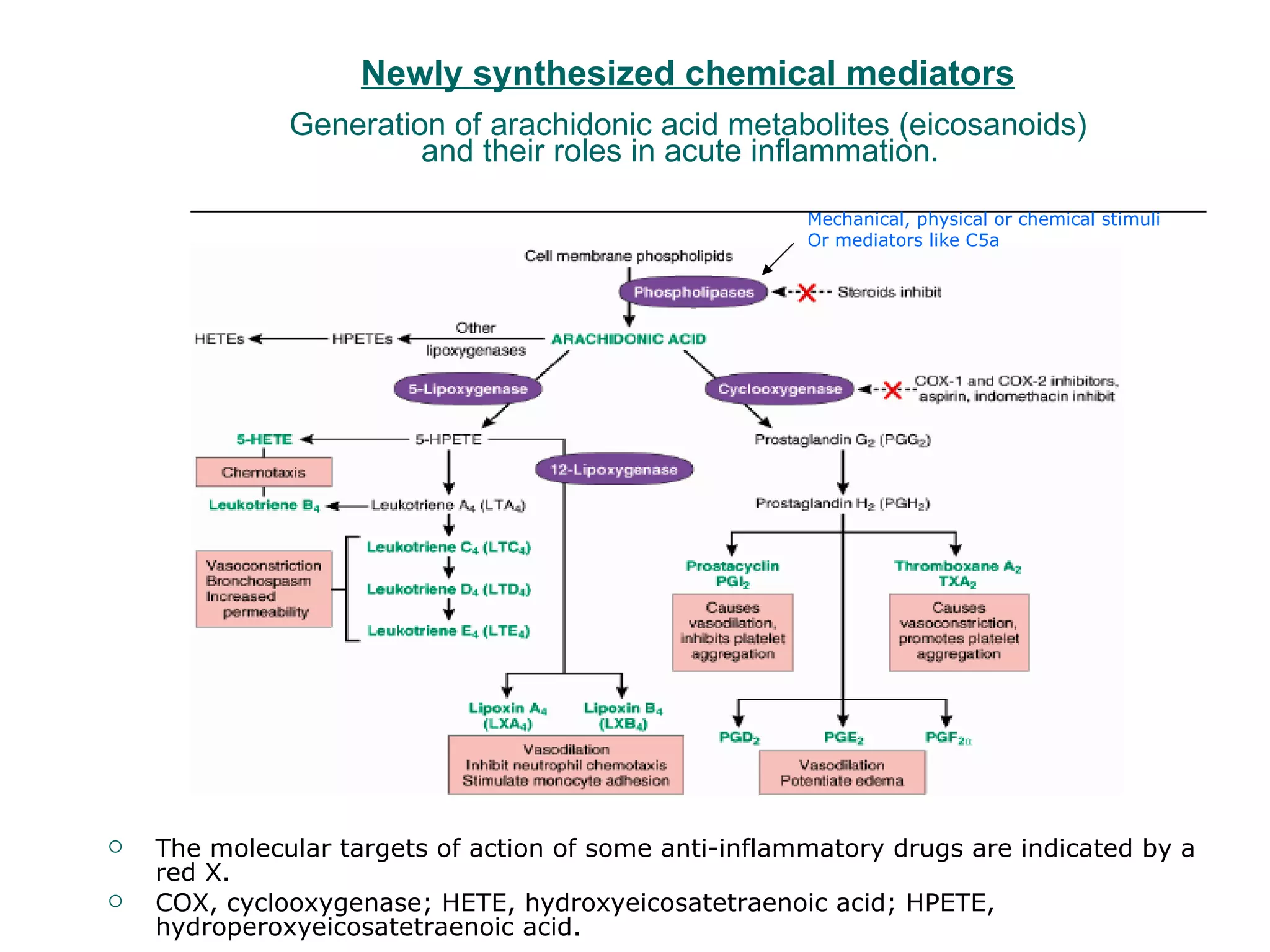
Newly synthesized chemicalmediators Generation of arachidonic acid metabolites (eicosanoids) and their roles in acute inflammation. The molecular targets of action of some anti-inflammatory drugs are indicated by a red X. COX, cyclooxygenase; HETE, hydroxyeicosatetraenoic acid; HPETE, hydroperoxyeicosatetraenoic acid. Mechanical, physical or chemical stimuli Or mediators like C5a
49.
Biosynthesis of leukotrienesand lipoxins by cell-cell interaction. AA products can pass from one cell type to another, and different cell types can co-operate with each other to generate eicosanoids (transcellular biosynthesis). Activated neutrophils generate LTB4 from arachidonic acid-derived LTA4 by the action of 5-lipoxygenase, but they do not possess LTC4 -synthase activity and consequently do not produce LTC4. In contrast, platelets cannot form LTC4 from endogenous substrates, but they can generate LTC4 and lipoxins from neutrophil-derived LTA4
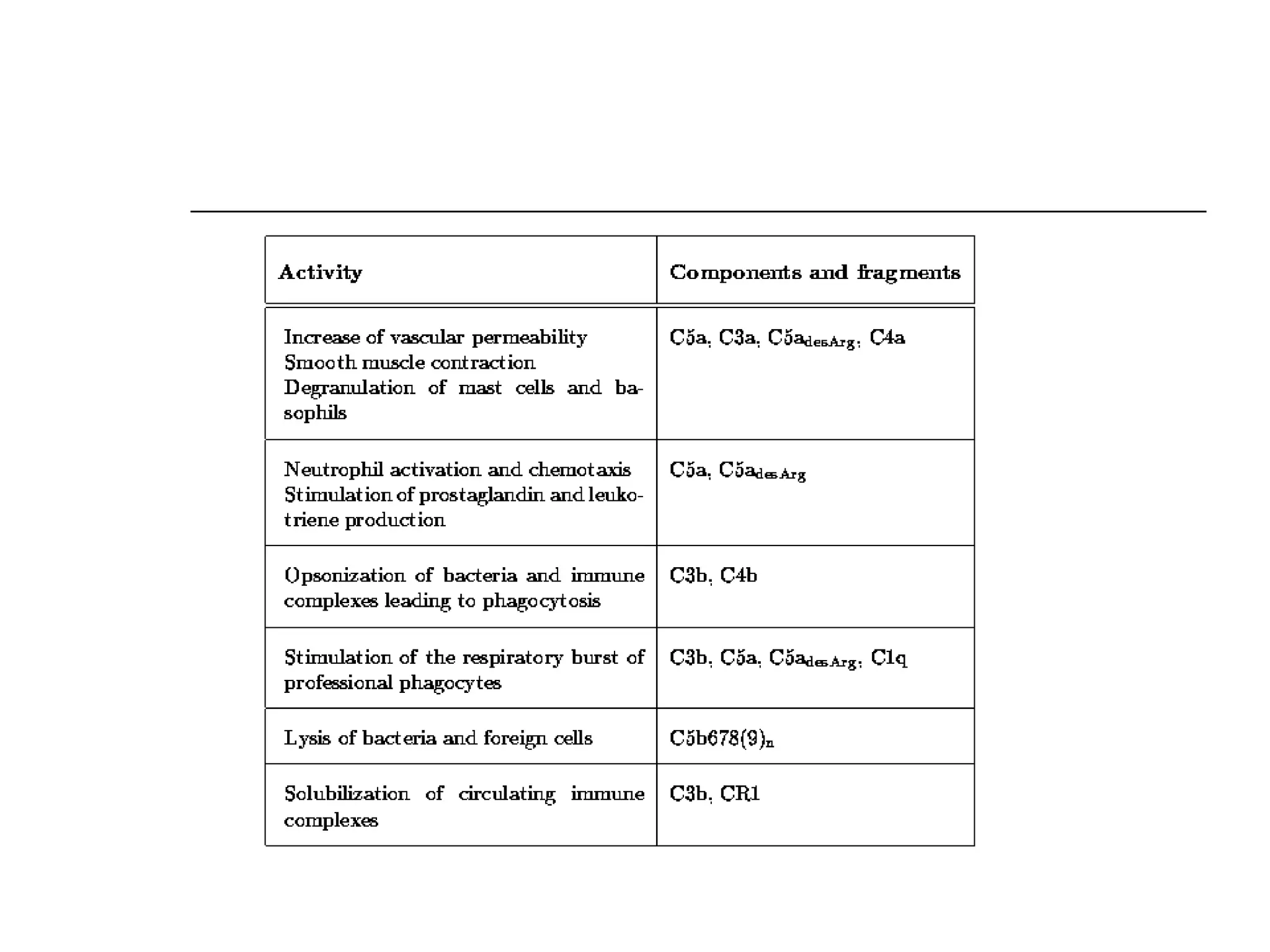
Plasma Derived mediatorsThe activation and functions of the complement system in inflammation. The most critical step is the activation of third component of complement i.e. C3. The cleavage of C3 can be brought abought by the classical, alternative or lectic pathway. Classical pathway - fixation of C1 to Ab (IgM or IgG) combined with Ag. Alternative pathway - the microbial surfaces (endotoxins). Lectin pathway - collectins bind to the carbohydrate containing proteins on bacteria and viruses and activates complement. C3 convertase splits C3 into C3a and C3b.
52.
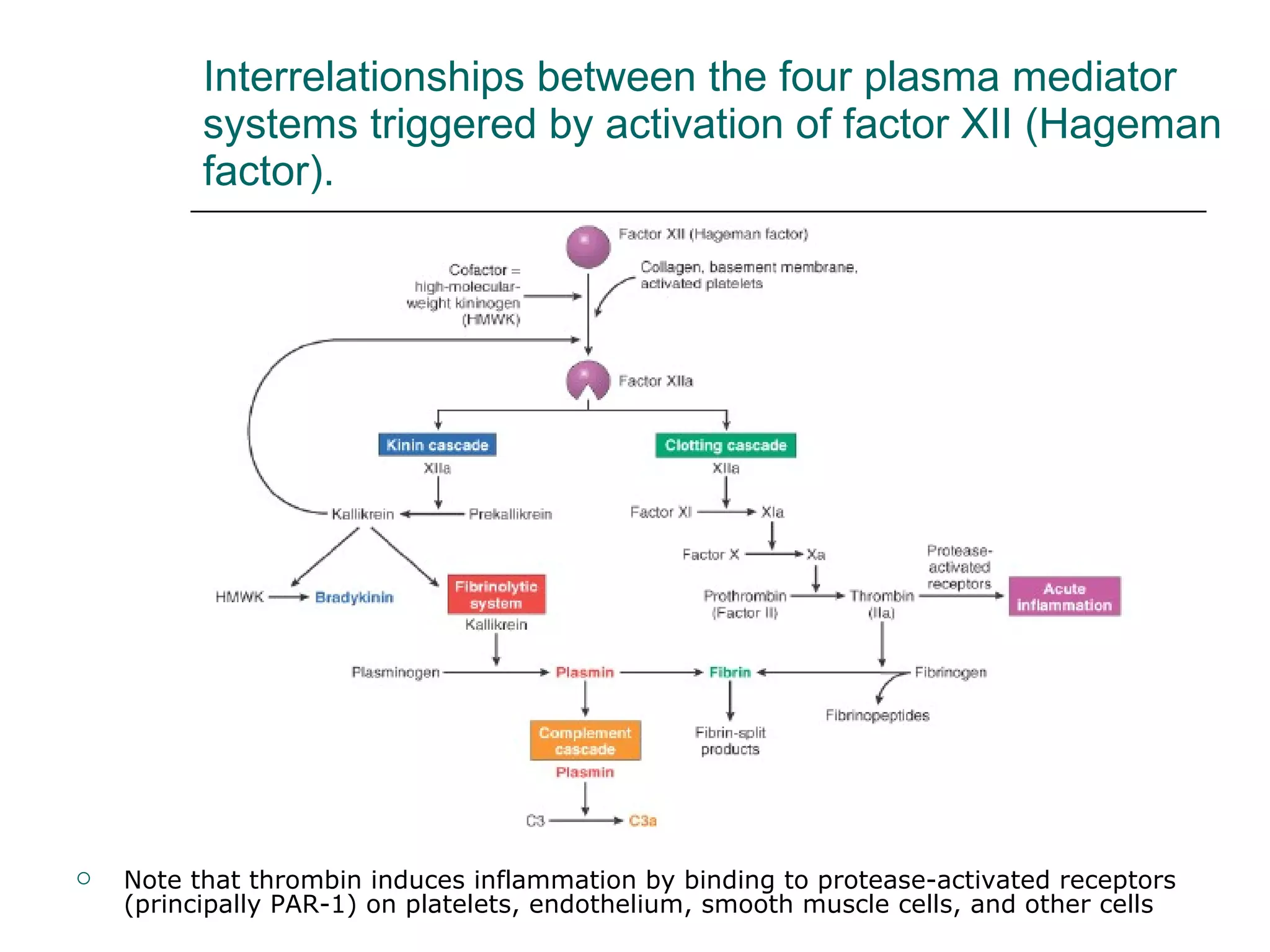
Kinin-Bradykinin System Bradykininincreases vascular permeability, contraction of smooth muscles, vasodilation and pain Kallikrein is a potent activator of factor XII, is chemotactic and can directly convert C5 to C5a (HMWK)
53.
Interrelationships between thefour plasma mediator systems triggered by activation of factor XII (Hageman factor). Note that thrombin induces inflammation by binding to protease-activated receptors (principally PAR-1) on platelets, endothelium, smooth muscle cells, and other cells
54.
55.
Major effects ofinterleukin-1 (IL-1) and tumor necrosis factor (TNF) in inflammation
56.
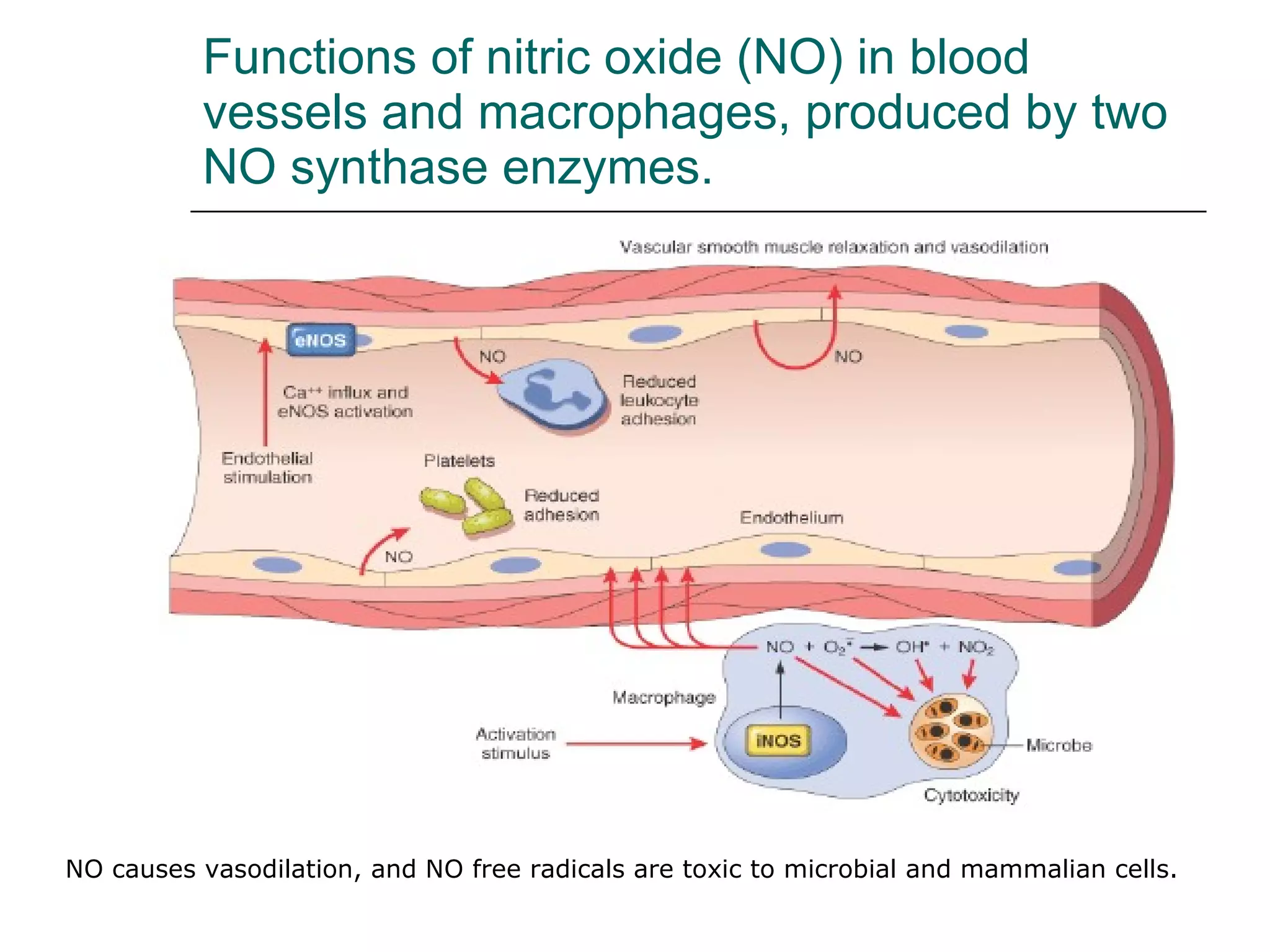
Functions of nitricoxide (NO) in blood vessels and macrophages, produced by two NO synthase enzymes. NO causes vasodilation, and NO free radicals are toxic to microbial and mammalian cells.
























































































![Inflammation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/inflammationautosaved-180806124543-thumbnail.jpg?width=640&height=640&fit=bounds)









