Downloaded 896 times
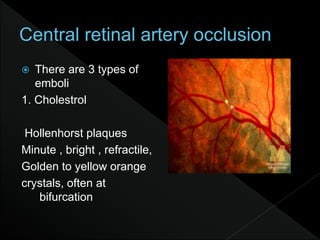
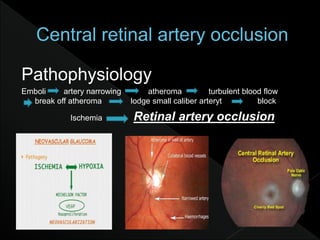
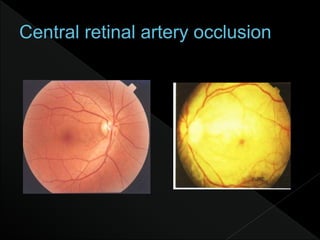
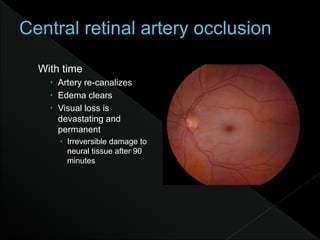
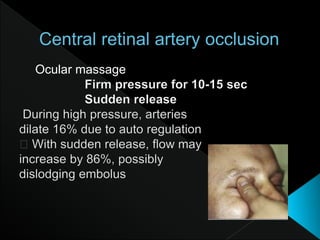
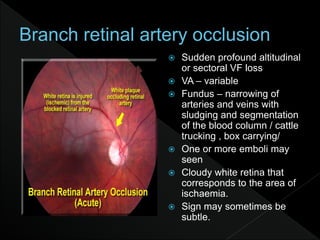
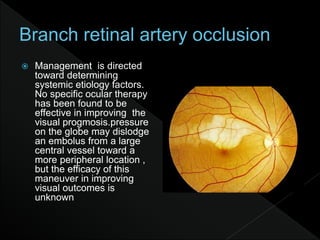
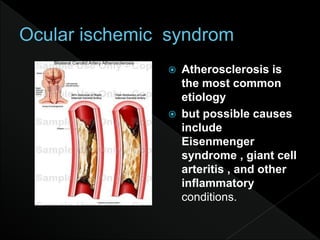

This document discusses retinal artery occlusion. Key points: - It typically affects people in their mid-60s and is more common in men. - Embolism, usually from the heart or carotid artery, is the most common cause. - Symptoms include sudden severe vision loss in one eye. On examination, the retina appears opaque and edematous with a narrowed artery. - Visual loss is usually permanent if not treated within 90 minutes. Prompt diagnosis and treatment aimed at dissolving the clot are needed to preserve vision.

















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)



