This document provides an overview of acetabular fractures including:
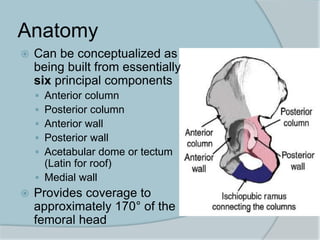
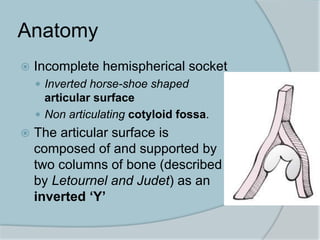
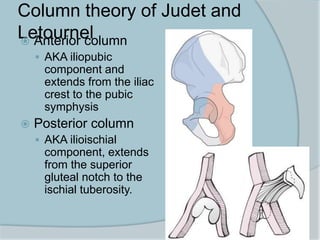
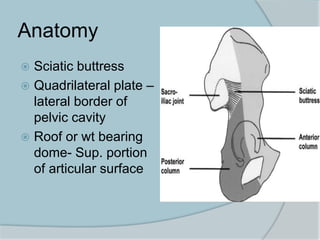
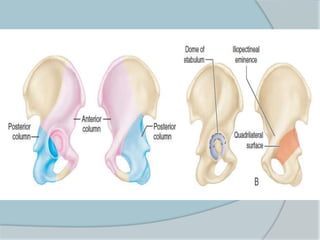
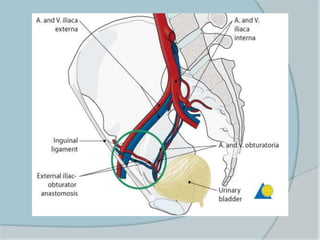
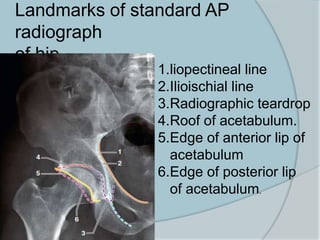
- Anatomy of the acetabulum and its components
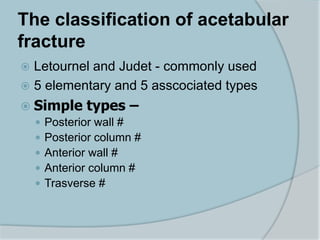
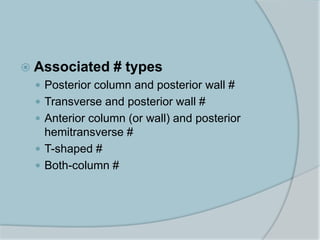
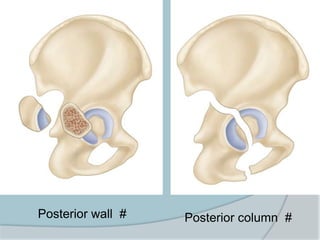
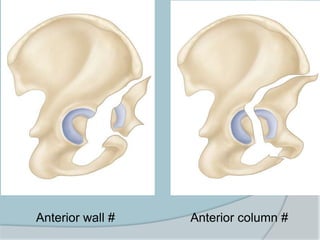
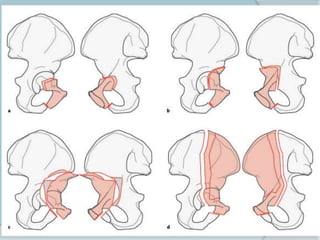
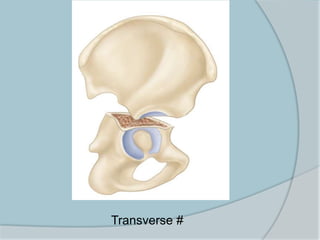
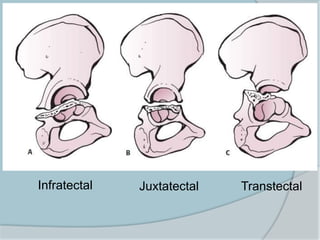
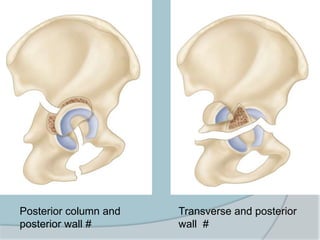
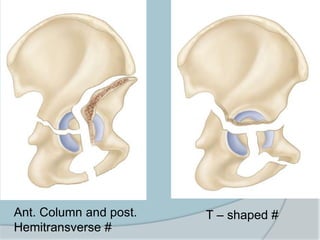
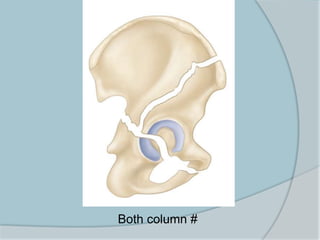
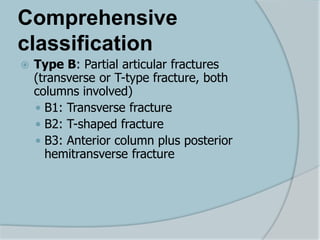
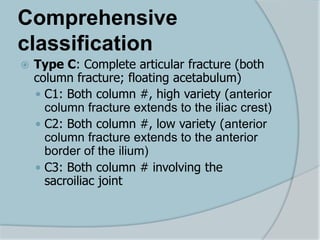
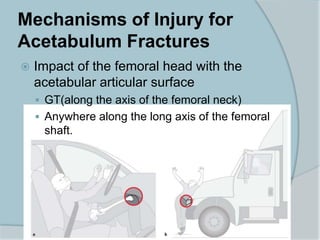
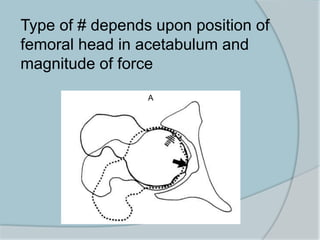
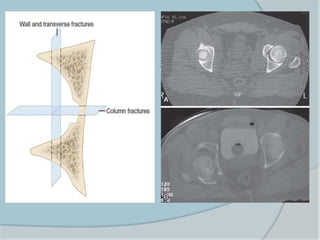
- Mechanisms and classifications of acetabular fractures
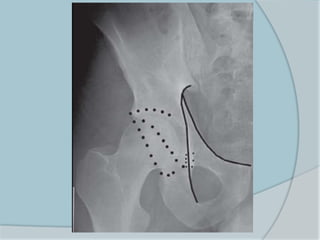
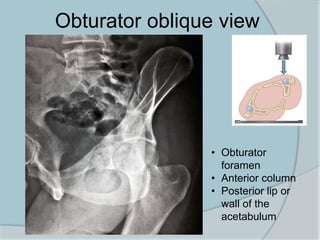
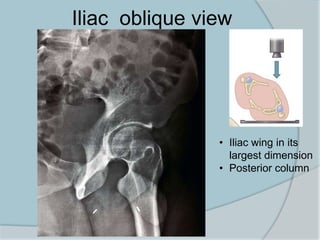
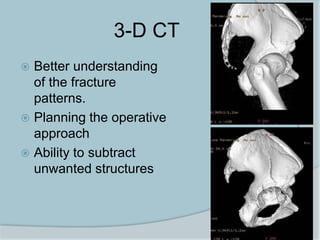
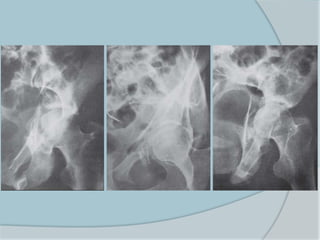
- Evaluation through radiographs and CT scans
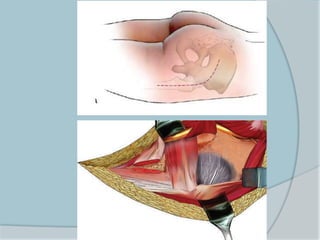
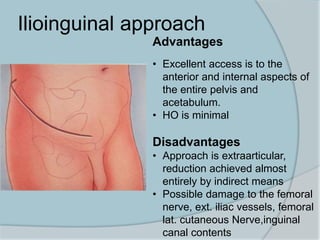
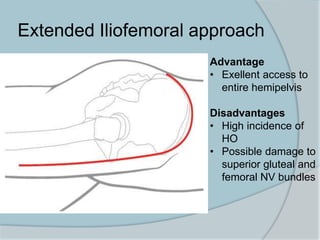
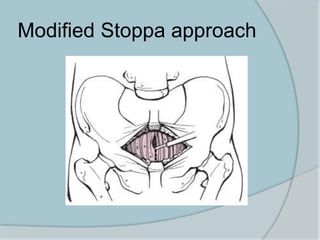
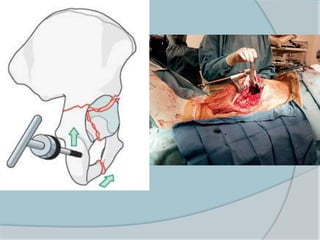
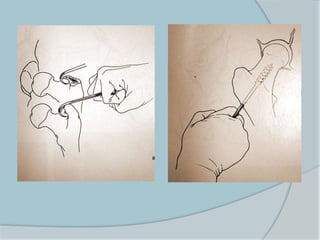
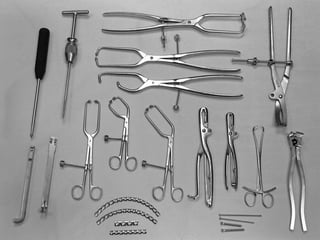
- Management considerations including operative vs non-operative treatment and various surgical approaches
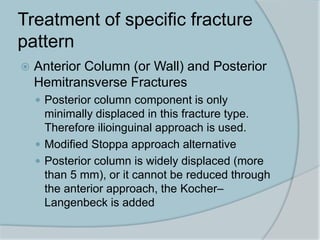
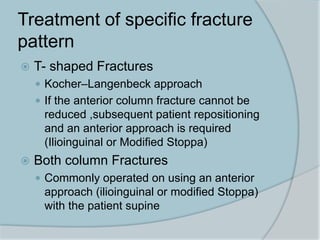
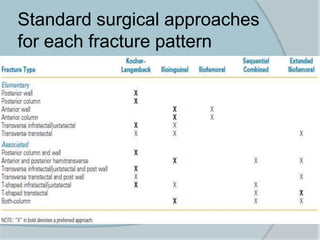
- Specifics on fracture types, indications for surgery, timing of surgery, and surgical approaches for different fractures
The document contains detailed information on evaluating and treating acetabular fractures.












































![Acetabularfracture hip fractue[1]_11[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/acetabularfracture1111-250322022902-1fed1d8a-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





