Aphasia and types
•Download as PPTX, PDF•
38 likes•17,899 views

This document provides an overview of aphasia and aphasia syndromes. It defines aphasia as an acquired language disorder resulting from brain damage. The major aphasia syndromes discussed are Broca's aphasia (nonfluent speech with relatively preserved comprehension), Wernicke's aphasia (fluent but meaningless speech with impaired comprehension), global aphasia (combination of Broca's and Wernicke's deficits), conduction aphasia (impaired repetition with otherwise intact language), and pure word deafness (isolated auditory comprehension deficit). Each syndrome is characterized by its pattern of impaired and preserved language functions as well as its associated neurological deficits and lesion location.
![INTRODUCTION
Language has provided the foundation of human
civilization and learning.
analysis of the patterns of abnormality in the language
has practical usefulness in neurological diagnosis.
Historically, language was the first higher cortical
function to be correlated with specific sites of brain
damage.
Aphasia is defined as a disorder of language that is
acquired secondary to brain damage. [Alexander and
Benson (1997)].
First, aphasia is distinguished from congenital or
developmental language disorders, called dysphasia's.](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Aphasia and types
Similar to Aphasia and types (20)
More from Manideep Malaka
More from Manideep Malaka (17)
Recently uploaded
Recently uploaded (20)
Aphasia and types
- 1. APHAISA AND APHASIA SYNDROMES
- 2. INTRODUCTION Language has provided the foundation of human civilization and learning. analysis of the patterns of abnormality in the language has practical usefulness in neurological diagnosis. Historically, language was the first higher cortical function to be correlated with specific sites of brain damage. Aphasia is defined as a disorder of language that is acquired secondary to brain damage. [Alexander and Benson (1997)]. First, aphasia is distinguished from congenital or developmental language disorders, called dysphasia's.
- 3. aphasia is a disorder of language rather than speech. language is a complex system of communication symbols and rules for their use. Speech is the articulation and phonation of language sounds. speech disorders include dysarthria, dysphonia (voice disorders), stuttering, speech apraxia. Dysarthrias are disorders of articulation of single sounds. Dysarthria may result from mechanical disturbance of the tongue or larynx or from neurological disorders.
- 4. Apraxia of speech syndrome of misarticulation of phonemes, especially consonant sounds. Dysarthria - certain phonemes are consistently distorted. apraxia of speech - inconsistent distortions and substitutions of phonemes. The disorder is called an apraxia because there is no primary motor deficit in articulation of individual phonemes. speech-apraxic patients produce inconsistent articulatory errors, usually worse on the initial phonemes of a word and with polysyllabic utterances.
- 5. LINGUISTIC COMPONENTS Phonemes are the smallest meaning-carrying sounds. morphology is the use of appropriate word endings and connector words. semantics refers to word meanings. lexicon is the internal dictionary. syntax is the grammatical construction of phrases and sentences. Discourse refers to the use of these elements to create organized and logical expression of thoughts. Pragmatics refers to the proper use of speech and language in a conversational setting including pausing while others are speaking, taking turns properly, and responding to questions
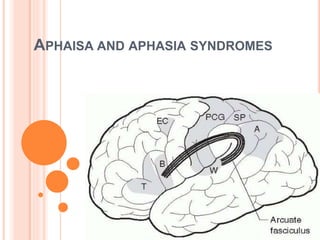
- 6. NEURO ANATOMICAL BASIS • Reception and processing of spoken language • Auditory cortex, Heschl’s gyrus, [ superior temporal gyrus]. • Wernicke’s area or Brodmann’s area 22 [ posterior part of the left superior temporal gyrus ] • Via the arcuate fasciculus • Broca’s area in the posterior inferior frontal gyrus. • Adjacent motor cortex, subserving the mouth and larynx • Brainstem cranial nerve nuclei.
- 8. The inferior parietal lobule, especially the supra marginal gyrus, involved in phoneme processing in language comprehension. phoneme production for repetition and speech. Reading requires the perception of visual language stimuli by the occipital cortex. followed by processing into auditory language information, via the heteromodal association cortex of the angular gyrus. Writing involves the activation of motor neurons projecting to the arm and hand. In addition, other cortical centers involved in cognitive processes project into the primary language cortex, influencing the content of language.
- 9. ROLE OF SUBCORTICAL STRUCTURES Thalamus: relay for the reticular activating system. appears to alert the language cortex. lesions of the dominant thalamus frequently produce fluent aphasia. Nuclei of the basal ganglia Especially the caudate nucleus and putamen, participate in expressive speech.
- 10. In right-handed people, and in a majority of left-handers, clinical syndromes of aphasia result from left hemisphere lesions. Rarely, aphasia may result from a right hemisphere lesion in a right-handed patient, a phenomenon called crossed aphasia. In left-handed persons, language disorders are usually similar to those of right-handed persons with similar lesions, but occasional cases present with atypical syndromes.
- 11. In right-handed aphasics left hemisphere lesion in 99% of the cases the other 1% are crossed aphasics. In left-handed aphasics 60% had lesions of the left hemisphere. 40% had lesions of the right hemisphere. There may be a degree of mixed dominance for language in non-right-handed individuals. Aphasia may tend to be less severe in left handers and recovery better. just a family history of left handedness in a right-handed aphasic may predict better recovery.
- 12. SYMPTOMS AND DIFFERENTIAL DIAGNOSIS OF DISORDERED LANGUAGE Muteness - a total loss of speech: May represent severe aphasia. Severe form of dysarthria. Frontal lobe dysfunction with akinetic mutism. Severe extrapyramidal system dysfunction, as in parkinson disease. Non- neurological disorders of the larynx and pharynx. Psychogenic syndromes, such as catatonia. A good rule of thumb is that if the patient can write or type and the language form and content are normal, the disorder is probably not aphasic in origin.
- 13. Hesitant speech: symptom of aphasia, symptom of dysarthria or stuttering, psychogenic disorder rule of thumb is that if one can transcribe the utterances of a hesitant speaker into normal language, the patient is not aphasic. Anomia: inability to produce a specific name. generally a reliable indicator of language disorder. it may also reflect memory loss.
- 14. Paraphasic speech: refers to the presence of errors in the patient’s speech output. literal or phonemic errors: involving substitution of an incorrect sound (e.g., shoon for spoon), verbal or semantic errors: involving substitution of an incorrect word (e.g., fork for spoon). Perseveration: The inappropriate repetition of a previous response. Neologisms: aphasic utterances involve non existent word forms. A pattern of paraphasic errors and neologisms that so contaminate speech that the meaning cannot be discerned is called jargon speech.
- 15. Fluent, paraphasic speech: differential diagnosis here involves Aphasia, Psychosis, Acute encephalopathy or delirium, Dementia. Aphasic patients are usually not confused or inappropriate in behavior. they do not appear agitated or misuse objects, with occasional exceptions. By contrast, most psychotic patients speak in an easily understood, grammatically appropriate manner, but their behavior and speech content are abnormal. Only rarely do schizophrenics speak in “clang association” or “word salad” speech.
- 16. BEDSIDE LANGUAGE EXAMINATION A wealth of information about language function can be obtained during the clinical interview. D. Frank Benson and Norman Geschwind popularized a bedside language examination of six parts, updated by Alexander and Benson (1997).
- 17. Spontaneous speech: Fluent speech flows rapidly and effortlessly. Non fluent speech is uttered in single words or short phrases, with frequent pauses and hesitations. 1st observe the elementary characteristics such as initiation difficulty, articulation, phonation or voice volume, rate of speech, prosody or melodic intonation of speech, phrase length. 2nd the content of speech utterances should be analyzed in terms of the presence of word-finding pauses, circumlocutions, and errors such as literal and verbal paraphasias and neologisms.
- 18. Naming: tested by asking the patient to name objects, object parts, pictures, colors, or body parts to confrontation. A few items from each category should be tested. Proper names of persons are often affected severely. The examiner should ensure that the patient recognizes the items or people that he or she cannot name.
- 19. Auditory comprehension: Is tested by asking the patient to follow a series of commands of one, two, and three steps. An example of a one-step command is “stick out your tongue”. a two-step command is “hold up your left thumb and close your eyes.” Successful following of commands ensures adequate comprehension but not vise versa.
- 20. The patient must hear the command, understand the language the examiner speaks, and possess the motor ability to execute it, including the absence of apraxia. Because apraxia is difficult to exclude with confidence, it is advisable to test comprehension by tasks that do not require a motor act, such as yes- no questions
- 21. Repetition: Dysarthric patients have difficulty with rapid sequences of consonants. Aphasics have special difficulty with grammatically complex sentences. Often, aphasics can repeat familiar phrases much better than unfamiliar ones. Reading: Should be tested both aloud and for comprehension. The examiner should carry a few printed commands to facilitate a rapid comparison of auditory to reading comprehension. Examiner must have some idea of the patient’s pre morbid reading ability
- 22. Writing: The element of the bedside examination most often omitted. A writing specimen may be the most sensitive indicator of mild aphasia, and it provides a permanent record for future comparison. Spontaneous writing, such as a sentence describing why the patient has come for examination, is especially sensitive for the detection of language difficulty. When spontaneous writing fails, writing to dictation and copying should be tested.
- 23. Finally, combine the results of the bedside language examination with those of the rest of the neurological examination. These “associated signs” help to classify the type of aphasia and to localize the responsible brain lesion
- 24. DIFFERENTIAL DIAGNOSIS OF APHASIC SYNDROMES
- 25. BROCA’S APHASIA Paul Broca, the French physician described in 1861. The speech pattern is non fluent. If the maximum sentence length is fewer than seven words, then the patient is nonfluent. Patient speaks hesitantly, often producing the principal, meaning-containing nouns and verbs but omitting small grammatical words. An example is “wife come hospital.”
- 26. “Agrammatism” or “telegraphic speech”. They make many phonemic errors, with substitution of phonemes usually differing only slightly from the correct target. Naming is deficient, but the patient often manifests a “tip of the tongue” phenomenon. Auditory comprehension seems intact. Repetition is hesitant in these patients, resembling their spontaneous speech. Reading is often impaired despite relatively preserved auditory comprehension
- 27. Benson termed this reading difficulty of Broca aphasics the “third alexia,” in distinction to the two classical types of alexia. Writing is virtually always deficient in Broca aphasics. Associated neurological deficits of Broca aphasia include right hemiparesis, hemisensory loss, apraxia of the oral apparatus and the nonparalyzed left limbs. An important clinical feature of Broca aphasia is its frequent association with depression. The lesions site - Broca area in the posterior part of the inferior frontal gyrus.
- 28. In CT scan analyses at the Boston Veterans Administration Medical Center, lesions combining Broca area, the lower pre central gyrus, and sub cortical white matter yielded the full syndrome of Broca aphasia. In studies by the same group, damage to two subcortical white matter sites the rostral sub callosal fasciculus deep to the Broca area and the periventricular white matter adjacent to the body of the left lateral ventricles - were required to cause permanent non fluency.
- 31. APHEMIA A rare variant of Broca aphasia. Non fluent syndrome. Patient is initially mute and then able to speak with phoneme substitutions and pauses. All other language functions are intact, including writing. usually transitory syndrome results from small lesions of the Broca area or its sub cortical white matter or of the inferior pre central gyrus. because written expression and auditory comprehension are normal, aphemia is not a true language disorder. aphemia may be equivalent to pure apraxia of speech.
- 32. WERNICKE APHASIA syndrome opposite to Broca aphasia. expressive speech is fluent. The speech pattern is effortless and sometimes even excessively fluent (logorrhea). Neurolinguists refer to this pattern as paragrammatism. In milder cases, the intended meaning of an utterance may be discerned. Naming is deficient, often with bizarre, paraphasic substitutions for the correct name.
- 33. Auditory comprehension is impaired, sometimes even for simple nonsense questions. Repetition is impaired. Reading comprehension is usually affected similarly to auditory comprehension, but occasional patients show greater deficit in one modality versus the other. Writing is also impaired. The patient usually has no hemiparesis and can grasp the pen. Written productions are even more abnormal than oral ones. Writing samples are especially useful in the detection of mild Wernicke aphasia.
- 34. Associated signs are limited in Wernicke aphasia. most patients have no elementary motor or sensory deficits. partial or complete right homonymous hemianopia may be present. The psychiatric manifestations of Wernicke aphasia are quite different. Some patients become angry or paranoid about the inability of family members and medical staff to understand them.
- 35. Lesion site - posterior portion of the superior temporal gyrus, sometimes extending into the inferior parietal lobule. Extension of the lesion into the inferior parietal region may predict greater involvement of reading comprehension. In terms of vascular anatomy, the Wernicke area lies within the territory of the inferior division of the left middle cerebral artery.
- 39. PURE WORD DEAFNESS Isolated loss of auditory comprehension and repetition, without any abnormality of speech, naming, reading, or writing. Hearing for pure tones and for nonverbal noises, such as animal cries, is intact. Classically, the anatomical substrate is a bilateral lesion, isolating Wernicke’s area from the primary auditory cortex, in the bilateral Heschl’s gyri.
- 40. Pure word deafness is thus an example of a “disconnection syndrome,” deficit results from loss of white matter connections rather than of gray matter language centers. Some cases are d/t unilateral, left temporal lesions.
- 41. GLOBAL APHASIA summation of the deficits of Broca aphasia and Wernicke aphasia. Speech is nonfluent or mute, but comprehension is also poor, as are naming, repetition, reading, and writing. Most patients have dense right hemiparesis, hemisensory loss, and often hemianopia.
- 42. Lesion site: Inferior frontal and superior temporal regions, and often much of the parietal lobe in between. Left middle cerebral artery territory. Recovery in global aphasia may be prolonged. Global aphasics may recover more during the second 6 months than during the first 6 months after a stroke.
- 44. CONDUCTION APHASIA Characterized by its striking deficit in repetition. Most patients have relatively normal spontaneous speech, although some make literal paraphasic errors and hesitate frequently for self-correction. Auditory comprehension is preserved. Naming may be impaired. Reading and writing are somewhat variable, but reading aloud may share some of the same difficulty as repeating.
- 45. Associated deficits include hemianopia in some patients right-sided sensory loss may be present right hemiparesis is usually mild or absent. Some patients have limb apraxia, creating a misimpression that comprehension is impaired. The lesions of conduction aphasia usually involve either the superior temporal or inferior parietal regions. Benson and associates suggested that patients with limb apraxia have parietal lesions, whereas those without apraxia have temporal lesions.
- 46. Wernicke originally postulated that a lesion disconnecting the Wernicke and Broca areas would produce this syndrome. Geschwind later pointed to the arcuate fasciculus, a white matter tract traveling from the deep temporal lobe, around the sylvian fissure to the frontal lobe, as the site of disconnection. Anatomical involvement of the arcuate fasciculus is present in most, if not all, cases of conduction aphasia.
- 48. ANOMIC APHASIA Naming or access to the internal lexicon, is the principal deficit. Spontaneous speech is normal except for the pauses produced by the inability to name. Comprehension, repetition, reading, and writing are intact, except for the same word-finding difficulty in written productions. less specific in localization than other aphasic syndromes.
- 49. Isolated, severe anomia may indicate focal left hemisphere pathology. Inability to produce nouns → temporal lobe lesions Inability to produce verbs → frontal lobe lesions Alexander and Benson (1997) refer to the angular gyrus as the site of lesions producing anomic aphasia. but lesions there usually produce other deficits, including alexia and the four elements of Gerstmann syndrome.
- 50. Anomia is also seen with mass lesions elsewhere in the brain, diffuse degenerative disorders, such as Alzheimer disease. Anomic aphasia is also a common stage in the recovery of many aphasic syndromes. Anomic aphasia thus serves as an indicator of left hemisphere or diffuse brain disease, but it has only limited localizing value.
- 52. TRANS CORTICAL APHASIA’S Syndromes in which repetition is normal. causative lesions do not disrupt the peri sylvian language circuit. lesions disrupt connections from other cortical centers into the language circuit hence the name “transcortical” .
- 53. Mixed transcortical aphasia: Global aphasia in which the patient repeats, often echolalically, but has no propositional speech or comprehension. Occurring predominantly in large, watershed infarctions of the left hemisphere or both hemispheres that spare the perisylvian cortex or in advanced dementias. Trans cortical sensory aphasia: Is an analogue of wernike aphasia but repetition is fluent. occurring in strokes of the left temporo-occipital area and in dementias
- 54. Trans cortical motor aphasia: Is an analogue of Broca aphasia but repetition is fluent. Occurs with lesions in the frontal lobe, anterior to the Broca area, deep frontal white matter, medial frontal region, vicinity of the supplementary motor area. All of these lesion sites are within the territory of the anterior cerebral artery.
- 56. SUB CORTICAL APHASIAS Defined by lesion localization in the basal ganglia or deep cerebral white matter. two major groups: Aphasia with thalamic lesions Aphasia with lesions of the subcortical white matter and basal ganglia.
- 57. Aphasia with thalamic lesions Left thalamic hemorrhages frequently produce a Wernicke like fluent aphasia. better comprehension than cortical Wernicke aphasia. fluctuating or “dichotomous” state has been described. consists of alternating alert state and a drowsy state. some have attributed thalamic aphasia to pressure on adjacent structures and secondary effects on the cortex.
- 58. Thalamic aphasia also occurs with small ischemic lesions Involving paramedian or anterior nuclei of the thalamus in the territory of the tubero thalamic artery indicate that the thalamus and its connections play a definite role in language function. Thalamic aphasia can occur even with a right thalamic lesion in a left handed patient.
- 59. LESIONS OF THE LEFT BASAL GANGLIA AND DEEP WHITE MATTER first described in basal ganglia hemorrhages, especially those involving the putamen. most commonly involve global or Wernicke like aphasia. ischemic strokes have provided better localizing information. posterior sub cortical aphasia syndrome Involving the posterior putamen and deep temporal white matter [temporal isthmus]. Fluent, paraphasic speech and impaired comprehension resembling Wernicke aphasia
- 60. Anterior sub cortical aphasia syndrome: lesion is an infarct involving the anterior putamen, caudate nucleus, and anterior limb of the internal capsule. dysarthria, decreased fluency, mildly impaired repetition, and mild comprehension disturbance. closely resembles Broca aphasia, but with greater dysarthria and less language dysfunction.
- 61. o Larger sub cortical lesions involving both the anterior and posterior lesion sites produce global aphasia. o basal ganglia lesions affect language, both directly and indirectly, via decreased activation of cortical language areas o In summary, sub cortical lesions do produce aphasia less commonly than cortical lesions language characteristics of sub cortical aphasias are often atypical.
- 62. PURE ALEXIA WITHOUT AGRAPHIA Alexia is an acquired inability to read. pure alexia without agraphia - described by the French neurologist Dejerine in 1892. Characterized by “linguistic blindfolding” Patients can write but cannot read their own writing. Spontaneous speech, auditory comprehension, and repetition are normal. Naming may be deficient, especially for colors.
- 63. Associated deficits include a right hemianopia or right upper quadrant defect in nearly all patients. Frequently, a deficit of short term memory. There is usually no hemiparesis or sensory loss. nearly always a stroke in the territory of the left posterior cerebral artery, with infarction of the medial occipital lobe, often the splenium of the corpus callosum and medial temporal lobe. Dejerine postulated a disconnection between the intact right visual cortex and left hemisphere language centers, particularly the angular gyrus.
- 66. ALEXIA WITH AGRAPHIA described by Dejerine in 1891. Is an acquired illiteracy, in which a previously educated patient is rendered unable to read or write. Spantanous speech, naming, auditory comprehension, and repetition are largely intact. but many cases manifest a fluent, paraphasic speech pattern with impaired naming. This syndrome thus overlaps with Wernicke aphasia.
- 67. Associated deficits include right hemi anopia and elements of Gerstmann syndrome. The lesions typically involve the inferior parietal lobule, especially the angular gyrus. Etiologies include strokes in the territory of the angular branch of the left middle cerebral artery or mass lesions in the same region.
- 69. Aphasic Alexia: many patients with aphasia have associated reading disturbance. These are “third alexia” syndrome of Broca’s aphasia and the reading deficit of Wernicke’s aphasia. Agraphia: Like reading, writing may be affected either in isolation (pure agraphia) or in association with aphasia (aphasic agraphia). In addition, writing can be impaired by motor disorders, by apraxia and by visuospatial deficits. Isolated agraphia has been described with left frontal or parietal lesions.
- 70. LANGUAGE IN RIGHT HEMISPHERE DISORDERS Left-handed patients→ right hemisphere language dominance → aphasia from right hemisphere lesions. Right-handed patients → become aphasic after right hemisphere strokes → crossed aphasia. Right-handed persons → left hemisphere dominance → subtly altered language function after right hemisphere damage → aprosodia. .
- 71. Aprosodia Fundamental mechanisms of speech are undisturbed. Affective aspects of language are impaired. Normal prosody or emotional intonation of speech is lost. Motor aprosodia involves loss of expressive emotion with preservation of emotional comprehension. sensory aprosodia Involves loss of comprehension of affective language. also called affective agnosia. In other words, right hemisphere-damaged patients understand what is said, but not how it is said.
- 72. LANGUAGE IN DEMENTING DISEASES Alzheimer disease (AD): Patients with early AD have anomic aphasia. In later stages, language functions become more obviously impaired. Reading and writing the last learned language functions are among the first to decline. Auditory comprehension later becomes deficient, whereas repetition and articulation remain normal.
- 73. The language profile may then resemble that of transcortical sensory or Wernicke aphasia. In terminal stages, speech is reduced to the expression of simple biological wants. eventually, even muteness can develop. Primary progressive aphasia (PPA): Varient of fronto temporal dementia (FTD). Fronto temporal dementia is now divided into four subgroups: behavioral variant FTD progressive nonfluent aphasia semantic dementia logopenic primary progressive aphasia.
- 74. progressive non fluent aphasia: Broca-like pattern of aphasia involving agrammatism and apraxia of speech. Usually reflects a “tauopathy”. Mutations in familial cases found in the tau gene on Ch 17.
- 75. Semantic dementia: progressive fluent aphasia with impaired naming and loss of understanding of even single words. In reading, they may have a surface alexia pattern. Not a tauopathy Progranulin mutation on Ch 17 with production of an abnormal protein called TDP-43. Logopenic primary progressive aphasia: involves anomia and some repetition difficulty, with intact single word comprehension.
- 76. MRI - different patterns of atrophy. Progressive non fluent aphasia → left frontal and insular atrophy. Semantic dementia → bilateral anterior temporal atrophy. Logopenic progressive aphasia → posterior temporal and inferior parietal atrophy. Cortico basal degeneration can also present with language abnormalities. Isolated aphasia secondary to Creutzfeldt–Jakob disease have been reported, but these usually progress to dementia over a period of months.
- 77. INVESTIGATION OF THE APHASIC PATIENT The bedside language examination is useful in forming a preliminary impression of the type of aphasia and the localization of the causative lesion. large number of standardized aphasia test batteries have been published. They have the advantage of quantitation and standardization, permitting comparison over time. most helpful battery is the Boston Diagnostic Aphasia Examination, or its Canadian adaptation, the Western Aphasia Battery.
- 78. Further diagnosis of the aphasic patient rests on the confirmation of a brain lesion by neuro imaging. MRI is the better modality than CT. In preparation for epilepsy surgery, the Wada test, or infusion of amobarbital through an arterial catheter, is useful in the determination of language dominance. Single-photon emission CT (SPECT), PET, and functional MRI are contributing greatly to the study of language.
- 79. fMRI study showed Hypo metabolism in the language cortex shortly after an ischemic insult. followed by increased activation of homologous areas in the contra lateral hemisphere. then a shift back to the more normal pattern of left hemisphere activation.
- 80. DIFFERENTIAL DIAGNOSIS 1. Ischemic strokes: bedside aphasia examination is helpful in delineating the vascular territory affected. Wernicke aphasia → inferior division of the left MCA. Global aphasia → left MCA stem / ICA. Trans cortical motor aphasia → left ACA territory. pure alexia without agraphia → left PCA territory. 2. Hemorrhagic strokes: most commonly the basal ganglionic hemorrhages. Recovery was better with hemorragic strokes. .
- 81. 3. Traumatic brain injury: Cerebral contusions, depressed skull fractures, and hematomas of the intra cerebral, subdural, and epidural spaces all cause aphasia when they disrupt or compress left hemisphere language structures. 4. Tumors of the left hemisphere: onset of the aphasia is gradual. other cognitive deficits may be associated because of edema and mass effect. 5. Degenerative diseases: Alzheimer disease / FTD Cortico basal degeneration
- 82. 6. Infections: Brain abscesses can mimic tumors in every respect. Chronic infections, such as tuberculosis or syphilis, can result in focal abnormalities. Herpes simplex encephalitis has a predilection for the temporal lobe and orbital frontal cortex and aphasia can be an early symptom. AIDS - Opportunistic infections / AIDS dementia complex. 7. Seizures: Associated with aphasia in children as part of the Landau– Kleffner syndrome or in adults as either an ictal or post ictal Todd phenomenon. Epileptic aphasia is important to recognize because anticonvulsant drug therapy can prevent the episodes.
- 83. 8. Migraine: Another transitory cause of aphasia. Wernicke aphasia may be seen in a migraine attack, usually with complete recovery over a few hours. 9. Psychogenic: often associated with stuttering or stammering.
- 84. RECOVERY AND REHABILITATION OF APHASIA Patients with aphasia from acute disorders, such as stroke, generally show spontaneous improvement over days, weeks and months. In general, the greatest recovery occurs during the first 3 months, but improvement may continue over a prolonged period, especially in young patients and in global aphasics The aphasia type often changes during recovery. Global aphasia evolves into Broca aphasia, and Wernicke aphasia into conduction or anomic aphasia.
- 85. Language recovery may be mediated by shifting of functions to the right hemisphere or to adjacent left hemisphere regions. aphasia recovers best when left hemisphere areas, recover function. Right hemisphere activation seems to be a “second best” type of recovery. Speech therapy, provided by speech-language pathologists, attempts to facilitate language recovery by a variety of techniques.
- 86. Repeated practice in articulation and comprehension tasks has traditionally been used to stimulate improvement. Other techniques include melodic intonation therapy → which uses melody to involve the right hemisphere in speech production. visual action therapy → which uses gestural expression. Two other therapeutic techniques are functional communication therapy →takes advantage of extra linguistic communication cVIC or Lingraphica → a computer program originally developed for primate communication.
- 87. Speech therapy has remained somewhat controversial, but evidence of efficacy is actually better for speech therapy than for many drugs. A new approach to language rehabilitation is the use of pharmacological agents to improve speech. first reported that the dopaminergic drug bromocriptine promotes spontaneous speech output in transcortical motor aphasia. Stimulant drugs are also being tested in aphasia rehabilitation.
- 88. Finally, stimulation techniques such as trans cranial magnetic stimulation and direct cortical stimulation are being applied to patients with aphasia. These techniques await validation by larger clinical trials.