Disha NEET Physics Guide for classes 11 and 12.pdf
Nephro
1. Practice Essentials
Nephrolithiasis specifically refers to calculi in the kidneys, but renal calculi and ureteral calculi
(ureterolithiasis) are often discussed in conjunction. The majority of renal calculi contain calcium.
The pain generated by renal colic is primarily caused by dilation, stretching, and spasm because of
the acute ureteral obstruction.
Signs and symptoms
The classic presentation for a patient with acute renal colic is the sudden onset of severe pain
originating in the flank and radiating inferiorly and anteriorly; at least 50% of patients will also have
nausea and vomiting. Patients with urinary calculi may report pain, infection, or hematuria
Urinary calculi are solid particles in the urinary system. They may cause pain, nausea, vomiting,
hematuria, and, possibly, chills and fever due to secondary infection. Diagnosis is based on
urinalysis and radiologic imaging, usually noncontrast helical CT. Treatment is with analgesics,
antibiotics for infection, medical expulsive therapy, and, sometimes, shock wave lithotripsy or
endoscopic procedures.
The location and characteristics of pain in nephrolithiasis include the following:
Stones obstructing ureteropelvic junction: Mild to severe deep flank pain without radiation to the
groin; irritative voiding symptoms (eg, frequency, dysuria); suprapubic pain, urinary
frequency/urgency, dysuria, stranguria, bowel symptoms
Stones within ureter: Abrupt, severe, colicky pain in the flank and ipsilateral lower abdomen;
radiation to testicles or vulvar area; intense nausea with or without vomiting
Upper ureteral stones: Radiate to flank or lumbar areas
Midureteral calculi: Radiate anteriorly and caudally
Distal ureteral stones: Radiate into groin or testicle (men) or labia majora (women)
Stones passed into bladder: Mostly asymptomatic; rarely, positional urinary retention
Diagnosis
The diagnosis of nephrolithiasis is often made on the basis of clinical symptoms alone, although
confirmatory tests are usually performed.
Examination in patients with nephrolithiasis includes the following findings:
Dramatic costovertebral angle tenderness; pain can move to upper/lower abdominal quadrant with
migration of ureteral stone
Generally unremarkable abdominal evaluation: Possibly hypoactive bowel sounds; usually absence
of peritoneal signs; possibly painful testicles but normal-appearing
Constant body positional movements (eg, writhing, pacing)
Tachycardia
Hypertension
Microscopic hematuria
2. Testing
The European Association of Urology (EAU) recommends the following laboratory tests in all
patients with an acute stone episode
Urinary sediment/dipstick test: To demonstrate blood cells, with a test for bacteriuria (nitrite) and
urine culture in case of a positive reaction
Serum creatinine level: To measure renal function
Other laboratory tests that may be helpful include the following:
CBC with differential in febrile patients
Serum electrolyte assessment in vomiting patients (eg, sodium, potassium, calcium, PTH,
phosphorus)
Serum and urinary pH level: May provide insight regarding patient’s renal function and type of
calculus (eg, calcium oxalate, uric acid, cystine), respectively
Microscopic urinalysis
24-Hour urine profile
Imaging studies
The following imaging studies are used in the evaluation of nephrolithiasis:
Noncontrast abdominopelvic CT scan: The imaging modality of choice for assessment of urinary
tract disease, especially acute renal colic
Renal ultrasonography: To determine presence of a renal stone and the presence of
hydronephrosis or ureteral dilation; used alone or in combination with plain abdominal radiography
Plain abdominal radiograph (flat plate or KUB): To assess total stone burden, as well as size, shape,
composition, location of urinary calculi; often used in conjunction with renal ultrasonography or CT
scanning
IVP (urography) (historically, the criterion standard): For clear visualization of entire urinary system,
identification of specific problematic stone among many pelvic calcifications, demonstration of
affected and contralateral kidney function
Plain renal tomography: For monitoring a difficult-to-observe stone after therapy, clarifying stones
not clearly detected or identified with other studies, finding small renal calculi, and determining
number of renal calculi present before instituting a stone-prevention program
Retrograde pyelography: Most precise imaging method for determining the anatomy of the ureter
and renal pelvis; for making definitive diagnosis of any ureteral calculus
Nuclear renal scanning: To objectively measure differential renal function, especially in a dilated
system for which the degree of obstruction is in question; reasonable study in pregnant patients, in
whom radiation exposure must be limited
Management
Supportive care and pharmacotherapy
Medical treatment of nephrolithiasis involves supportive care and administration of agents, such as
the following:
Acute Stone Attacks (Renal Colic):
IV hydration
NSAIDS (eg, ketorolac, ketorolac intranasal, ibuprofen)
Nonnarcotic analgesics (eg, APAP)
PO/IV narcotic analgesics (eg, codeine, morphine sulfate, oxycodone/APAP, hydrocodone/APAP,
dilaudid, fentanyl)
Alpha blockers (eg, tamsulosin, terazosin)
Antiemetics (eg, metoclopramide, ondansetron)
Antibiotics (eg, ampicillin, gentamicin, trimethoprim-sulfamethoxazole, ciprofloxacin, levofloxacin,
ofloxacin)
Stone Prevention/Chemolysis
Uricosuric agents (eg, allopurinol)
Alkalinizing agents (eg, potassium citrate, sodium bicarbonate): For uric acid and cysteine calculi
Thiazide diuretics- helps treat hypercalcicuria
Surgical options
3. Stones that are 7 mm and larger are unlikely to pass spontaneously and require some type of
surgical procedure, such as the following:
Stent placement
Percutaneous nephrostomy
Extracorporeal shockwave lithotripsy (ESWL)
Ureteroscopy
Percutaneous nephrostolithotomy (PCNL) or mini PNCL
Open nephrostomy- more historical
Anatrophic nephrolithotomy- for large complex stag horn calculi that cannot be cleared by an
acceptable number of PCNLs. Typically now done via laparoscopic or robotic approach
Anatomy
Most of the pain receptors of the upper urinary tract responsible for the perception of renal colic are
located submucosally in the renal pelvis, calices, renal capsule, and upper ureter. Acute distention
seems to be more important in the development of the pain of acute renal colic than spasm, local
irritation, or ureteral hyperperistalsis.
Stimulation of the peripelvic renal capsule causes flank pain, while stimulation of the renal pelvis and
calices causes typical renal colic (see the image below). Mucosal irritation can be sensed in the renal
pelvis to some degree by chemoreceptors, but this irritation is thought to play only a minor role in the
perception of renal or ureteral colic.
Renal pain fibers are primarily preganglionic sympathetic nerves that reach spinal cord levels T-11
to L-2 through the dorsal nerve roots (see the images below). Aortorenal, celiac, and inferior
mesenteric ganglia are also involved. Spinal transmission of renal pain signals occurs primarily
through the ascending spinothalamic tracts.
In the lower ureter, pain signals are also distributed through the genitofemoral and ilioinguinal
nerves (see the image below). The nervi erigentes, which innervate the intramural ureter and
bladder, are responsible for some of the bladder symptoms that often accompany an intramural
ureteral calculus.
Pathophysiology
Formation of stones
Urinary tract stone disease is likely caused by two basic phenomena. The first phenomenon is
supersaturation of the urine by stone-forming constituents, including calcium, oxalate, and uric acid.
Crystals or foreign bodies can act as nidi, upon which ions from the supersaturated urine form
microscopic crystalline structures. The resulting calculi give rise to symptoms when they become
impacted within the ureter as they pass toward the urinary bladder.
The overwhelming majority of renal calculi contain calcium. Uric acid calculi and crystals of uric acid,
with or without other contaminating ions, comprise the bulk of the remaining minority. Other, less
frequent stone types include cystine, ammonium acid urate, xanthine, dihydroxyadenine, and various
rare stones related to precipitation of medications in the urinary tract. Supersaturation of the urine is
likely the underlying cause of uric and cystine stones, but calcium-based stones (especially calcium
oxalate stones) may have a more complex etiology.
The second phenomenon, which is most likely responsible for calcium oxalate stones, is deposition of
stone material on a renal papillary calcium phosphate nidus, typically a Randall plaque (which always
consists of calcium phosphate). Evan et al proposed this model based on evidence accumulating from
several laboratories. [5]
Calcium phosphate precipitates in the basement membrane of the thin loops of Henle, erodes into the
interstitium, and then accumulates in the subepithelial space of the renal papilla. The subepithelial
deposits, which have long been known as Randall plaques, eventually erode through the papillary
urothelium. Stone matrix, calcium phosphate, and calcium oxalate gradually deposit on the substrate to
create a urinary calculus.
Development of renal colic pain and renal damage
4. The colicky-type pain known as renal colic usually begins in the upper lateral midback over the
costovertebral angle and occasionally subcostally. It radiates inferiorly and anteriorly toward the groin.
The pain generated by renal colic is primarily caused by the dilation, stretching, and spasm caused by
the acute ureteral obstruction. (When a severe but chronic obstruction develops, as in some types of
cancer, it is usually painless.)
In the ureter, an increase in proximal peristalsis through activation of intrinsic ureteral pacemakers may
contribute to the perception of pain. Muscle spasm, increased proximal peristalsis, local inflammation,
irritation, and edema at the site of obstruction may contribute to the development of pain through
chemoreceptor activation and stretching of submucosal free nerve endings.
The term "renal colic" is actually a misnomer, because this pain tends to remain constant, whereas
intestinal or biliary colic is usually somewhat intermittent and often comes in waves. The pattern of the
pain depends on the individual’s pain threshold and perception and on the speed and degree of the
changes in hydrostatic pressure within the proximal ureter and renal pelvis. Ureteral peristalsis, stone
migration, and tilting or twisting of the stone with subsequent intermittent obstructions may cause
exacerbation or renewal of the renal colic pain.
The severity of the pain depends on the degree and site of the obstruction, not on the size of the stone.
A patient can often point to the site of maximum tenderness, which is likely to be the site of the ureteral
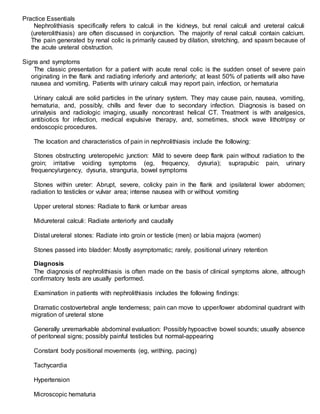
obstruction (see the image below).
Nephrolithiasis: acute renal colic. Distribution of renal and ureteral pain.
A stone moving down the ureter and causing only intermittent obstruction actually may be more painful
than a stone that is motionless. A constant obstruction, even if high grade, allows for various
autoregulatory mechanisms and reflexes, interstitial renal edema, and pyelolymphatic and pyelovenous
backflow to help diminish the renal pelvic hydrostatic pressure, which gradually helps reduce the pain.
The interstitial renal edema produced stretches the renal capsule, enlarges the kidney (ie,
nephromegaly), and increases renal lymphatic drainage. (Increased capillary permeability facilitates this
edema.) It may also reduce the radiographic density of the affected kidney’s parenchyma when viewed
on a noncontrast CT scan.
Distention of the renal pelvis initially stimulates ureteral hyperperistalsis, but this diminishes after 24
hours, as does renal blood flow. Peak hydrostatic renal pelvis pressure is attained within 2-5 hours after
a complete obstruction.
Within the first 90 minutes of a complete ureteral obstruction, afferent preglomerular arteriolar
vasodilation occurs, which temporarily increases renal blood flow. Between 90 minutes and 5 hours after
the obstruction, renal blood flow starts to decrease while intraureteral pressure continues to rise. By 5
hours after a complete obstruction, both renal blood flow and intraluminal ureteral pressure decrease on
the affected side.
Renal blood flow decreases to approximately 50% of normal baseline levels after 72 hours, to 30% after
1 week, to 20% after 2 weeks, and to 12% after 8 weeks. By this point, intraureteral pressures have
returned to normal, but the proximal ureteral dilation remains and ureteral peristalsis is minimal.
Interstitial edema of the affected kidney actually enhances fluid reabsorption, which helps to increase the
renal lymphatic drainage to establish a new, relatively stable, equilibrium. At the same time, renal blood
flow increases in the contralateral kidney as renal function decreases in the obstructed unit.
5. In summary, by 24 hours after a complete ureteral obstruction, the renal pelvic hydrostatic pressure has
dropped because of (1) a reduction in ureteral peristalsis; (2) decreased renal arterial vascular flow,
which causes a corresponding drop in urine production on the affected side; and (3) interstitial renal
edema, which leads to a marked increase in renal lymphatic drainage.
Additionally, as the ureter proximal to the stone distends, some urine can sometimes flow around the
obstruction, relieving the proximal hydrostatic pressure and establishing a stable, relatively painless
equilibrium. These factors explain why severe renal colic pain typically lasts less than 24 hours in the
absence of any infection or stone movement.
Whether calyceal stones cause pain continues to be controversial. In general, in the absence of
infection, how a renal stone causes pain remains unclear, unless the stone also causes obstruction.
Arguably, proving that a calyceal stone is causing an obstruction can be difficult. However, a stone
trapped in a calyx plausibly could block the outflow tract from that calyx, causing an obstruction and
subsequent pain.
Experimental studies in animals have suggested that renal damage may begin within 24 hours of a
complete obstruction and that permanent kidney deterioration starts within 5-14 days. Whereas some
practitioners wait several months for a stone to pass in an asymptomatic patient, others argue that
permanent damage is occurring as long as intervention is delayed.
Based on personal experience and anecdotal cases, the author recommends waiting no longer than 4
weeks for a stone to pass spontaneously before considering intervention. Convincing asymptomatic
patients of the need for surgical intervention may be difficult in the absence of a clear consensus in the
urological community about the length of time to wait before surgical stone removal, fragmentation, or
bypass.
If only a partial obstruction is present, the same changes occur, but to a lesser degree and over a longer
period. Proximal ureteric and renal pelvic hydrostatic pressures tend to remain elevated longer, and
ureteral peristalsis does not diminish as quickly. If the increased pressure is sufficient to establish a
reasonable flow beyond the obstructing stone, glomerular filtration and renal blood flow approximates
reference range baseline levels, although pain may be ongoing.
Etiology
A low fluid intake, with a subsequent low volume of urine production, produces high concentrations of
stone-forming solutes in the urine. This is an important, if not the most important, environmental factor in
kidney stone formation. The exact nature of the tubular damage or dysfunction that leads to stone
formation has not been characterized.
Most research on the etiology and prevention of urinary tract stone disease has been directed toward
the role of elevated urinary levels of calcium, oxalate, and uric acid in stone formation, as well as
reduced urinary citrate levels.
Hypercalciuria is the most common metabolic abnormality. Some cases of hypercalciuria are related to
increased intestinal absorption of calcium (associated with excess dietary calcium and/or overactive
calcium absorption mechanisms), some are related to excess resorption of calcium from bone (ie,
hyperparathyroidism), and some are related to an inability of the renal tubules to properly reclaim
calcium in the glomerular filtrate (renal-leak hypercalciuria).
Magnesium and especially citrate are important inhibitors of stone formation in the urinary tract.
Decreased levels of these in the urine predispose to stone formation.
The following are the four main chemical types of renal calculi, which together are associated with more
than 20 underlying etiologies:
Calcium stones
Struvite (magnesium ammonium phosphate) stones
Uric acid stones
Cystine stones
Stone analysis, together with serum and 24-hour urine metabolic evaluation, can identify an etiology in
more than 95% of patients. Specific therapy can result in a remission rate of more than 80% and can
decrease the individual recurrence rate by 90%. Therefore, emergency physicians should stress the
6. importance of urologic follow-up, especially in patients with recurrent stones, solitary kidneys, or
previous kidney or stone surgery and in all children. [6]
Calcium stones
Calcium stones account for 75% of renal calculi. Recent data suggest that a low-protein, low-salt diet
may be preferable to a low-calcium diet in hypercalciuric stone formers for preventing stone
recurrences. [7] Epidemiological studies have shown that the incidence of stone disease is inversely
related to the magnitude of dietary calcium intake in first-time stone formers.
There is a trend in the urology community not to restrict dietary intake of calcium in recurrent stone
formers. This is especially important for postmenopausal women in whom there is an increased concern
for the development of osteoporosis. Calcium oxalate, calcium phosphate, and calcium urate are
associated with the following disorders:
Hyperparathyroidism - Treated surgically or with orthophosphates if the patient is not a surgical
candidate
Increased gut absorption of calcium - The most common identifiable cause of hypercalciuria,
treated with calcium binders or thiazides plus potassium citrate
Renal calcium leak - Treated with thiazide diuretics
Renal phosphate leak - Treated with oral phosphate supplements
Hyperuricosuria - Treated with allopurinol, low purine diet, or alkalinizing agents such as potassium
citrate
Hyperoxaluria - Treated with dietary oxalate restriction, oxalate binders, vitamin B-6, or
orthophosphates
Hypocitraturia - Treated with potassium citrate
Hypomagnesuria - Treated with magnesium supplements
Struvite (magnesium ammonium phosphate) stones
Struvite stones account for 15% of renal calculi. They are associated with chronic urinary tract infection
(UTI) with gram-negative, urease-positive organisms that split urea into ammonia, which then combines
with phosphate and magnesium to crystalize into a calculus. Usual organisms include Proteus,
Pseudomonas, and Klebsiella species. Escherichia coli is not capable of splitting urea and, therefore, is
not associated with struvite stones. Because ammonia, a base, is produced during the catalytic process,
the urine pH is typically greater than 7.
Underlying anatomical abnormalities that predispose patients to recurrent kidney infections should be
sought and corrected. UTI does not resolve until stone is removed entirely.
Uric acid stones
Uric acid stones account for 6% of renal calculi. These are associated with urine pH less than 5.5, high
purine intake (eg, organ meats, legumes, fish, meat extracts, gravies), or malignancy (ie, rapid cell
turnover). Approximately 25% of patients with uric acid stone have gout.
Serum and 24-hour urine sample should be sent for creatinine and uric acid determination. If serum or
urinary uric acid is elevated, the patient may be treated with allopurinol 300 mg daily. Patients with
normal serum or urinary uric acid are best managed by alkali therapy alone.
Cystine stones
Cystine stones account for 2% of renal calculi. They arise because of an intrinsic metabolic defect
resulting in failure of renal tubular reabsorption of cystine, ornithine, lysine, and arginine. Urine becomes
supersaturated with cystine, with resultant crystal deposition.
Cystine stones are treated with a low-methionine diet (unpleasant), binders such as penicillamine or a-
mercaptopropionylglycine, large urinary volumes, or alkalinizing agents. A 24-hour quantitative urinary
cystine determination helps to titrate the dose of drug therapy to achieve a urinary cystine concentration
of less than 300 mg/L.
7. Drug-induced stone disease
A number of medications or their metabolites can precipitate in urine causing stone formation. These
include the following
Indinavir
Atazanavir
Guaifenesin
Triamterene
Silicate (overuse of antacids containing magnesium silicate)
Sulfa drugs, including sulfasalazine, sulfadiazine, acetylsulfamethoxazole, acetylsulfasoxazole, and
acetylsulfaguanidine
Ceftriaxone (rarely)
A population-based case-control study from the United Kingdom found that use of any of the following
five oral antibiotic classes 3–12 months before the index date was associated with nephrolithiasis:
Sulfas - Adjusted odds ratio (OR) 2.33 (95% confidence interval [CI] 2.19-2.48)
Cephalosporins – OR 1.88 (95% CI 1.75-2.01)
Fluoroquinolones – OR 1.67 (95% CI 1.54-1.81)
Nitrofurantoin/methenamine – OR 1.70 (95% CI 1.55-1.88)
Broad-spectrum penicillins – OR 1.27 (9% CI 1.18-1.36)
Associations were greatest for exposure at younger ages (P< 0.001) and exposure 3–6 months before
the index date (P< 0.001). With all but broad-spectrum penicillins, the risk remained statistically
significant 3–5 years from exposure.
Genetic factors
Nephrolithiasis is known to have a familial nature and significant heritability, and genes that may be
involved in renal stone formation have been identified. Genome-wide association studies and candidate
gene studies have implicated genes involved in renal tubular handling of lithogenic substrates, such as
calcium, oxalate, and phosphate, and of inhibitors of crystallization, such as citrate and magnesium.
Prognosis
Approximately 80-85% of stones pass spontaneously. Approximately 20% of patients require hospital
admission because of unrelenting pain, inability to retain enteral fluids, proximal UTI, or inability to pass
the stone.
The most morbid and potentially dangerous aspect of stone disease is the combination of urinary tract
obstruction and upper urinary tract infection. Pyelonephritis, pyonephrosis, and urosepsis can ensue.
Early recognition and immediate surgical drainage are necessary in these situations.
Because the minimally invasive modalities for stone removal are generally successful in removing
calculi, the primary consideration in managing stones is not whether the stone can be removed but
whether it can be removed in an uncomplicated manner with minimum morbidity.
The usually quoted recurrence rate for urinary calculi is 50% within 5 years and 70% or higher within 10
years, although a large, prospective study published in 1999 suggested that the recurrence rate may be
somewhat lower at 25-30% over a 7.5-year period. Recurrence rates after an initial episode of
ureterolithiasis have also been reported to be 14%, 35%, and 52% at 1, 5, and 10 years, respectively.
Metabolic evaluation and treatment are indicated for patients at greater risk for recurrence, including
those who present with multiple stones, who have a personal or family history of previous stone
formation, who present with stones at a younger age, or who have residual stones after treatment.
Medical therapy is generally effective at delaying (but perhaps not completely stopping) the tendency for
stone formation. The most important aspect of medical therapy is maintaining a high fluid intake and
subsequent high urinary volume. Without an adequate urinary volume, no amount of medical or dietary
therapy is likely to be successful in preventing stone formation.
According to estimates, merely increasing fluid intake and regularly visiting a physician who advises
increased fluids and dietary moderation can cut the stone recurrence rate by 60%. This phenomenon is
known as the “stone clinic” effect. In contrast, optimal use of metabolic testing with proper evaluation
8. and compliance with therapy can completely eliminate new stones in many patients and significantly
reduces new stone formation in most patients.
Endogenous sources
ROS are produced during a variety of biochemical reactions within the cell and within organelles
such as mitochondria, peroxisomes, and endoplasmic reticulum. Mitochondria convert energy for
the cell into a usable form, adenosine triphosphate (ATP). The process of ATP production in the
mitochondria, called oxidative phosphorylation, involves the transport of protons (hydrogen ions)
across the inner mitochondrial membrane by means of the electron transport chain. In the electron
transport chain, electrons are passed through a series of proteins via oxidation-reduction reactions,
with each acceptor protein along the chain having a greater reduction potential than the previous.
The last destination for an electron along this chain is an oxygen molecule. In normal conditions, the
oxygen is reduced to produce water; however, in about 0.1–2% of electrons passing through the
chain (this number derives from studies in isolated mitochondria, though the exact rate in live
organisms is yet to be fully agreed upon), oxygen is instead prematurely and incompletely reduced
to give the superoxide radical (•O−
2), most well documented for Complex I and Complex III.
Another source of ROS production is the electron transfer reactions catalyzed by the mitochondrial
P450 systems in steroidogenic tissues.[10] These P450 systems are dependent on the transfer of
electrons from NADPH to P450. During this process, some electrons "leak" and react with O2
producing superoxide. To cope with this natural source of ROS, the steroidogenic tissues, ovary and
testsis, have a large concentration of antioxidants such as vitamin C (ascorbate) and β-carotene and
anti-oxidant enzymes.
If too much damage is present in mitochondria, a cell undergoes apoptosis or programmed cell
death.
ROS are produced in immune cell signaling via the NOX pathway. Phagocytic cells such as
neutrophils, eosinophils, and mononuclear phagocytes produce ROS when stimulated.
Exogenous sources
The formation of ROS can be stimulated by a variety of agents such as pollutants, heavy metals,[2]
tobacco, smoke, drugs, xenobiotics, or radiation.
Ionizing radiation can generate damaging intermediates through the interaction with water, a
process termed radiolysis. Since water comprises 55–60% of the human body, the probability of
radiolysis is quite high under the presence of ionizing radiation. In the process, water loses an
electron and becomes highly reactive. Then through a three-step chain reaction, water is
sequentially converted to hydroxyl radical (•OH), hydrogen peroxide (H2O2), superoxide radical (•O−
2), and ultimately oxygen (O2).
The hydroxyl radical is extremely reactive and immediately removes electrons from any molecule
in its path, turning that molecule into a free radical and thus propagating a chain reaction. However,
hydrogen peroxide is actually more damaging to DNA than the hydroxyl radical, since the lower
reactivity of hydrogen peroxide provides enough time for the molecule to travel into the nucleus of
the cell, subsequently reacting with macromolecules such as DNA.
According to the free radical theory of aging, oxidative damage initiated by reactive oxygen species
is a major contributor to the functional decline that is characteristic of aging. While studies in
invertebrate models indicate that animals genetically engineered to lack specific antioxidant
enzymes (such as SOD), in general, show a shortened lifespan (as one would expect from the
theory), the converse manipulation, increasing the levels of antioxidant enzymes, has yielded
inconsistent effects on lifespan (though some studies in Drosophila do show that lifespan can be
9. increased by the overexpression of MnSOD or glutathione biosynthesizing enzymes). Also contrary
to this theory, deletion of mitochondrial SOD2 can extend lifespan in Caenorhabditis elegans.
In mice, the story is somewhat similar. Deleting antioxidant enzymes, in general, yields shorter
lifespan, though overexpression studies have not (with some recent exceptions) consistently
extended lifespan.[28] Study of a rat model of premature aging found increased oxidative stress,
reduced antioxidant enzyme activity and substantially greater DNA damage in the brain neocortex
and hippocampus of the prematurely aged rats than in normally aging control rats.[29] The DNA
damage 8-OHdG is a product of ROS interaction with DNA. Numerous studies have shown that 8-
OHdG increases in different mammalian organs with age.
Renal Health Plus
Kidney diseases, especially End Stage Renal Disease (ESRD), are already the 7 th leading cause of death
among the Filipinos. One Filipino develops chronic renal failure every hour or about 120 Filipinos per
million population per year. More than 5,000 Filipino patients are presently undergoing dialysis and
approximately 1.1 million people worldwide are on renal replacement therapy. Reliable estimates reveal
that the number of these patients will double in 2010.
In the past, chronic glomerulonephritis was the most common cause of chronic renal failure. Today,
diabetes mellitus and hypertension have taken center stage in the causation of ESRD which together
account for almost 60% of dialysis patients.
The cost of medical treatment for kidney diseaseis really exorbitant, beyond the reach of ordinary patients.
Renal transplantation is limited due to the expense and the shortage of donors. The best that can be done
at present is to focus efforts on the prevention of progression of renal diseases. Strict blood pressure and
glycemic control and adoption of “ healthy lifestyle” play a major role in reducing if not totally controlling
the epidemic of renal failure and this could be achieved through proper education.
This Renal Health Plus provides educational information related to the prevention, diagnosis and treatment
of kidney diseases.
The Human Kidneys
Kidneys are important parts of the urinary system. They are found at each side of the spine, below
the rib cage of the human body. Each kidney is as big as a fist, weighs ¼ pound and looks like a
kidney bean.
The kidneys perform vital life-maintaining functions as monitors and regulators of body fluid. They
excrete fluids when the body has an excess of them and retain the substances necessary for the
body’s continuing function. They produce and release a variety of chemicals to keep the body
healthy and filter the entire blood supply every 2 minutes, excreting waste materials through the
urine.
The kidneys also produce erythropoietin, a hormone that controls the production of red blood cells
by the bone marrow.
They also are involved in the regulation of blood pressure. This probably happens through the
regulation of blood volume and the amount of sodium in the body as well as the production of
substances such as the angiotensin.
10. General Ways of Protecting your Kidneys
Exercise regularly
Eat healthy diet
Maintain ideal body weight
Avoid smoking
Avoid taking medications or herbal supplements without advice of physician
Consult doctor right away if with symptoms
Drink lots of water and avoid excessive salt
Have annual physical check-up especially if with or with family history of hypertension, diabetes or
renal failure
If hypertensive and diabetic,
Take medications regularly
See the doctor regularly
Know blood sugar and blood pressure goals and make sure targets are met
Make sure the doctor checks the kidneys regularly
Diagnostic Service
Diagnosis of kidney ailments and kidney related health diseases is pivotal in providing effective
therapeutic plan. The National and Kidney and Transplant Institute offers a wide range of the latest
and state of the art diagnostic tools to quickly and accurately diagnose kidney diseases.
Question:
What are the signs and symptoms of kidney disorder?
Answer:
The main symptom of kidney disorder is fluid retention or edema. Patients may have puffiness
around the eyes, swelling in the feet and legs and water in the lungs leading to difficulty of breathing
Any change in urination may also indicate kidney problem. This may consist of pain or unusual
sensation during voiding, increased or decreased frequency of urination, difficulty in initiating
urination, frequent urination at night, change in color of urine, blood in the urine or bubbly
appearance of the urine.
Kidney failure results in the retention of various body wastes which cause anorexia, vomiting,
difficulty in sleeping and generalized body weakness. This is often evaluated by measuring serum
creatinine and blood urea nitrogen.
The presence of protein and red blood cells in the urine is also an indication of kidney disorder. In
glomerulonephritis, proteinuria and hematuria are commonly seen because the glomeruli have
become inflamed. Proteinuria is also the earliest manifestation of diabetic nephropathy. Pallor and
weakness are also among the indications of kidney failure due to anemia secondary to low
erythropoietin production by the failing kidneys.
11. Hypertension is also a major consequence of kidney disorder. Initial evaluation of all newly
diagnosed hypertensive patients should include serum creatinine and electrolyte levels (sodium and
potassium) particularly among young hypertensive subgroup.
Repeated urinary tract infections, back pain or pain in the lower abdomen may indicate the
presence of kidney stones and may also cause blood in the urine.
Question:
What diseases commonly affect the kidneys?
Answer:
Infection is the most common disorder of the kidneys and the urinary tract. Uncomplicated urinary
tract infections are very easy to treat
Stones are solid residues in the urinary tract that may cause obstruction to the flow of urine which
in turn may lead to infection of the kidneys and subsequent scarring.
Glomerulonephritis is inflammation of the glomeruli, the small vessels in the nephron. If not treated,
patients may suffer slow progressive damage to the kidneys and develop renal failure.
Hypertension occurs with many cases of kidney diseases. Prolonged hypertension damages the
small arteries in the kidneys. This may start a vicious cycle: damaged kidneys cause more serious
hypertension which in turn brings more damage to the kidneys.
Diabetes may also damage the kidneys. It is the leading cause of chronic renal failure in many
countries.
Abnormalities in the urinary tract that are congenital or inborn may consequently lead to poor
function, obstruction or infection of the kidneys.
Some drugs, herbal medicine, solvents and insectides can also harm the kidneys.
Question:
What are the warning signs of kidney disease?
Answer:
Puffiness of the eye area
Progressive swelling of parts of the body usually at the ankles
Back pain on the lower part just below the ribcage
Changes in urination (increased or decreased frequency of urination, frequent urination at night,
pain or unusually sensation during voiding, hesitancy or difficulty in initiating urination, change in
color of the urine, blood in the urine)
New onset of high blood pressure
Question:
What are the symptoms of Urinary Tract Infection (UTI)?
Answer:
Not everyone with UTI has symptoms, but most people get at least some. These may include a
frequent urge to urinate and a painful, burning feeling in the area of the bladder or urethra during
urination. It is not unusual to feel bad and to feel pain even when not urinating. Often women feel an
uncomfortable pressure above the pubic bone and some men experience fullness in the rectum. It
12. is common for a person with UTI to complain that despite the urge to urinate, only a small amount
of urine is passed.
The urine itself may look milky or cloudy, even reddish if blood is present. A fever may mean that
the infection has reached the kidneys. Other symptoms of a kidney infection include pain in the back
or side below the ribs, nausea or vomiting.
Question:
How can UTI be prevented?
Answer:
There is no proven way to prevent UTI, but the following suggestions maybe helpful:
Drink plenty of liquids about 6-8 glasses/day to flush bacteria out of the urinary system,
Schedule frequent bathroom breaks
Women should drink water before and after sex so they will urinate a good volume with a steady
stream afterward. This will help eliminate any bacteria that may have entered the urinary bladder.
After defecating, women should not wipe in the direction of the vagina to avoid spreading bacteria
from the gastrointestinal tract
Question:
How should patients with hypertension be treated?
Answer:
Treatment of hypertension can be achieved through non-pharmacologic and pharmacologic
means. It consists of the following
Lifestyle modification
Weight loss
Exercise
Low salt, low fat diet
Stop smoking
Less alcohol consumption
Cope with stress
Regular intake of antihypertensive medications
Question:
How are kidney stones prevented from developing?
Answer:
The simplest and most important lifestyle change to prevent all kinds of kidney stones from
developing is to drink more liquids. Water is the best. It is recommended that water intake should be
at least 2 liters per day. There are many proponents of various “cures” by drinking other liquids such
13. as buko juice, pito-pito tea, sambong tea and many other teas but scientific studies have not proven
their efficacy and safety.
Therapeutic Options
Treatment of kidney diseases may involve the following: medical therapy such as medicines and
dietary changes, dialysis and transplantation
Because kidney failure is already irreversible at later stages, treatment focuses on controlling the
symptoms, minimizing complications and slowing the progression of the disease.
Associated diseases that cause or result from chronic renal failure must be controlled.
Hypertension, diabetes, congestive heart failure, UTI, kidney stones, obstructions of the urinary tract,
glomerulonephritis, and other disorders should be treated appropriately.
Medications such as iron supplements and erythropoietin injections may be needed to control
anemia. Blood transfusion may be given but they are less preferred.
Fluid intake may be restricted, often to an amount equal to the volume of urine produced. Dietary
protein restriction may slow the build-up of wastes in the bloodstream and control associated
symptoms such as nausea and vomiting. Salt, potassium, phosphorus and other electrolytes may
be restricted.
Dialysis and kidney transplantation may be required eventually when end stage renal disease
ensues or when 85-90 percent of kidney function is lost.
Hemodialysis uses a special filter called a dialyzer that functions as an artificial kidney to clean the
blood. During treatment, blood travels through the tubes into the dialyzer which filters out wastes
and extra water. Then the cleaned blood flows through another set of tubes back into the body. The
dialyzer is connected to the machine that monitors blood flow and removes wastes from the blood.
Hemodialysis is usually performed 2 to 3 times a week. Each treatment last for 4 hours.
Peritoneal dialysis is another procedure that removes extra water and wastes from the body. This
type of dialysis uses the lining of the abdomen to filter the blood. This lining is called the peritoneal
membrane and acts as the artificial kidney. A mixture of minerals and sugar dissolved in water called
dialysis solution travels through a soft tube into the abdomen. The sugar, called dextrose, draws
wastes, chemical and extra water from the tiny blood vessels in the peritoneal membrane into the
dialysis solution. After several hours, the used solution is drained from the abdomen through the
tube, taking the wastes from the blood with it. Then the patient fills his abdomen with fresh dialysis
solution and the cycle is repeated usually 3 to 4 times a day. Each cycle is called an exchange.
Kidney transplantation surgically places a healthy kidney from another person into the body of the
patient with end stage renal disease. The donated kidney does the work that the 2 failed kidneys
used to do. It is generally not necessary to remove the diseased kidneys. A donated kidney may
come from an anonymous donor who has recently died or from a living person usually relative. The
kidney that the patient receives must be a good match for his body. The more the new kidney is like
his own, the less likely will his immune system reject it. The patient will be made to take special
drugs called immunosuppressives to help trick his immune system so it would not reject the
transplanted kidney.