2. Functions of the liver
• The liver regulates most chemical levels in the blood and
excretes a product called bile.
• This helps carry away waste products from the liver. All the
blood leaving the stomach and intestines passes through the
liver.
• The liver processes this blood and breaks down, balances, and
creates the nutrients and also metabolises drugs into forms that
are easier to use for the rest of the body or that are nontoxic.
• More than 500 vital functions have been identified with the
liver.
3. Some of the more well-known functions include the following:
• Production of bile, which helps carry away waste and break down
fats in the small intestine during digestion
• Production of certain proteins for blood plasma
• Production of cholesterol and special proteins to help carry fats
through the body
• Conversion of excess glucose into glycogen for storage (glycogen can
later be converted back to glucose for energy) and to balance and
make glucose as needed.
• Regulation of blood levels of amino acids, which form the building
blocks of proteins
• Processing of haemoglobin for use of its iron content (the liver stores
iron)
4. • Conversion of poisonous ammonia to urea (urea is an end product
of protein metabolism and is excreted in the urine)
• Clearing the blood of drugs and other poisonous substances
• Regulating blood clotting
• Resisting infections by making immune factors and removing
bacteria from the bloodstream
• Clearance of bilirubin, also from red blood cells. If there is an
accumulation of bilirubin, the skin and eyes turn yellow.
When the liver has broken down harmful substances, its by-products
are excreted into the bile or blood. Bile by-products enter the intestine
and leave the body in the form of feces. Blood by-products are filtered
out by the kidneys, and leave the body in the form of urine.
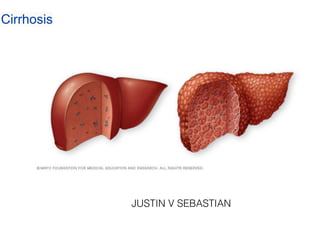
5. Introductio
n
• Cirrhosis occurs in response to damage to
liver. Each time liver is injured, it tries to
repair itself. In the process, scar tissue forms.
As cirrhosis progresses, more and more scar
tissue forms, making it dif
fi
cult for the liver
to function.
6. Defi
nition
• Cirrhosis is a chronic disease characterized by
replacement of normal liver tissue with diffuse
fi
brosis that disrupts the structure and function of
the liver. (Brunner)
• Cirrhosis is de
fi
ned as the presence of large
amounts of scar tissue in the liver due to many
years of liver in
fl
ammation and injury.
(Mayo Clinic)
7. Type
s
There are three types of cirrhosis or scarring of the liver:
Alcoholic cirrhosis, in which the scar tissue characteristically
surrounds the portal areas. This is most frequently due to
chronic alcoholism and is the most common type of cirrhosis.
Post-necrotic cirrhosis, in which there are broad bands of scar
tissue as a late result of a previous bout of acute viral hepatitis.
Biliary cirrhosis, in which scarring occurs in the liver around
the bile ducts. This type usually is the result of chronic biliary
obstruction and infection (cholangitis); it is much less common
than the other two types.
8. Cause
s
•
Chronic alcohol abus
e
•
Chronic viral hepatitis (hepatitis B and C
)
•
Fat accumulating in the liver (nonalcoholic fatty liver disease
)
Other possible causes include
:
•
Iron buildup in the body (hemochrombtosis
)
•
Cystic
fi
brosi
s
•
Copper accumulated in the liver (Wilson's disease
)
•
Poorly formed bile ducts (biliary atresia
)
•
Genetic digestive disorder (Alagille syndrome
)
•
Liver disease caused by body's immune system (autoimmune hepatitis
)
•
Destruction of the bile ducts (primary biliary cirrhosis
)
•
Hardening and scarring of the bile ducts (primary sclerosing cholangitis
)
•
Infection such schistosomiasi
s
•
Medications
9.
10. Symptom
s
Cirrhosis often has no signs or symptoms until liver damage is
extensive. When signs and symptoms do occur, they may include
:
•
Fatigu
e
•
Bleeding easil
y
•
Bruising easil
y
•
Itchy ski
n
•
Yellow discoloration in the skin and eyes (jaundice
)
•
Fluid accumulation in abdomen (ascites
)
•
Loss of appetit
e
•
Nausea
11. •
Swelling in leg
s
•
Weight los
s
•
Confusion, drowsiness and
s l u r r e d s p e e c h ( h e p a t i c
encephalopathy
)
•
Spider-like blood vessels on ski
n
•
Redness in the palms of the
hand
s
•
Testicular atrophy in me
n
•
Breast enlargement in men
12. Complication
s
Complications of cirrhosis can include
:
Complications related to blood
fl
ow
:
•
High blood pressure in the veins that supply the liver (portal
hypertension). Cirrhosis slows the normal
fl
ow of blood through
the liver, thus increasing pressure in the vein that brings blood
from the intestines and spleen to the liver
.
•
Swelling in the legs and abdomen. Portal hypertension can cause
fl
uid to accumulate in the legs (edema) and in the abdomen
(ascites). Edema and ascites also may result from the inability of
the liver to make enough of certain blood proteins, such as
albumin.
13. •
E n l a r g e m e n t o f t h e s p l e e n
(splenomegaly). Portal hypertension
can also cause changes to the spleen
.
•
Bleeding. Portal hypertension can
cause blood to be redirected to smaller
veins, causing them to increase in size
and become varices. Strained by the
extra load, these smaller veins can
burst, causing serious bleeding. If the
liver can't make enough clotting
factors, this also can contribute to
continued bleeding.
14. Other complications
:
•
Infections. If there cirrhosis, body may have
dif
fi
culty
fi
ghting infections. Ascites can lead to
spontaneous bacterial peritonitis, a serious
infection
.
•
Malnutrition. Cirrhosis may make it more
dif
fi
cult for body to process nutrients, leading to
weakness and weight loss
.
•
Buildup of toxins in the brain (hepatic
encephalopathy). A liver damaged by cirrhosis
isn't able to clear toxins from the blood as well
as a healthy liver can. These toxins can then
build up in the brain and cause mental confusion
and dif
fi
culty concentrating.
15. •
Jaundice. Jaundice occurs when the diseased liver
doesn't remove enough bilirubin, a blood waste
product, from blood. Jaundice causes yellowing of the
skin and whites of the eyes and darkening of urine
.
•
Increased risk of liver cancer. A large proportion of
people who develop liver cancer that forms within the
liver itself have cirrhosis
.
•
Acute-or-chronic liver failure. Some people end up
experiencing multi organ failure.
16. Diagnosis
Liver function.
• Blood is checked for excess bilirubin, which is a product of red blood cells
breaking down.
• Aspartate aminotransferase (AST), alanine aminotransferase (ALT), and
lactate dehydrogenase (LDH). An increased level of these enzymes may
mean injury to the liver and the death of liver cells.
• Alkaline phosphatase (ALP). An increased ALP level may mean blockage of
bile ducts
.
Kidney function. Blood is checked for creatinine as kidney function may
decline in later stages of cirrhosis (decompensated cirrhosis)
.
Tests for hepatitis B and C. Blood is checked for the hepatitis viruses
.
Clotting. International normalized ratio (INR) is checked for blood's ability to
clot.
17. Doctor may order imaging and other tests to further diagnose
cirrhosis:
•
Magnetic resonance elastography or transient
elastography. These noninvasive imaging tests detect
hardening or stiffening of the liver and may eliminate the need
for a liver biopsy
.
•
Other imaging tests. MRI, CT and ultrasound create images
of the liver
.
•
Biopsy. A tissue sample (biopsy) is not necessarily needed to
diagnose cirrhosis. However, doctor may use it to identify the
severity, extent and cause of liver damage.
18. Treatment for the underlying cause of cirrhosi
s
In early cirrhosis, it may be possible to minimize damage to the liver by treating the
underlying cause. The options include
:
•
Treatment for alcohol dependency. People with cirrhosis caused by alcohol
abuse should stop drinking
.
•
Weight loss. People with cirrhosis caused by nonalcoholic fatty liver disease may
become healthier if they lose weight
.
•
Medications to control hepatitis. Medications may limit further damage to liver
cells caused by hepatitis B or C through speci
fi
c treatment of these viruses
.
•
Medications to control other causes and symptoms of cirrhosis. Medications
may slow the progression of certain types of liver cirrhosis. For example, for
people with primary biliary cirrhosis (now known as primary biliary cholangitis)
that is diagnosed early, medication may signi
fi
cantly delay progression to
cirrhosis.
19. Treatment for complications of cirrhosi
s
•
Excess
fl
uid in body. A low-sodium diet and medication to prevent
fl
uid
buildup in the body may help control ascites and swelling. At times, a small
tube — a transjugular intrahepatic portosystemic shunt (TIPS) — is placed in
the vein within the liver to reduce blood pressure in liver and slow the rate of
fl
uid accumulation
.
•
Portal hypertension. Certain blood pressure medications may control
increased pressure in the veins that supply the liver (portal hypertension) and
prevent severe bleeding. In severe cases, a TIPS can be placed in the vein
within the liver to reduce blood pressure in liver and to prevent further
bleeding
.
•
Infections. Patient may receive antibiotics or other treatments for infections
.
•
Increased liver cancer risk. Doctor will recommend blood tests and
ultrasound exams every six months to look for signs of liver cancer.
20.
21. Liver transplantatio
n
In advanced cases of cirrhosis, when the liver ceases to
function, a liver transplant may be the only treatment
option. People usually need to consider this option when
they develop symptoms from cirrhosis, such as jaundice,
signi
fi
cant
fl
uid retention (ascites), bleeding varices,
hepatic encephalopathy, kidney dysfunction, or liver
cancer. A liver transplant replaces liver with a healthy liver
from a deceased donor or with part of a liver from a living
donor.
22. Nursing diagnosi
s
1
Imbalanced Nutrition: Less Than Body Requirement
s
2
Excess Fluid Volum
e
3
Risk for Impaired Skin Integrit
y
4
Ineffective Breathing Patter
n
5
Risk for Injur
y
6
Risk for Acute Confusio
n
7
Disturbed Body Imag
e
8
De
fi
cient Knowledge
24. • Few cancers originate in the liver.
• Primary tumors ordinarily occur in patients with chronic
liver disease (cirrhosis)
• Hepatocellular carcinoma (HCC), the most common
type of primary liver tumor, usually cannot be resected
because of rapid and metastasis elsewhere.
• Other types include cholangiocellular carcinoma
(CCC) and combined HCC and CCC.
• If found early resection may be possible: however, early
detection is rare.
25. Etiology
• Cirrhosis, hepatitis B and C, and exposure to
certain chemical toxins have been implicated in
the etiology of HCC.
• Cigarette smoking, especially when combined
with alcohol use, has also been identified as a risk
factor.
• Half of all advanced liver cancer cases represent
metastases from other primary sites.
27. Clinical manifestations
• Early manifestations include pain ( dull ache in
upper right quadrant, epigastrium, or back), recent
weight loss, loss of strength, anorexia and anemia.
• Liver enlargement and irregular surface may be
noted on palpation
• Jaundice is present only if larger bile duct are
occluded.
• Ascites occurs if portal veins are obstructed.
28. Diagnosis
• History collection and physical
examination.
• Tumor marker identification: it includes
alfa fetoprotein (AFP), carcinoembryonic
antigen ( CEA)
30. Treatment
Surgical management
• Hepatic lobectomy: can be performed when the primary
hepatic tumor is localized or when the primary site can
be completely excised and the metastasis is limited.
• Capitalising on the regenerative capacity of the liver
cells, 90% of the liver has been removed.
• The presence of cirrhosis limits the ability of the liver
to regenerate.
31. • Liver transplantation: removal of the liver
and replacement with a healthy donor has
been successful, but recurrence rate of
primary liver malignancy after
transplantation is 75-85%.
32. Percutaneous biliary drainage
• Percutaneous biliary drainage is used to bypass
biliary ducts obstructed by the liver, pancreatic,
or bile ducts tumours in patients with inoperable
tumors or those who are surgical risk.
• Complications include sepsis, leakage of bile,
haemorrhage, and reobstruction of the biliary
system.
33.
34. • Radiation therapy
Radiation therapy uses high-powered beams of
energy, such as X-rays and protons, to kill cancer
cells.
• Chemotherapy
Chemotherapy uses drugs to destroy cancer cells,
doctor may recommend chemotherapy to decrease
the chance that the cancer will recur.
38. Causes of portal hypertensio
n
Pre hepati
c
• Congenital portal atresi
a
• Portal vein thrombosi
s
• Phlebitis of portal vei
n
Hepati
c
• Cirrhosi
s
• Chronic hepatiti
s
• Parasitic infections (schistosomiasis
)
Post hepati
c
• Budd-chiari syndrom ( Hepatic venus thrombosis
)
• Constructive pericarditi
s
• Tricuspid valve incompetence
40. Symptoms
Symptoms of portal hypertension include the following:
•
Weakness, tiredness, and malaise
•
Anorexia
•
Sudden and massive bleeding, with or without shock on
presentation
•
Nausea and vomiting
•
Weight loss
•
Abdominal discomfort and pain - Usually felt in the right
hypochondrium or under the right lower ribs (front, side, or back)
and in the epigastrium or the left hypochondrium
•
Jaundice
•
Edema and abdominal swelling
41. •
Pruritus
•
Spontaneous bleeding and easy bruising
•
Symptoms of encephalopathy
•
Impotence and sexual dysfunction
•
Hematemesis or melena - May indicate gastroesophageal
variceal bleeding
•
Increasing abdominal girth - May indicate ascites
formation
•
Abdominal pain and fever - May indicate spontaneous
bacterial peritonitis
•
Hematochezia
44. Medical Management
DIETARY MODIFICATION
The goal of treatment for the patient with ascites is
a negative sodium balance to reduce fluid
retention.
DIURETICS
Use of diuretics along with sodium restriction is
successful in 90% of patients with ascites.
PARACENTESIS
Paracentesis is the removal of fluid (ascites) from
the peritoneal cavity through a small surgical
incision or puncture made through the abdominal
wall under sterile conditions.
45. Beta-blockers
Beta-blockers (nadolol or propranolol) may be prescribed to reduce
the pressure in varices and further reduce the risk of bleeding.
BALLOON TAMPONADE
To control haemorrhage in certain patients, balloon tamponade
may be used. In this procedure, pressure is exerted on the cardia
(upper orifice of the stomach) and against the bleeding varices by a
balloon tamponade. The tube has four openings, each with a
specific purpose: gastric aspiration, esophageal aspiration, inflation
of the gastric balloon, and inflation of the esophageal balloon.
46.
47. ENDOSCOPIC SCLEROTHERAPY
In endoscopic sclerotherapy (also referred to as injection sclerotherapy),
a sclerosing agent is injected through a fiberoptic endoscope into the
bleeding esophageal varices to promote thrombosis and eventual sclerosis.
48. ESOPHAGEAL BANDING THERAPY (VARICEAL BAND LIGATION)
In variceal banding, a modi
fi
ed endoscope loaded with an elastic rubber band
is passed through an over-tube directly onto the varix (or varices) to be
banded. After suctioning the bleeding varix into the tip of the endoscope, the
rubber band is slipped over the tissue, causing necrosis, ulceration, and
eventual sloughing of the varix.
49. TRANSJUGULAR INTRAHEPATIC PORTOSYSTEMIC SHUNTING
Transjugular intrahepatic portosystemic shunting (TIPS) is a method of
treating esophageal varices in which a cannula is threaded into the portal
vein by the transjugular route. An expandable stent is inserted and serves
as an intrahepatic shunt between the portal circulation and the hepatic
vein, reducing portal hypertension.
50. SURGICAL MANAGEMENT
Several surgical procedures have
been developed to treat esophageal
varices and to minimise rebleeding,
but they are often accompanied by
signi
fi
cant risk. Procedures that may
be used for esophageal varices are;
splenorenal and portacaval venous
shunts to relieve portal pressure.