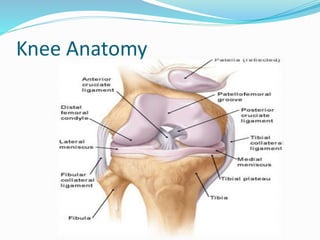
The document discusses rehabilitation after ACL reconstruction surgery. It begins with an introduction noting that ACL tears are a common sports injury. It then covers knee anatomy, the anatomy and biomechanics of the ACL, surgical treatment, and post-operative rehabilitation phases and techniques. The rehabilitation process involves regaining range of motion and quadriceps strength in early phases, advancing to sport-specific drills, with a focus on gradually increasing loads on the knee through strengthening and proprioceptive exercises.



![References
1. Brown CH Jr, Carson EW: Revision anterior cruciate ligament surgery.
Clin Sports Med 18:109-171, 1999
2.Reiman PR, Jackson DW: Anatomy of the anterior cruciate ligament, in
Jackson DW, DrezD (eds): The Anterior Cruciate Deficient Knee. St.Louis, CV Mosby & Co, 1987, pp 17-26
3.Dienst M, Burks RT, Greis PE: Anatomy and biomechanics of the anteriorcruciate ligament. Orthop Clin North Am
33:605-620, 2002
4.Cross.MJ.Anterior Cruciate Ligament injuries :Treatment and Rehabilitation. Sydney, Australia :North Sydney
Orthopedic and Sports Medicine Center.
5.Bradley JB , Klimkiewicz JJ , rytel MJ , Powell JW Anterior Cruciate Ligament Injuries In The National Football League
6.Root ML , Weed JH , Sgarlato TE , et al : Axis of Motion Of The Subtalar Joint . J Am Podiatr Med Assoc 56:149-155 , 1966.
7. Shelbourne KD, Wilckens JH, Mollabashy A, DeCarlo M. Arthrofibrosis in acute anterior cruciate ligament
reconstruction. The effect of timing of reconstruction and rehabilitation. Am J Sports Med. 1991;19:332–336. [PubMed]
8. Chmielewski TL, Stackhouse S, Axe MJ, Snyder-Mackler L. A prospective analysis of incidence and severity of quadriceps
inhibition in a consecutive sample of 100 patients with complete acute anterior cruciate ligament rupture. J Orthop
Res. 2004;22:925–930. [PubMed]](https://image.slidesharecdn.com/aclppt-141218113153-conversion-gate02/85/Acl-ppt-30-320.jpg)