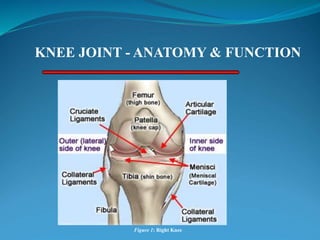
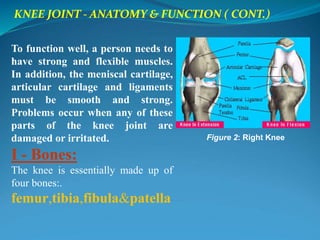
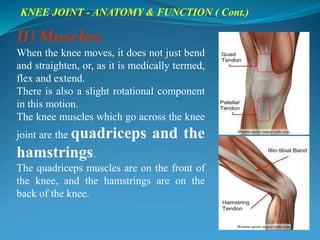
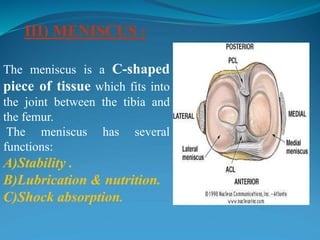
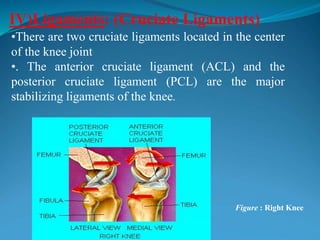
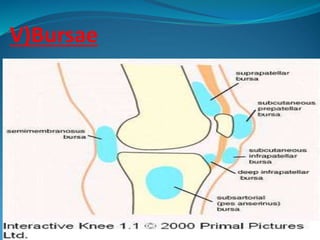
1. The document discusses the anatomy and function of the knee joint, including the bones, muscles, meniscus, ligaments, and bursae that make up the knee.
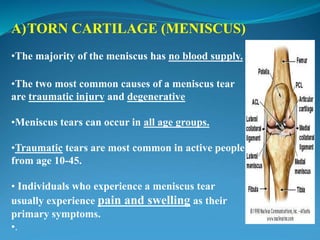
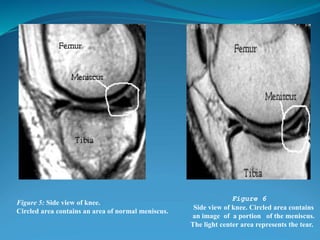
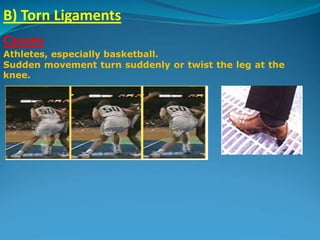
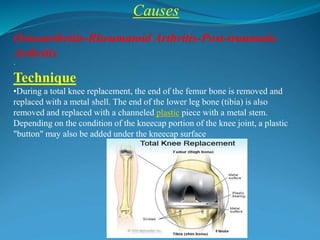
2. Common knee injuries are described such as torn cartilage (meniscus), ligament tears, arthritis, bursitis, and bone tumors.
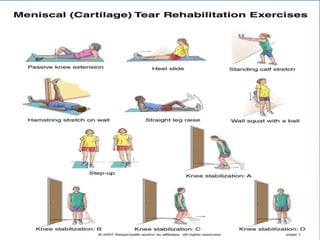
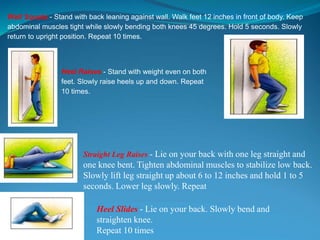
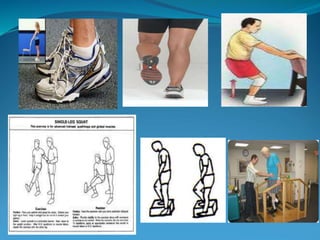
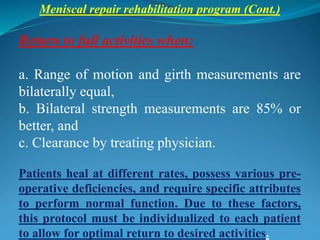
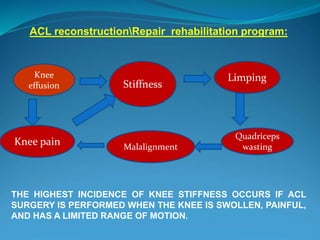
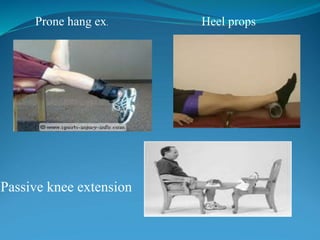
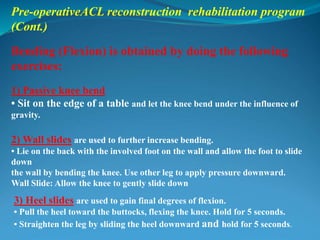
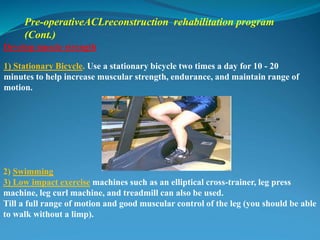
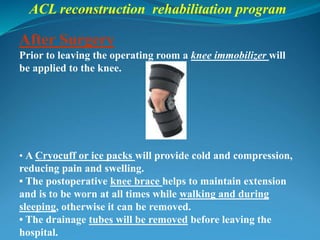
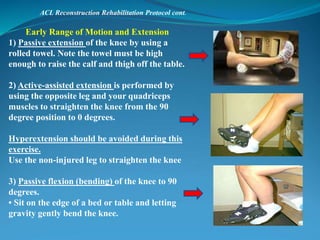
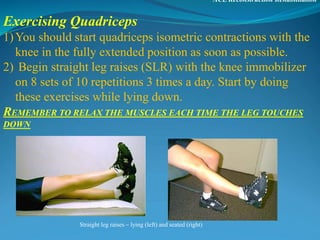
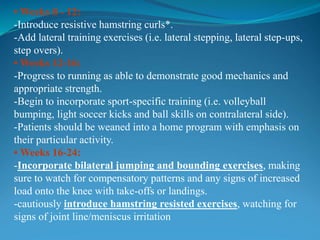
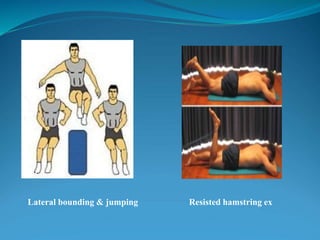
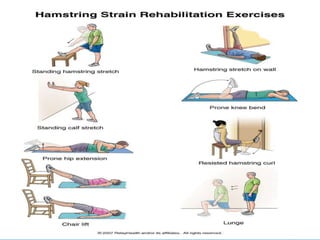
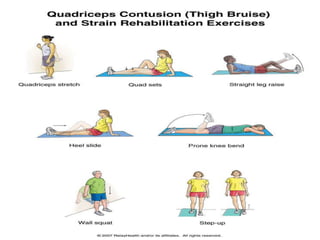
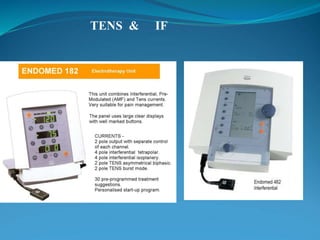
3. Rehabilitation programs for meniscus tears and ACL reconstruction are outlined, focusing on reducing pain, restoring range of motion and strength through exercises.