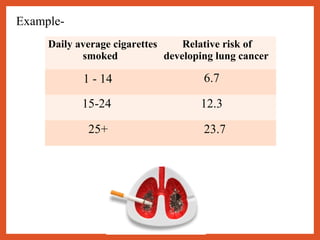
This document discusses criteria for determining causal association. It defines association and different types of association, including spurious, indirect, and direct causal association. Bradford Hill's criteria for making causal inferences are described, including strength of association, dose-response relationship, consistency of findings, biological plausibility, specificity of association, and temporal relationship. Examples for each criterion are provided, such as the relationship between smoking and lung cancer. The document concludes with a summary of association types and causal association criteria.











































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
