Call Girls In Andheri East Call 9920874524 Book Hot And Sexy Girls
037. osseous surgery
1. Jаffaя яaza Syзd
Osseous Surgery
“Procedures to modify bone support altered by periodontal disease, either by reshaping the
alveolar process to achieve physiologic form, without
removal of some alveolar bone, thus changing the
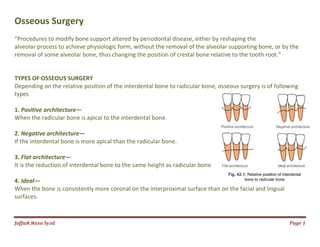
TYPES OF OSSEOUS SURGERY
Depending on the relative position of the interdental bone to
types
1. Positive architecture—
When the radicular bone is apical to the interdental bone.
2. Negative architecture—
If the interdental bone is more apical than the radicular bone.
3. Flat architecture—
It is the reduction of interdental bone to the same height as radicular bone.
4. Ideal—
When the bone is consistently more coronal on
surfaces.
altered by periodontal disease, either by reshaping the
alveolar process to achieve physiologic form, without the removal of the alveolar supporting bone, or by the
removal of some alveolar bone, thus changing the position of crestal bone relative to the tooth root.”
tion of the interdental bone to radicular bone, osseous surgery is
to the interdental bone.
apical than the radicular bone.
to the same height as radicular bone.
When the bone is consistently more coronal on the interproximal surface than on the facial and lingual
Page 1
altered by periodontal disease, either by reshaping the
supporting bone, or by the
position of crestal bone relative to the tooth root.”
radicular bone, osseous surgery is of following
the interproximal surface than on the facial and lingual
2. Jаffaя яaza Syзd Page 2
Osseous surgery can also be:
1. Additive—
Directed towards restoring the bone to original levels.
2. Subtractive—
It is designed to restore the form of the pre-existing alveolar bone to the level existing at the
time of surgery or slightly apical to this level.
Indications
1. One-walled angular defects.
2. Thick, bony margins.
3. Shallow crater formations.
Contraindications
1. Anatomic factors such as close proximity of the roots to the maxillary antrum or the ramus.
2. Age.
3. Systemic health.
4. Improper oral hygiene.
5. High caries index.
6. Extreme root sensitivity.
7. Advanced periodontitis.
8. Unacceptable esthetic result.
3. Jаffaя яaza Syзd
Instruments used
Hand instruments include:
1. Rongeurs-Friedman and Blumenthal.
2. Interproximal files—Schluger and Sugarman.
3. Back action chisels.
4. Oschsenbein chisels.
Rotary instruments include:
1. Carbide round burs.
2. Slow-speed handpiece.
3. Diamond burs.
Schluger and Sugarman.
Page 3
4. Jаffaя яaza Syзd
TECHNIQUE
The following steps are suggested:
1. Vertical grooving.
2. Radicular blending.
3. Flattening of interproximal bone.
4. Gradualizing marginal bone.
Not all the steps are necessary in each case.Not all the steps are necessary in each case.
Page 4
6. Jаffaя яaza Syзd Page 6
RECONSTRUCTIVE OSSEOUS SURGERY
periodontal therapy involves two primary components:
Elimination of bacterial plaque
Elimination of the anatomic defects produced by periodontitis.
two primary approaches to eliminating these anatomic defects—
resective and regenerative, both being surgical
The following reconstructive surgical techniques have been proposed.
1. Nongraft-associated new attachment.
2. Graft-associated new attachment .
3. Combination of both
7. Jаffaя яaza Syзd Page 7
Non graft-associated New Attachment
New attachment can be achieved without the use of grafts in:
a. Meticulously treated three-walled defects (Infrabony defect).
b. Perio-endodontal abscesses.
c. When the destructive procedure has occurred very rapidly, for example, after
treatment of pockets which had acute periodontal abscess.
8. Jаffaя яaza Syзd Page 8
Techniques
Removal of Junctional and Pocket Epithelium
The methods used to do so include:
i. Curettage—Only 50 percent of junctional epithelium and pocket epithelium can be
removed.
ii. Chemical agents—Mostly used in conjunction with curettage. The most commonly
used drugs are sodium sulfide, phenol, camphor, sodium hypochlorite and antiformin.
The main disadvantage is that the depth of action cannot be controlled.
iii. Ultrasonic methods—It is again not very useful, because of lack of clinicians tactile
sense while using these methods
9. Jаffaя яaza Syзd Page 9
iv. Surgical methods—
• Excisional new attachment procedure with internal bevel incision (ENAP).
• Gingivectomy procedure.
• Modified Widman flap.
• Coronal displacement of the flap.
10. Jаffaя яaza Syзd Page 10
Graft-associated New Attachment
Terminology
Graft
Xenograft or heterograft
Allograft or homograft
Autograft
Alloplastic graft
Osteoinduction:
A process by which the graft material is capable of promoting cementogenesis,
osteogenesis and new periodontal ligament.
Osteoconduction:
The graft material acts as a passive matrix, like a trellis or scaffolding for new bone to
cover.
11. Jаffaя яaza Syзd Page 11
Ideal Requirements of a Bone Graft Material
Biologic acceptability,
predictability,
clinical feasibility,
minimal postoperative hazards,
minimal postoperative sequelae,
good patient acceptance.
All grafting techniques require
presurgical scaling,
occlusal adjustment as needed and
exposure of defect with full thickness flap, best-suited is papilla preservation flap
13. Jаffaя яaza Syзd Page 13
Osseous coagulum:
a bur is used in the donor site to reduce it to small particles which when coated with blood
becomes coagulum and is placed in the defect until there is considerable excess and the flap is
replaced.
This technique uses small particles of donor bone and hence it provides additional surface area
for the interaction of cellular and vascular elements
Bone blend:
It uses an autoclaved plastic capsule and pestle.
Bone is removed from the predetermined site with chisels or rongeur forceps,
placed in the capsule with a few drops of saline,
triturated for sixty seconds to a workable plastic-like mass
packed into the bony defect.
14. Jаffaя яaza Syзd Page 14
Intraoral cancellous bone marrow chips:
It can be obtained from:
a. Maxillary tuberosity—
It contains good amount of cancellous bone with foci of red marrow and the bone is
removed with a cutting rongeur.
b. Edentulous areas—
The bone is removed with curette.
c. Healing sockets—
They are allowed to heal for eight to twelve weeks and the apical portion is utilized as donor
material.
15. Jаffaя яaza Syзd Page 15
Bone swaging:
This technique requires presence of an endentulous area adjacent to the defect from which the
bone is pushed into contact with root surface without fracturing the bone at its base
Bone from extraoral sites:
Iliac autografts/extraoral hip marrow:
The use of iliac cancellous bone marrow has shown good results in bony defects with varying
number of walls and furcation defects.
disadvantages associated with it.
i. Additional surgical trauma.
ii. Postoperative morbidity infection, exfoliation, sequestration.
iii. Root resorption.
iv. Rapid recurrence of the defect
16. Jаffaя яaza Syзd Page 16
Allografts:
Bone grafts are commercially available in tissue banks.
They can be:
1. FDBA (Freeze dried bone allograft)—
It is an osteoconductive material, varying results have been observed using this material.
Average bone fill of 50 percent has been reported.
2. DFDBA (Demineralized freeze dried bone allograft)—
Demineralization process exposes the components of bone matrix termed as bone morphogenic
protein, e.g. DemboneTM, which is a bone inductive protein isolated from the extracellular matrix
of human bones. Hence, this is an osteoinductive material
17. Jаffaя яaza Syзd Page 17
Xenografts:
They have been shown to cause severe immunologic reactions because of molecular divergencies,
therefore it is not used any longer
Alloplasts/non-bone graft material:
Non-bone graft materials have also been used for restoration of the periodontium.
Some of them are sclera, dura, cartilage, plaster of Paris, ceramics, and coral derived materials.
Lot of attention has been given to calcium phosphate ceramics which are of two types:
a. Hydroxyapatite—nonresorbable
b. Tricalcium phosphate—partially-bioresorbable.
18. Jаffaя яaza Syзd Page 18
Bioactive glass:
Consists of sodium and calcium salts, phosphates and silicon dioxide with particle size
ranging from 90 to 170 um (perioglas®) or 300 to 355 um (biogran®).
Coral-derived materials:
Two types of materials are available,
natural coral
coral-derived porous hydroxyapatite (both are proven to be biocompatible).
Combined techniques:
A combination of both graft and nongraft associated methods have been proposed, e.g.
combination of barrier techniques with bone grafts have been suggested by many authors.