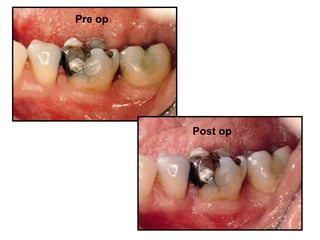
Bone grafts are materials used to replace or augment bone around teeth. They work through osteoconduction, osteoinduction, or osteogenesis. Common grafts used for periodontal defects include autografts obtained from the patient, allografts from other humans, xenografts from other species, and synthetic alloplasts. A graft is selected and placed into debrided periodontal defects to promote new bone formation and regeneration of lost tissues.